Page 8 of 14
CM17.5-6 | CM17.5-6 | Healthcare Delivery and Health System Functioning — SDL Guide (Part 2)
The WHO Health System Building Blocks — Applying the Framework to India
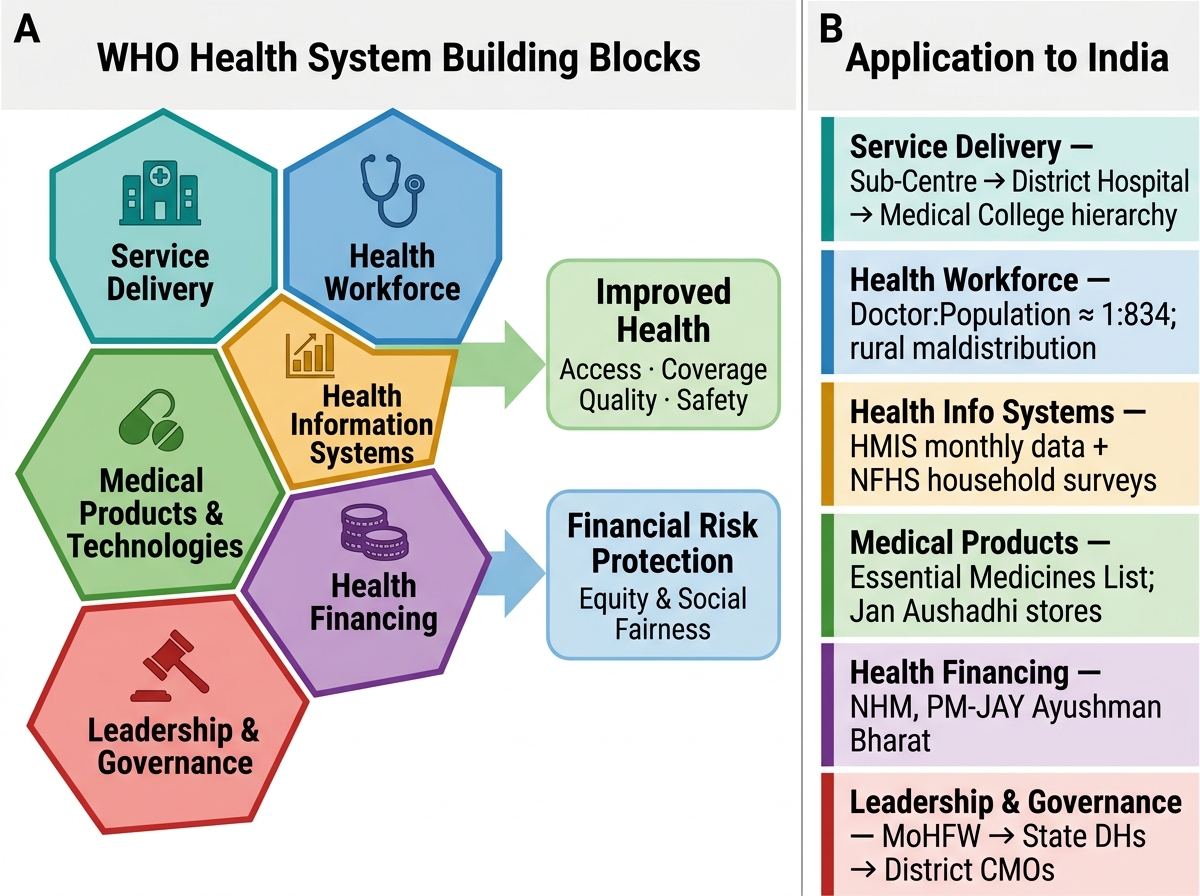
In 2007, the World Health Organization published a framework for health system strengthening based on six building blocks — the essential functional components that any health system must have to deliver good health outcomes and financial risk protection. This framework is the analytical tool used by health system researchers, policymakers, and programme evaluators worldwide.
WHO Health System Building Blocks and Their Application to India
The six building blocks and their application to India:
- Service delivery: The availability, coverage, quality, and equity of health services. India's multi-tier hierarchy (Sub-Centre to Medical College) is the structural expression of this building block. Key gaps: CHC specialist shortfalls, urban-rural inequity, quality deficits at peripheral levels.
