Page 1 of 16
CM16.1-2 | CM16.1-2 | Health Planning Concepts and Planning Cycle — SDL Guide
Learning Objectives
- Define health planning and explain its core principles
- Describe the six phases of the health planning cycle and their interrelationships
- Identify the role of monitoring and evaluation in the iterative planning process
- Apply the planning cycle framework to India's National Health Mission
INSTRUCTIONS
India's health system serves over 1.4 billion people across vast geographic and socioeconomic diversity. Without systematic planning, resources are misallocated, preventable diseases remain unaddressed, and health inequities widen. This module equips you with the conceptual framework of health planning and the practical tool of the planning cycle — the foundations underpinning every national health programme you will encounter in clinical and public health practice.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 27th ed. Ch: Health Planning and Management (textbook)
- Government of India. National Health Policy 2017. Ministry of Health and Family Welfare (policy)
- Government of India. National Health Mission Framework for Implementation 2012-17. MoHFW (report)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2014. A district health officer in a tribal block of Odisha receives a message: the local primary health centre has run out of anti-malarial drugs in the peak monsoon season. Thirty children under five are admitted with severe Plasmodium falciparum malaria. The drugs had been ordered, but the indent was filed six months late, the supply chain was not monitored, and there was no contingency plan. Three children die. The root cause is not a shortage of drugs in the state; it is a failure of planning. This module examines how systematic health planning — and the iterative cycle that sustains it — can prevent exactly this kind of catastrophe.
WHY THIS MATTERS
As a medical officer posted to a primary health centre or working in a district health system, you will be both a user and a contributor to health plans — from the facility's annual action plan to the district health society's programme implementation plan. Understanding the planning cycle allows you to identify where resources are being squandered, flag gaps in monitoring, and advocate for evidence-based priority setting. Every national programme — NHM, Ayushman Bharat, the tuberculosis elimination initiative — is built on the framework you are about to learn.
RECALL
Before we begin, recall from your earlier Community Medicine units: (1) the epidemiological transition — India is experiencing a dual burden of communicable diseases (TB, malaria, diarrhoeal diseases) alongside a rising tide of non-communicable diseases (cardiovascular disease, diabetes, cancer); (2) the three levels of health care in India — primary (sub-centres, PHCs), secondary (CHCs, district hospitals), and tertiary (medical college hospitals, AIIMS); and (3) the concept of disease burden — measured in DALYs or deaths — as the starting point for any needs assessment. These concepts form the evidence base upon which health planning begins.
The Burden of Unplanned Health Systems: Why Health Planning Matters
India's health landscape presents a paradox: a country with nuclear and space programmes that simultaneously has districts where children die of preventable diarrhoea. This paradox is, in large part, a planning failure. The burden of health inequity in India is immense — the NFHS-5 (2019-21) documents that under-5 mortality ranges from 12 per 1,000 live births in Kerala to 50 per 1,000 in Uttar Pradesh, a fourfold difference driven by differential investment, infrastructure, and programme quality. Without explicit planning, resources flow to visible urban hospitals while rural sub-centres remain understaffed. The National Health Accounts (2019-20) estimate that out-of-pocket expenditure constitutes approximately 48% of total health expenditure — a proportion that pushes an estimated 55 million Indians into poverty each year. These numbers are not inevitable; they reflect decades of under-planning at the primary care level.
Resource maldistribution is both a cause and a consequence of poor planning. A 2019 government assessment found that nearly 18% of sub-centres and 22% of PHCs across India were functioning below the Indian Public Health Standards (IPHS) norms for staffing. When there is no situation analysis phase to document this deficit, no priority-setting mechanism to allocate corrective resources, and no monitoring system to track progress, the deficit compounds over years. Health planning is therefore not an administrative luxury; it is the mechanism by which governments fulfil their constitutional commitment to the right to health.
Key population norms (IPHS 2022, for reference throughout this module):
- Sub-centre (SC): 1 per 5,000 population (plains); 1 per 3,000 (hilly/tribal)
- Primary Health Centre (PHC): 1 per 30,000 (plains); 1 per 20,000 (hilly/tribal)
- Community Health Centre (CHC): 1 per 1,20,000 (plains)
These norms are the benchmarks against which a situation analysis measures existing infrastructure — the first step of the planning cycle.
