Page 8 of 16
CM16.4-5 | CM16.4-5 | Health Policy, Planning and Economics in India — SDL Guide
Learning Objectives
- Describe the evolution of India's National Health Policies (NHP 1983, 2002, 2017) and their key targets and innovations
- Explain India's national health planning architecture — from Five-Year Plans to the NITI Aayog framework
- Define core health economics concepts: sources of financing, categories of expenditure, economic burden of disease, and efficiency in health systems
- Evaluate India's health financing performance and apply these concepts to Ayushman Bharat's design
INSTRUCTIONS
National health policy is the framework within which every district health plan is written, every programme is funded, and every facility is built or neglected. Health economics provides the analytical lens for understanding why resources flow where they do and how to make the case for better allocation. Together, these two domains explain why India's health system looks the way it does — and how it is being transformed. This SDL equips you to read, interpret, and critically engage with the policy documents and financing data that will shape your practice environment for the next three decades.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 27th ed. Ch: National Health Policies and Programmes (textbook)
- Government of India. National Health Policy 2017. Ministry of Health and Family Welfare (policy)
- Ministry of Health and Family Welfare. National Health Accounts 2019-20. New Delhi: National Health Systems Resource Centre, 2022 (report)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2004-05, a family in rural Rajasthan took their mother to a private nursing home for a hip fracture. The bill came to Rs. 42,000. Their annual household income was Rs. 38,000. They sold their cattle, borrowed from a moneylender at 24% annual interest, and spent three years repaying. The mother survived. The family was pushed below the poverty line. This is a textbook example of catastrophic health expenditure — defined as health costs exceeding 10-25% of household consumption — which affected an estimated 55 million Indians in 2011. The trajectory of India's national health policies, from NHP 1983 to Ayushman Bharat in 2018, is the story of a government progressively taking on responsibility for preventing exactly this outcome. This module tells that story — and provides the health economics framework to analyse how well it is working.
WHY THIS MATTERS
Understanding national health policies and health economics is not a purely academic exercise for the MBBS student. These policies determine: whether there is a functional PHC in the village where you will be posted; whether your patient can access free essential medicines under a state drug scheme; whether the government will reimburse hospitalisation for a patient who qualifies for PM-JAY; and whether the district health budget has been allocated to maternal health or to NCD management. Every prescribing and referral decision you make occurs within a policy and economics framework. Reading that framework critically allows you to advocate for your patients within the system — and to work toward improving it.
RECALL
Before beginning, recall from SDL 1 of this cluster: the planning cycle and the concept of situation analysis (Phase 1 — using data to characterise health burden and resource gaps). Recall also the IPHS infrastructure norms: SC 1:5,000, PHC 1:30,000, CHC 1:1,20,000. From SDL 2, recall the distinction between cost-effectiveness analysis (cost per health outcome unit), cost-benefit analysis (costs and benefits in money), and cost-utility analysis (cost per QALY). These concepts from earlier SDLs are now placed in the national policy and financing context.
The Burden That Drove National Health Policy: India's Pre-Reform Health Landscape
India's national health policy trajectory has been driven by the persistent gap between its public health ambitions and the reality of its population's health burden — a gap that has justified successive waves of policy reform. Understanding this burden context is essential for making sense of why each policy said what it said, and why each proved insufficient on its own.
At Independence in 1947, India faced an overwhelming communicable disease burden: smallpox, cholera, plague, malaria, tuberculosis, and diarrhoeal diseases dominated mortality and morbidity statistics. Life expectancy was approximately 32 years. Infant mortality exceeded 150 per 1,000 live births. The initial policy response was largely disease-control oriented — vertical programmes targeting specific infections — within the framework of the Planning Commission's Five-Year Plans.
By the 1980s and 1990s, India was experiencing what epidemiologists call the epidemiological transition: communicable diseases remained prevalent, but non-communicable diseases — cardiovascular disease, diabetes, cancer, chronic respiratory disease — were rising rapidly, creating a dual burden. The triple burden — communicable diseases + NCDs + injuries — characterises India's contemporary disease landscape. NFHS-5 (2019-21) data shows anaemia affecting 57% of women aged 15-49 (a communicable/nutritional deficiency indicator) in the same survey round that shows hypertension affecting 23% of men (an NCD indicator).
The financing burden has been equally compelling as a policy driver. India's out-of-pocket (OOP) expenditure as a share of total health expenditure was approximately 70-75% in the early 2000s — one of the highest in the world, reflecting a health system where public provision was chronically underfunded and the private sector filled the gap at full market price. The consequence: catastrophic health expenditure affecting millions of households annually, with health spending being a leading cause of household impoverishment. This financing landscape — not just the disease burden — is what made universal health coverage the central organising principle of NHP 2017.