- Health workforce: The numbers, skills, distribution, and performance of all health workers. India has a doctor-population ratio of approximately 1:834 (Medical Council data including AYUSH) — meeting the WHO benchmark of 1:1,000, but with severe urban-rural maldistribution: most doctors are in cities; many rural PHCs remain single-officer or vacant. Specialist shortfalls at CHC level (surgeon, anaesthetist, gynaecologist) remain a persistent challenge.
- Health information systems: Data collection, analysis, and use for decision-making. India's HMIS collects monthly data from PHC to national level; NFHS provides household-level data every 4–5 years; the Civil Registration System (CRS) covers vital events. Gaps: completeness and timeliness of facility-level data; verbal autopsy to determine cause of death in areas with poor CRS coverage.
- Medical products, vaccines, and technologies: Availability, quality, and rational use of medicines, vaccines, equipment, and diagnostics. The Essential Medicines List (EML) and the National Essential Diagnostics List (NEDL) operationalise this building block. Gaps: drug stock-outs at PHC/CHC level are common; cold chain maintenance for immunisation remains patchy in remote areas.
- Health financing: Revenue collection, pooling, and purchasing of health services. India's out-of-pocket expenditure (~47–50% of total health expenditure) is the most critical failure in this building block. Government expenditure at ~1.5% of GDP is insufficient. Ayushman Bharat–Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) is India's attempt at demand-side financing to reduce OOP for secondary and tertiary care.
- Leadership and governance: Policy frameworks, accountability, regulation, and intersectoral coordination. India's fragmented federal health governance (health is a state subject; national government sets policies but states implement) creates both flexibility and inconsistency. The National Health Mission provides a convergent platform, but accountability for outputs (IMR reduction, institutional delivery) varies widely by state.
SELF-CHECK
A district PHC reports persistent stock-outs of cotrimoxazole and ORS for the past two months, causing patients to purchase medicines from private pharmacies at personal expense. Which WHO health system building block is MOST directly failing in this scenario?
A. Service delivery
B. Health workforce
C. Medical products, vaccines, and technologies
D. Health financing
Reveal Answer
Answer: C. Medical products, vaccines, and technologies
A persistent drug stock-out at a PHC — forcing patients to purchase essential medicines out-of-pocket — is a direct failure of the 'medical products, vaccines, and technologies' building block. This building block covers the availability, quality, and rational use of medicines and diagnostics. Stock-outs indicate failures in procurement, supply chain management, or distribution — all within this domain. While the consequent out-of-pocket expense also affects the 'health financing' building block, the primary failure is in medical products supply — without available medicines, even well-funded and well-staffed facilities cannot deliver effective service.