Determinants That Shape a Health Plan
A health plan does not emerge in a vacuum. It is shaped by a constellation of determinants that the planner must understand and account for, because ignoring any one of them undermines the plan's feasibility and sustainability. These determinants of health planning operate at multiple levels and interact in complex ways.
The epidemiological determinants set the need: the burden of disease (mortality, morbidity, DALYs), the distribution of risk factors (sanitation, nutrition, tobacco use), and the vulnerable populations most affected. The planner uses data from NFHS (National Family Health Survey), DLHS (District Level Household Survey), the HMIS (Health Management Information System), and special surveys such as the Annual Health Survey to characterise the epidemiological situation. Without this data, priority setting is guesswork.
The economic determinants define the envelope: the total health budget, its composition (central vs state vs local body contributions), the degree of external aid (donor funding for TB, HIV), and the opportunity cost of each rupee allocated. India's NHP 2017 set a target of raising government health expenditure to 2.5% of GDP by 2025 — the recognition that the prior level (~1.2% GDP) was structurally insufficient. Plans must be costed; uncosted plans are aspirations, not plans.
The political determinants shape priorities: political will for health equity, the electoral cycle (programmes with visible output before elections attract disproportionate funding), and inter-ministerial competition for budget. The shift from Five-Year Plans (Planning Commission era) to NITI Aayog's three-year action plans (2017 onward) reflects a political restructuring of how government-wide planning is coordinated.
The social and cultural determinants affect implementation: health-seeking behaviour, community trust in the health system, gender norms (women's access to care), literacy, and caste dynamics all influence whether a well-designed plan actually reaches its intended beneficiaries. A malaria bednet distribution programme that does not account for local sleeping practices will show high distribution numbers but low utilisation.
Finally, organisational and human resource determinants — staff availability, competency, motivation, and the management capacity of the district health administration — determine whether a plan can be executed at all. Plans that assume staffing levels 30% above what exists are plans for failure.
SELF-CHECK
India's NHP 2017 set a target for government health expenditure as a proportion of GDP. What was this target, and by which year?
A. 1.5% of GDP by 2020
B. 2.5% of GDP by 2025
C. 3.0% of GDP by 2030
D. 2.0% of GDP by 2022
Reveal Answer
Answer: B. 2.5% of GDP by 2025
The National Health Policy 2017 set a target of raising government health expenditure to 2.5% of GDP by 2025. At the time of the policy, India was spending approximately 1.15-1.2% of GDP on health — one of the lowest among comparable economies. The 2.5% target, while still below the WHO recommendation of 5%, represents a significant commitment to scaling public investment in health.
Defining Health Planning: Concepts and Core Principles
Health planning is formally defined (following Park) as 'an orderly process of defining community health problems, identifying unmet needs and surveying the resources available to meet them, establishing priority goals that are realistic and feasible, and projecting administrative action to accomplish the purpose of the proposed programme.' This definition contains several important elements: it is orderly (systematic, not reactive), it begins with problem definition (not solution prescription), it is resource-aware (feasibility is built in), and it is directed toward administrative action (it produces implementable outputs, not just recommendations).
Distinguishing health planning from general planning is useful: general planning may be applied to infrastructure, defence, or education, with different goal structures and stakeholder sets. Health planning is distinguished by its primary goal — improving population health outcomes — its unique data sources (epidemiological surveys, clinical registries, HMIS), and the normative commitments embedded in public health (equity, universal access).
