Page 4 of 14
CM17.3-4 | CM17.3-4 | Primary Health Care and Health Policies — SDL Guide
Learning Objectives
- Define Primary Health Care (PHC) and describe its Alma-Ata 1978 definition
- List the 8 elements and 5 principles of PHC as defined at Alma-Ata
- Distinguish comprehensive PHC from selective PHC (GOBI-FFF)
- Describe India's National Health Policy 2017 and National Population Policy 2000 goals
- State the Millennium Development Goals and Sustainable Development Goals relevant to health
- Explain how PHC indicators are used to monitor health programme progress in India
INSTRUCTIONS
In 1978, at a conference in Alma-Ata (now Almaty, Kazakhstan), 134 nations declared that the existing approach to healthcare — expensive, hospital-based, curative-only — was failing the world's poorest populations. They issued a revolutionary call: 'Health for All by the year 2000,' grounded in a new framework called Primary Health Care. Nearly five decades later, PHC remains the organisational backbone of India's health system and the philosophical foundation of every national health policy from the National Health Policy to the Ayushman Bharat programme. Understanding PHC is not an academic formality — it is the conceptual map every medical officer must carry.
References
- Park's Textbook of Preventive & Social Medicine, 27th ed., Ch. 1 & 29 (Primary Health Care, Health Planning in India) (textbook)
- WHO/UNICEF Alma-Ata Declaration, 1978 (policy)
- National Health Policy 2017, Ministry of Health & Family Welfare, Government of India (policy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In the early 1970s, a WHO survey revealed a startling paradox: countries spending the most on healthcare were not achieving the best health outcomes. Infant mortality in low-income rural populations remained catastrophically high while hospital beds in capital cities sat underutilised. In response, the World Health Organization and UNICEF convened a historic conference at Alma-Ata in 1978. The delegation from India arrived with a country where 80% of the population lived in rural areas largely inaccessible to tertiary care — and left with a framework that would shape Indian health policy for the next half century. That framework was Primary Health Care, and its principles are at work every time an ASHA worker makes a home visit, every time a ANM conducts an antenatal check at a Sub-Centre, and every time a PHC medical officer prescribes from the essential medicines list.
WHY THIS MATTERS
NMC competencies CM17.3 and CM17.4 test your understanding of PHC as a concept and India's national health policies — knowledge directly applied in MBBS internship postings, NEET-PG theory papers, and your future role as a Medical Officer or District Health Officer. Postings at PHC and CHC are structured around PHC principles; the entire maternal and child health programme, the immunisation schedule, the ASHA/ANM/MPW cadre, and the essential medicines list all derive from PHC's 8 elements. Health policies examined here (NHP 2017, NPP 2000, MDGs, SDGs) set the targets by which your institution's performance will be measured.
RECALL
From the previous module (CM17.1–17.2), recall:
- Community health is the health status of a defined population, shaped by biological, behavioural, environmental, and socioeconomic determinants.
- The five components of healthcare — promotive, preventive, curative, rehabilitative, palliative — must all be accessible for care to be comprehensive.
- Community diagnosis uses epidemiological data to identify health problems in a population — the same data that PHC programmes use to define their priorities.
PHC provides the organisational and philosophical framework for DELIVERING these five components at scale.
The Global Burden That Drove the Alma-Ata Declaration
By the late 1970s, the global health landscape revealed a deeply inequitable distribution of illness and death. The vast majority of preventable deaths — from communicable diseases, malnutrition, unsafe childbirth, and contaminated water — were concentrated among the world's poorest rural populations who had no meaningful access to conventional healthcare. Conventional healthcare at the time was predominantly hospital-based, curative-oriented, physician-centric, and unaffordably expensive for most of the developing world. There was a growing recognition, led by WHO and UNICEF, that this model was fundamentally mismatched to the burden of disease it was supposed to address.
The core problem identified was not merely a shortage of hospitals or doctors — it was a structural mismatch between health system design and the social, environmental, and economic determinants driving the majority of the disease burden. Children were dying of diarrhoea from contaminated water, not from diseases that required specialist care. Mothers were dying in childbirth from preventable complications, not from conditions requiring complex surgery. Malaria, tuberculosis, and malnutrition — conditions amenable to simple, low-cost interventions — were responsible for the greatest losses of life and productivity.
