Page 1 of 8
CM14.1-4 | CM14.1-4 | Hospital Waste Classification, Treatment, Law and Segregation — SDL Guide
Learning Objectives
- Define hospital (biomedical) waste and distinguish it from general solid waste
- Classify hospital waste using the BMW Rules 2016 four-category colour-code system
- Describe the treatment method appropriate for each waste category
- Outline the legal framework and stakeholder duties under the Biomedical Waste Management Rules 2016
- Demonstrate correct segregation of given waste items into the appropriate colour-coded container
INSTRUCTIONS
Healthcare workers who mishandle biomedical waste expose patients, colleagues, and the community to preventable infection and toxic harm. This module equips you to classify, segregate, treat, and legally manage hospital waste in compliance with India's Biomedical Waste Management Rules 2016 — a skill you will exercise every clinical day for the rest of your career.
References
- Park's Textbook of Preventive and Social Medicine, 25th ed — Ch. 19 (Environment and Health: Waste Management) (textbook)
- Biomedical Waste Management Rules 2016 (Ministry of Environment, Forest and Climate Change, India) (regulation)
- WHO Safe Management of Wastes from Health-Care Activities, 2nd ed, 2014 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are finishing a night shift in the surgical ward. A nurse inadvertently discards a used needle into the general municipal waste bin. The sanitation worker, unaware of the contents, reaches in bare-handed and sustains a needle-stick injury. Within hours, the needle-stick triggers a post-exposure prophylaxis cascade — blood tests, antiretrovirals, anxious counselling sessions. All of this was preventable by one act: placing that needle in the correct white puncture-proof container. Hospital waste is not merely a logistical nuisance. It is a patient-safety, occupational-safety, and environmental-safety matter, governed by law.
WHY THIS MATTERS
Every year, Indian hospitals generate an estimated 600 tonnes of biomedical waste per day (Park, 25th ed). A significant fraction is infectious — contaminated with blood-borne pathogens, drug-resistant organisms, or cytotoxic chemicals. When improperly discarded, this waste becomes a source of healthcare-associated infections (HAIs), needle-stick injuries to sanitation staff, and soil/water contamination in surrounding communities. As a future doctor, you will generate biomedical waste with every procedure you perform. Knowing what goes in which bag, which treatment method is mandated, and what the law requires is not optional — it is a clinical and legal duty. The NMC CBME curriculum places CM14.1–CM14.4 in Year 3 precisely because by this stage you have seen enough clinical procedures to contextualise the waste they produce.
RECALL
Before we classify hospital waste, recall two foundational ideas from your earlier years:
Infection transmission routes (Microbiology, Year 1): Blood-borne pathogens — HIV, Hepatitis B, Hepatitis C — spread through contaminated sharps and body fluids. Hospital waste containing these materials is therefore a fomite and must be treated as such.
Cytotoxic agents (Biochemistry/Pharmacology): Many drugs used in oncology are cytotoxic — they damage DNA. Waste containing these agents cannot simply be incinerated in a standard incinerator; it requires a high-temperature incinerator or plasma pyrolysis to ensure complete destruction without toxic exhaust. These two prior concepts explain why the colour-code system differentiates waste not just by type but by risk level.
Burden and Magnitude of Hospital Waste
Understanding the scale of the problem motivates safe practice. India's healthcare sector — comprising over 50,000 hospitals, 1.5 million hospital beds, and millions of smaller clinics and diagnostic laboratories — produces an estimated 600 tonnes of biomedical waste per day (Park's Preventive and Social Medicine, 25th ed). Of this, roughly 15–20% is classified as infectious or hazardous; the remainder is general waste that, if properly segregated, can enter the municipal waste stream without special treatment.
Healthcare-associated infections (HAIs) are among the most direct consequences of poor waste management. The WHO estimates that in low-to-middle-income countries, 10–15% of hospitalised patients acquire an HAI, and contaminated waste — particularly improperly disposed sharps — is a recognised transmission vector. Needle-stick injuries alone account for approximately 100,000 blood-borne pathogen exposures among healthcare workers globally each year.
Beyond the hospital perimeter, improperly managed biomedical waste contaminates groundwater (leaching from open dumps), generates toxic dioxins and furans when burned in low-temperature open fires, and creates entry points for scavengers — both human (rag-pickers at dumpsites) and animal (dogs, birds). Understanding that hospital waste has both an internal burden (HAIs, occupational injury) and an external burden (community and environmental harm) frames why India enacted the BMW Rules 2016 — the central regulation governing this module.
SELF-CHECK
A district hospital discharges 600 kg of waste per day. What fraction of this is typically classified as infectious or hazardous biomedical waste according to Park?
A. 50–60%
B. 15–20%
C. 5% or less
D. All of it, because it comes from a hospital
Reveal Answer
Answer: B. 15–20%
Park's Textbook states approximately 15–20% of hospital waste is infectious or hazardous. The majority (80–85%) is general waste (paper, food, packaging) that, if kept uncontaminated through segregation at source, can enter the municipal waste stream. This distinction makes source segregation — keeping hazardous and general waste physically separate — the single highest-impact intervention in hospital waste management.
Classification of Hospital Waste: The BMW Rules 2016 Colour-Code System
The Biomedical Waste Management Rules 2016 (BMW Rules 2016), enacted under the Environment Protection Act 1986, introduced a simplified colour-code system replacing the earlier nine-category Schedule I of the BMW Rules 1998. The 2016 rules classify biomedical waste into four colour-coded streams, each requiring a specific container type and treatment pathway. This classification system is the operationalised answer to CM14.1 and CM14.4.