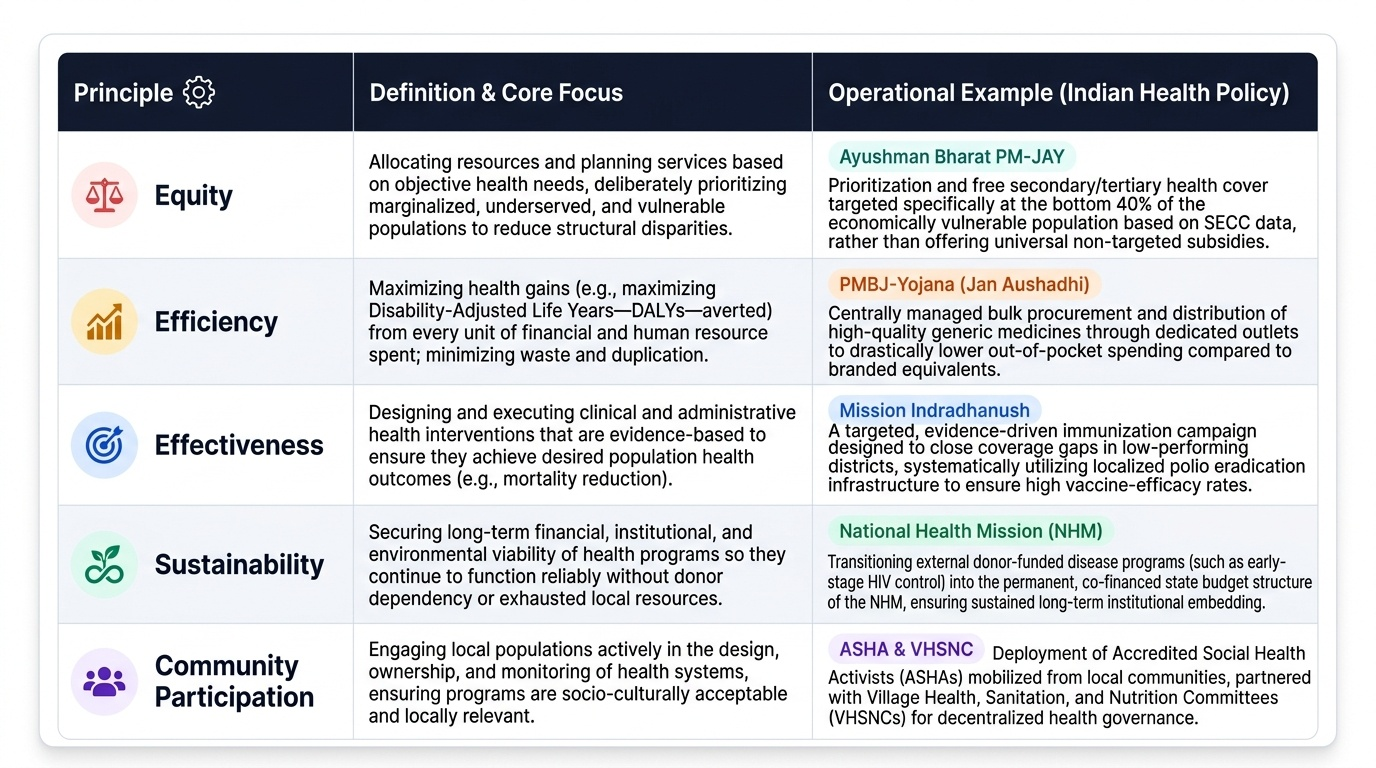
Core principles of health planning are the non-negotiable values that guide the process:
- Equity — resources and programmes must prioritise those with the greatest need and the least existing access. A plan that disproportionately benefits the urban, literate, or wealthy fails this principle.
- Efficiency — maximum health gain must be extracted from each rupee of expenditure. Cost-effectiveness analysis (comparing, e.g., cost per DALY averted) operationalises this principle.
- Effectiveness — interventions must actually achieve their stated health objectives. Evidence-based programming (using interventions proven in rigorous trials or strong observational data) operationalises this.
- Sustainability — the programme must be maintainable over time without continuous external inputs. Plans that depend entirely on donor funding for recurrent costs are structurally unsustainable.
- Community participation — the communities whose health is being planned for must be involved in needs assessment and priority setting. This improves relevance, ownership, and compliance.
- Intersectoral coordination — health is shaped by water, sanitation, food, education, and housing; effective planning involves sectors beyond the health ministry.
Provided image