This recognition led to a fundamental reorientation: if the majority of health problems have social, environmental, and economic roots, then the health system must engage with those roots — through community education, sanitation, nutrition, and accessible first-contact care. This was the intellectual foundation that the Alma-Ata conference crystallised into the PHC framework in 1978.
The magnitude of the burden also revealed a justice argument: inequitable access to health was not inevitable — it was a consequence of policy choices and resource allocation. The Alma-Ata Declaration was explicit that health inequity was both preventable and morally unacceptable, making health equity a political commitment, not merely a technical aspiration.
Primary Health Care — Alma-Ata 1978: Definition, Elements, and Principles
The Alma-Ata Declaration of 1978, jointly convened by WHO and UNICEF, defined Primary Health Care (PHC) as:
> 'Essential health care based on practical, scientifically sound and socially acceptable methods and technology, made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford to maintain at every stage of development in the spirit of self-reliance and self-determination.'
This definition has four essential elements embedded in it: (1) it is essential care — covering the basic health needs, not every possible intervention; (2) it uses appropriate technology — scientifically valid and locally feasible; (3) it is universally accessible — geographic, financial, and cultural barriers must be eliminated; (4) it requires community participation — communities are not passive recipients but active agents.
The 8 elements of PHC (mnemonics vary; Park uses these categories):
1. Education on prevailing health problems and methods of prevention and control
2. Nutritional promotion including food supply promotion
3. Safe water supply and basic sanitation
4. Maternal and child health (MCH), including family planning
5. Immunisation against major infectious diseases
6. Prevention and control of locally endemic diseases
7. Appropriate treatment of common diseases and injuries
8. Provision of essential drugs
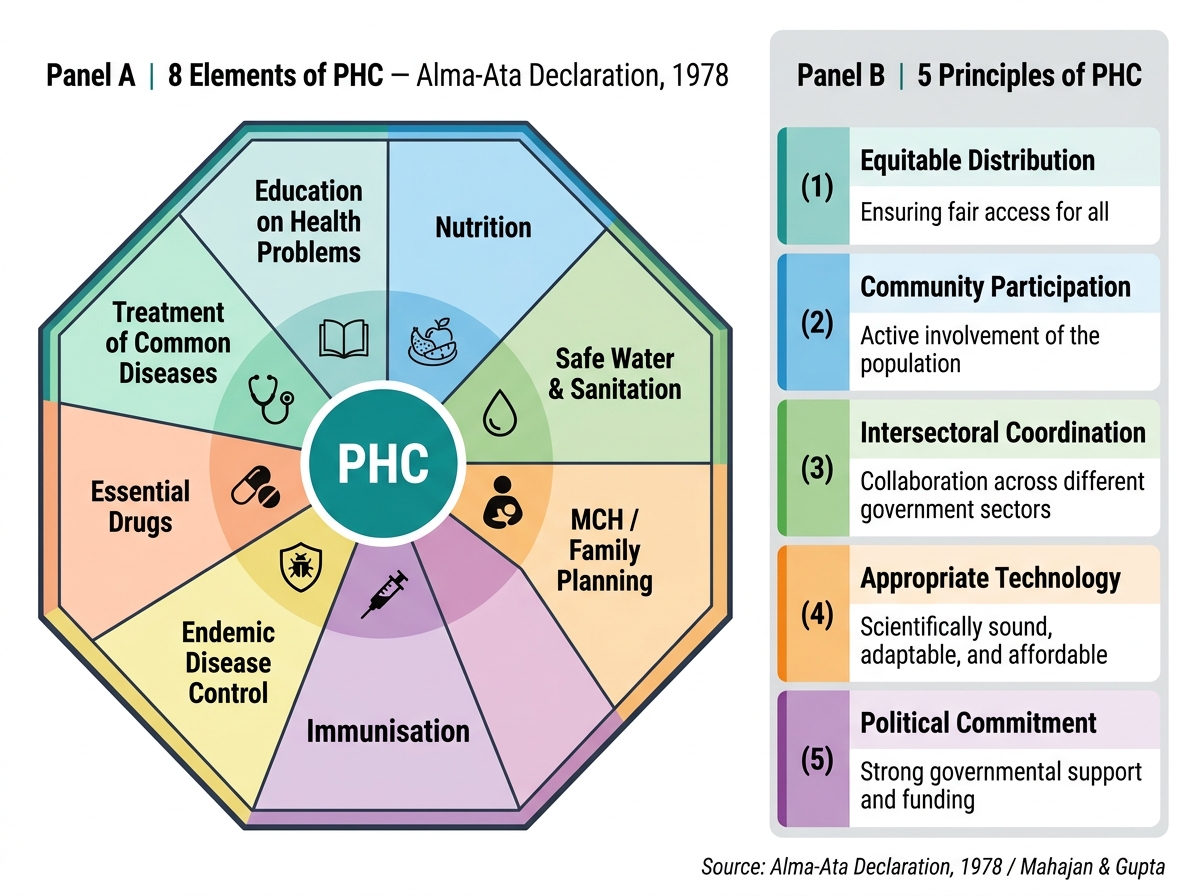
Elements and Principles of Primary Health Care — Alma-Ata Declaration, 1978
The 5 principles of PHC (operationalising the definition):
1. Equitable distribution — services must reach the underserved, not concentrate in cities
2. Community participation — communities plan, implement, and evaluate their own health care
3. Intersectoral coordination — health outcomes require action by agriculture, education, water, housing sectors
4. Appropriate technology — interventions must be scientifically valid, locally acceptable, and affordable
5. Political commitment (sometimes stated as 'political will') — governments must prioritise and resource PHC
These principles explain why PHC cannot be delivered by the health sector alone — and why India's NRHM/Ayushman Bharat programmes involve ICDS, Panchayati Raj, and the rural development ministry alongside the health ministry.
SELF-CHECK