Determinants of National Health Policy: What Shapes India's Policy Choices
India's health policies are not produced by technocratic calculation alone; they are shaped by a complex political economy of determinants that explain both what each policy prioritised and why implementation often fell short of intention. Recognising these determinants is as important as knowing the policy content.
The federal structure is the foundational political determinant: health is a State List subject under the Indian Constitution — meaning states have primary legislative and executive authority over health service delivery. The Union government operates through Centrally Sponsored Schemes (CSS) that co-fund state programmes (NHM, Ayushman Bharat) but cannot directly manage state health systems. The centre-state funding relationship (typically 60:40 for general states, 90:10 for special category/hilly states under NHM) shapes what national policies can actually mandate versus what they can only incentivise.
The fiscal determinant — how much money is available for health — is the binding constraint on policy ambition. India's chronic underinvestment in public health (approximately 1.15-1.2% of GDP in the pre-NHP 2017 period) was itself a policy choice made in competition with other priorities (defence, infrastructure, education). The decision to set the 2.5% GDP target in NHP 2017 reflected a fiscal-political consensus that the prior level was insufficient — but achieving that target requires sustained multi-year budget decisions across both central and state governments, each with their own fiscal constraints.
The epidemiological determinant shapes programme priorities: the disease profile of the 1970s-80s (predominantly communicable) drove the vertical programme era; the epidemiological transition forced the shift toward integrated primary care (Health and Wellness Centres) and insurance-based secondary/tertiary coverage (PM-JAY). Policy is always responding to a disease burden that has already evolved; the time lag between epidemiological reality and policy response is a persistent challenge.
The political economy determinant — the interests of organised constituencies — has shaped several key policy choices. Medical associations (IMA) have influenced the scope of task shifting allowed in official policy. The pharmaceutical industry has affected essential medicines list decisions. Private hospital associations have shaped the PM-JAY empanelment rate negotiations. Understanding that policy is made at the intersection of epidemiology, economics, and politics — not by epidemiology alone — is essential for critical policy analysis.
SELF-CHECK
India's Constitution places 'health' on which list, and what does this mean for national health policy implementation?
A. Union List — the central government directly manages all health facilities and programmes
B. State List — states have primary authority; the central government operates through Centrally Sponsored Schemes to co-fund and influence but not directly control state health systems
C. Concurrent List — both central and state governments share equal authority, requiring joint management of all programmes
D. Residuary List — health is managed by a separate constitutional body independent of both central and state governments
Reveal Answer
Answer: B. State List — states have primary authority; the central government operates through Centrally Sponsored Schemes to co-fund and influence but not directly control state health systems
Health is a State List subject under India's Seventh Schedule to the Constitution, meaning state governments have primary legislative and executive authority over health service delivery within their territories. The central government's primary mechanism for influencing state health systems is through Centrally Sponsored Schemes (CSS) — like NHM and Ayushman Bharat — where the centre provides most of the funding (typically 60% for general states) but states implement, hire staff, and manage facilities. This federal structure explains why implementation quality varies dramatically across states even when a single national policy is in place: state governments have the authority, but the centre holds most of the money.
Evolution of National Health Policies: NHP 1983, 2002, and 2017
India's three National Health Policies span 35 years of evolving health priorities, international commitments, and political-economic contexts. Each built on — and responded to the limitations of — its predecessor.