Evaluating Health System Functioning — Indicators and India's Gaps
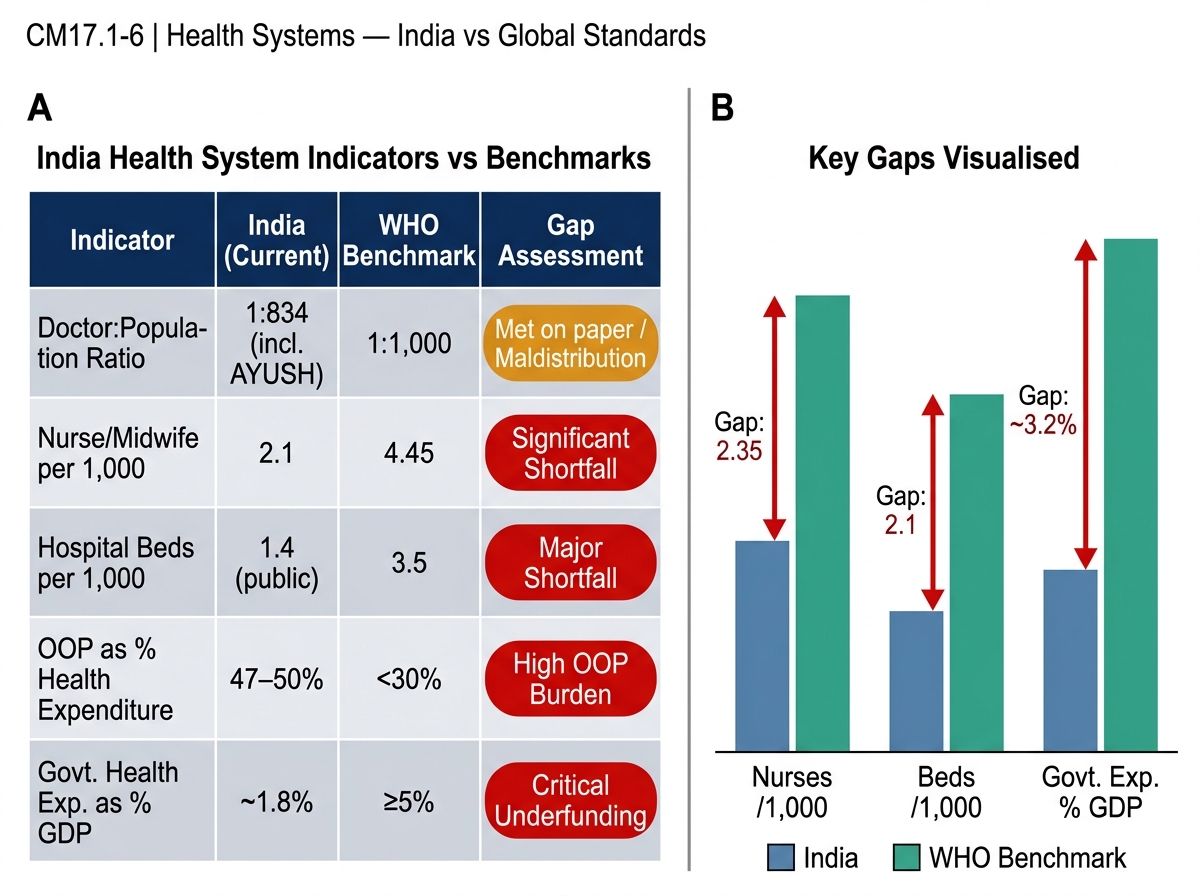
Health system functioning is evaluated by comparing actual system performance against established benchmarks. The WHO, NHP 2017, and IPHS standards provide reference values against which India's current performance can be assessed.
India Health System Indicators vs WHO Benchmarks
| Indicator | India Current | WHO Benchmark | NHP 2017 Target | Gap Assessment |
|---|---|---|---|---|
| Doctor : population ratio | 1:834 (incl. AYUSH) | 1:1,000 | — | Met on paper; severe urban-rural maldistribution |
| Nurse/midwife : population | ~2.1/1,000 | 4.45/1,000 | — | Significant shortfall |
| Hospital beds / 1,000 pop. | ~1.4 (public) | 3.5 | — | Major shortfall in public beds |
| OOP as % total health exp. | ~47–50% | <15–20% | Reduce to 25% | Critically high |
| Govt. health exp. / GDP | ~1.5% | 5–6% (high-income) | 2.5% | Major underfunding |
| CHC specialist vacancy rate | ~70–80% positions vacant | 0% vacancy | Fully staffed | Critical gap |
Interpreting the gaps:
The doctor-population ratio meeting WHO benchmarks on aggregate masks a critical distributional problem: India produces approximately 75,000 MBBS graduates per year, but the majority of rural PHCs and CHCs face severe doctor shortages because most graduates choose urban private practice. This is a health workforce building block failure of distribution and incentive alignment, not a failure of production volume.
The 70–80% CHC specialist vacancy rate (Rural Health Statistics 2023) means that the First Referral Unit function — the lynchpin of the PHC referral chain — is systematically non-functional across large swathes of India. Obstetric emergencies, surgical emergencies, and complicated paediatric cases cannot be managed at the tier designed for them, forcing patients to bypass CHC and PHC for district and private hospitals, creating financial catastrophe.
The 47–50% OOP rate is the single most consequential health system failure in India. Every other building block weakness ultimately manifests as financial catastrophe for the patient who must pay privately for medicines, investigations, or specialist care that should have been available publicly at no cost.
Reform responses: Ayushman Bharat–Health and Wellness Centres (AB-HWC) are upgrading PHCs and Sub-Centres into comprehensive primary care platforms with expanded essential medicines, diagnostics, and telemedicine. AB-PMJAY (PM Jan Arogya Yojana) provides insurance coverage of Rs 5 lakh per family per year for secondary/tertiary hospitalisation — addressing the OOP gap at the hospital care end.