The Alma-Ata Declaration defines PHC as 'essential health care made universally accessible at a cost the community and country can afford.' Which of the following actions BEST embodies the principle of 'appropriate technology' in this context?
A. Establishing a CT scanner at every PHC to improve diagnostic accuracy
B. Training ASHAs to use Oral Rehydration Solution for diarrhoeal disease management in villages
C. Deploying telemedicine only in urban hospitals where internet connectivity is reliable
D. Restricting immunisation to tertiary care hospitals to ensure cold-chain integrity
Reveal Answer
Answer: B. Training ASHAs to use Oral Rehydration Solution for diarrhoeal disease management in villages
Appropriate technology in PHC means interventions that are scientifically valid, locally feasible, culturally acceptable, and affordable — not necessarily the most advanced technology available. Training ASHAs to prepare and distribute ORS for diarrhoeal disease management is the textbook example: ORS is evidence-based, requires no electricity or complex equipment, is affordable, and can be deployed at village level by a community health worker. CT scanners at every PHC would be prohibitively expensive and technically unsustainable — violating the 'cost the community can afford' criterion.
Comprehensive vs Selective PHC and India's Adaptation
Following the Alma-Ata Declaration, a practical debate emerged: was comprehensive PHC — addressing all 8 elements simultaneously — feasible in resource-constrained settings? In 1979, Walsh and Warren proposed Selective PHC: focusing resources on a few high-impact, cost-effective interventions rather than the full PHC spectrum. This led to the GOBI-FFF strategy:
- Growth monitoring (to detect malnutrition)
- Oral rehydration salts (for diarrhoeal disease)
- Breastfeeding promotion
- Immunisation (EPI — Expanded Programme on Immunisation)
- Female education
- Food supplementation
- Family planning
Critics of selective PHC argued that it fragmented healthcare and ignored the social determinants that comprehensive PHC was designed to address. India largely chose a hybrid approach: implementing national vertical programmes (National Tuberculosis Programme, Universal Immunisation Programme, RCH Programme) that resemble selective PHC, while the PHC infrastructure and community health worker cadre (ASHAs, ANMs, MPWs) deliver the broader comprehensive PHC elements.
India's PHC delivery structure translates the Alma-Ata framework into a three-tier system:
- Sub-Centre: staffed by ANM and Male Health Worker (MPW); serves 3,000–5,000 (plains) or 1,000–3,000 (tribal/hilly) population; first contact for MCH, immunisation, basic curative care
- Primary Health Centre (PHC): doctor-led; serves 20,000–30,000 (plains) or 12,000–20,000 (tribal/hilly); OPD, inpatient (6 beds), laboratory, referral
- Community Health Centre (CHC): specialist-led (4 specialists: surgeon, physician, gynaecologist, paediatrician); serves 80,000–1,20,000; 30 beds, OT, X-ray
ASHAs (Accredited Social Health Activists) are the community link workers connecting households to the Sub-Centre and PHC — a direct operationalisation of Alma-Ata's community participation principle. One ASHA per 1,000 population in rural areas is the norm.