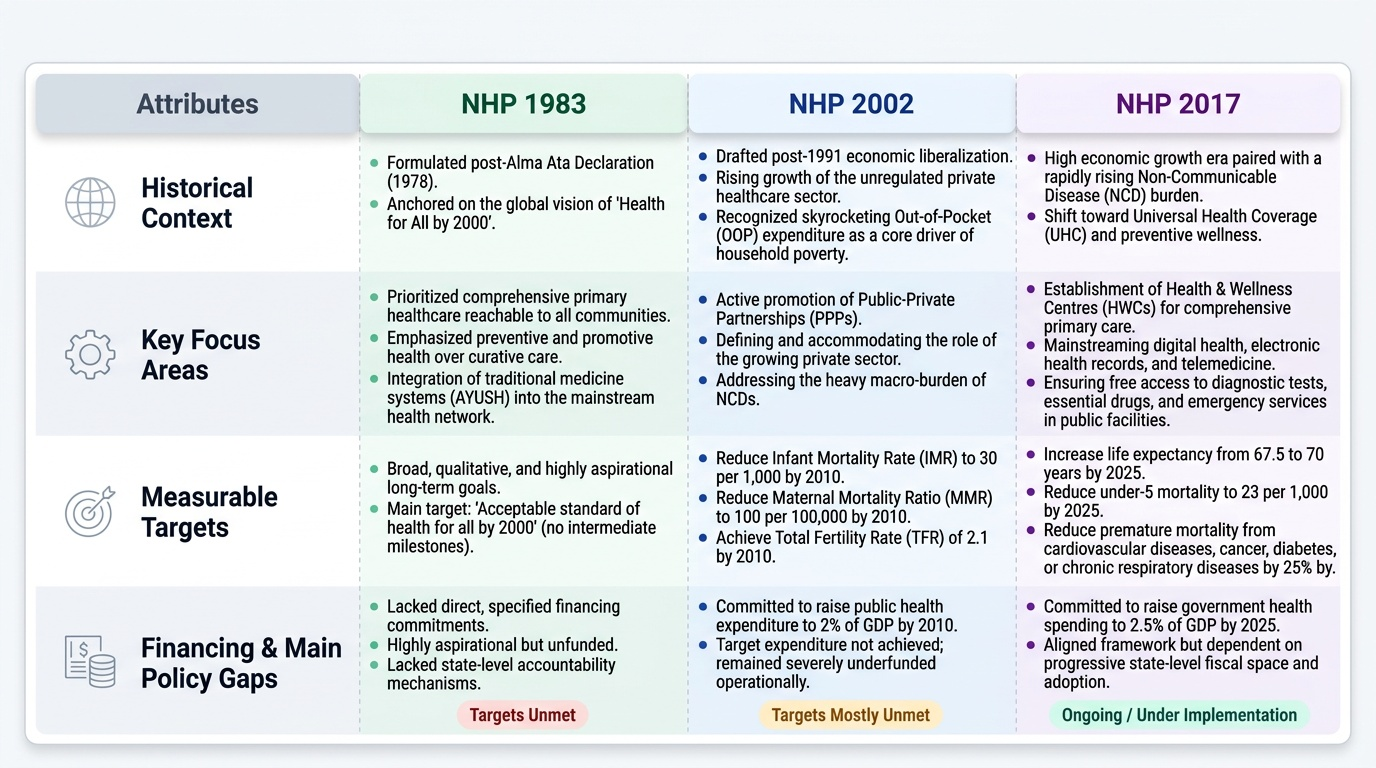
NHP 1983 was India's first comprehensive national health policy, developed in the context of the Alma Ata Declaration (1978) and its vision of 'Health for All by 2000.' Its central commitments were: (1) the development of a universal, comprehensive primary health care system reachable to all communities; (2) emphasis on preventive and promotive health over curative care; (3) integration of AYUSH (Ayurveda, Yoga, Unani, Siddha, Homeopathy) into the mainstream health system; and (4) a target to achieve an acceptable standard of health for all by 2000. NHP 1983 was aspirational but largely unfunded — it did not specify financing commitments or hold states accountable for targets. The 'Health for All by 2000' goal was not achieved.
NHP 2002 was formulated against the backdrop of India's economic liberalisation, rising private sector health care, and increasing recognition of OOP expenditure as a poverty driver. Its key features were: (1) setting measurable, time-bound targets for the first time — reducing IMR to 30/1,000, MMR to 100/1,00,000, TFR to 2.1, all by 2010; (2) acknowledging the growing role of the private sector and exploring public-private partnerships; (3) committing to raise health expenditure to 2% of GDP by 2010 (not achieved); and (4) addressing the emerging NCD burden. NHP 2002 was more operationally specific than 1983 but remained underfunded; its 2010 targets were largely not met.
NHP 2017 — the current policy — represents a fundamental shift in framing toward Universal Health Coverage (UHC): the goal of ensuring all people can access quality health services without financial hardship. Key commitments: (1) raise government health expenditure to 2.5% of GDP by 2025; (2) reduce out-of-pocket expenditure from approximately 65% to 25% of total health expenditure; (3) provide Health and Wellness Centres (1.5 lakh target) for comprehensive primary care; (4) implement PM-JAY for secondary/tertiary financial protection; (5) move toward health assurance — a guarantee of specific services — rather than only health insurance. NHP 2017 also set a 25-year vision for India's health system, moving beyond the 5-10 year time horizon of previous policies.
Provided image