CLINICAL PEARL
Pearl: The bypass behaviour trap. When a CHC lacks specialists and a PHC has drug stock-outs, rational patients bypass both and go directly to district hospitals or private facilities — incurring catastrophic OOP costs. Health system analysts call this 'bypassing' and it creates a vicious cycle: peripheral facilities appear underutilised (justifying budget cuts); district and tertiary hospitals become overcrowded; OOP expenditure rises. The solution is not to discourage bypassing — it is to fix the peripheral level so bypassing is no longer necessary. Whenever you see an empty Sub-Centre or PHC, the right question is: 'Why would a rational patient come here?' That diagnostic question is the WHO building blocks framework applied in practice.
Applying Health System Knowledge — A Referral Scenario
Trace the following scenario through India's health delivery hierarchy and identify the system failure points using the WHO building blocks framework.
Scenario: Sumitra, a 22-year-old primigravida in her 39th week of pregnancy, develops obstructed labour at 11 PM in a village in rural Jharkhand. Her ASHA, Rukmini, identifies the danger sign and mobilises the family. The Sub-Centre ANM is available but cannot manage obstructed labour. She calls the PHC doctor for referral — the ambulance (108 service) takes 45 minutes to arrive. The PHC doctor provides IV fluids, oxytocin management, and immediately refers to CHC. At the CHC, the regular gynaecologist post has been vacant for 4 months; only an MBBS general duty MO is present who is not trained for operative delivery. He refers immediately to the District Hospital — 60 kilometres away. Sumitra arrives at the District Hospital 3.5 hours after the obstructed labour was identified. Emergency caesarean section is performed. The baby survives. Sumitra develops uterine rupture and requires blood transfusion — blood is available at the District Hospital. She survives, but requires 10-day hospitalisation. The family's total out-of-pocket cost: Rs 45,000 (ambulance, blood, medicines not available in district hospital pharmacy).
Health system failure analysis:
| Failure Point | WHO Building Block | Level of Delivery System |
|---|---|---|
| CHC gynaecologist vacancy (4 months) | Health workforce | CHC — First Referral Unit failure |
| CHC not functioning as FRU | Service delivery | CHC |
| 45-min ambulance wait | Service delivery (emergency transport) | Sub-Centre/PHC area |
| Medicines OOP at District Hospital | Medical products | District Hospital |
| Rs 45,000 OOP cost | Health financing | System-wide |
What worked: ASHA recognition of danger sign (community participation), PHC immediate referral (appropriate decision-making), 108 ambulance system (JSY/LSAS-linked transport), blood availability at District Hospital, competent emergency surgery at tertiary level.
This scenario illustrates that health system functioning is not binary — it partially works, partially fails. The WHO building blocks framework allows a structured analysis of which components need strengthening. For a medical officer or DHO, this analysis translates directly into an action plan: fill the CHC specialist vacancy (building block 2), maintain drug stocks (building block 4), maximise JSY financial protection (building block 5).
SELF-CHECK
India's doctor-population ratio meets the WHO benchmark of 1:1,000 when AYUSH practitioners are included — yet rural PHCs report severe doctor shortages. Which health system building block analysis BEST explains this paradox?
A. The medical products building block — there are insufficient drugs to attract doctors to rural areas
B. The health workforce building block — adequate total numbers mask severe urban-rural maldistribution and incentive misalignment
C. The health financing building block — rural patients cannot afford to pay private doctors
D. The leadership and governance building block — the government has not issued a rural posting policy
Reveal Answer
Answer: B. The health workforce building block — adequate total numbers mask severe urban-rural maldistribution and incentive misalignment
The health workforce building block addresses not only total numbers of health workers, but their distribution, skills, performance, and the policy environment that governs where they work. India's doctor-population ratio appearing adequate on aggregate masks a critical maldistribution: the majority of doctors are urban, private-sector practitioners, while rural government positions remain unfilled. This is a workforce distribution and incentive alignment failure — not a production failure. The building blocks framework requires analysis at this level of specificity to design effective interventions (rural service incentives, compulsory rural posting, telemedicine, task-shifting to trained nurses).