The four colour categories are:
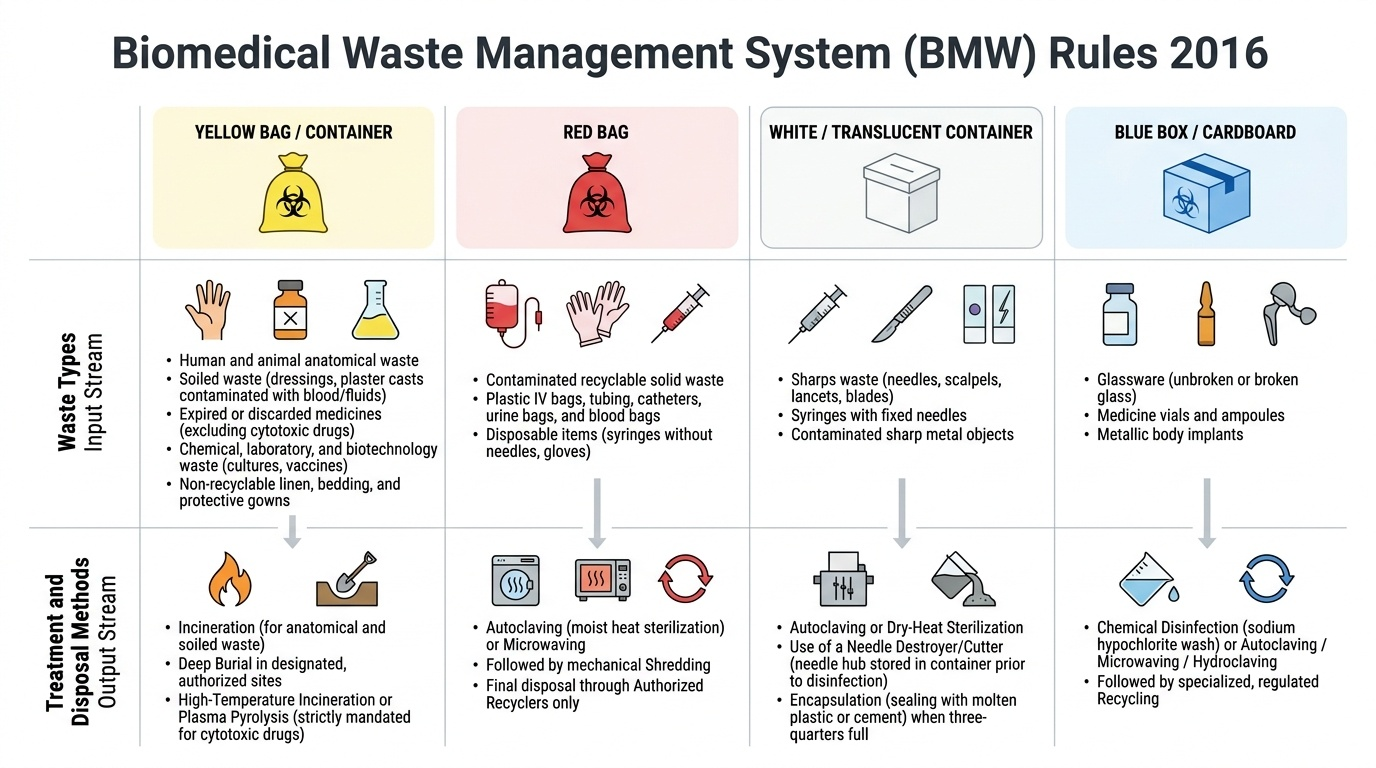
1. Yellow bag / container — The largest and most hazardous category. Includes: human anatomical waste (organs, tissues, body parts); animal anatomical waste from veterinary hospitals; soiled waste (dressings, bandages, plaster casts contaminated with blood or body fluids); expired or discarded medicines other than cytotoxic drugs; chemical waste including disinfectants and lab chemicals; discarded linen, bedding, and gowns that are not recyclable; and microbiology/biotechnology laboratory waste (cultures, stocks, vaccines). Treatment: incineration (for anatomical and cytotoxic-adjacent waste) or deep burial in a designated biomedical waste treatment site. Cytotoxic drugs specifically require high-temperature incineration or plasma pyrolysis.
2. Red bag — Contaminated recyclable solid waste that can be processed back into raw material after disinfection. Includes: plastic IV tubing and bags, catheters, urine bags, blood bags, syringes WITHOUT needles (needle separated into white container), gloves, and other plastic disposable items contaminated with blood or body fluids. Treatment: autoclaving (moist heat sterilisation) or microwave treatment followed by shredding and recycling through an authorised recycler.
3. White/translucent puncture-proof container — The sharps stream. Includes: needles (with or without syringe), lancets, scalpel blades, glass slides if broken and contaminated, surgical wire, and any sharp object that has contacted the patient or infected material. Treatment: autoclaving, dry-heat sterilisation, or for needles specifically — a needle destroyer/cutter with the hub stored in the container, then autoclaving. When the container is three-quarters full it is sealed and sent for treatment. Encapsulation (pouring molten plastic or cement into the container) is an alternative final-disposal step in some settings.
4. Blue cardboard box with blue plastic bag — Glassware and metallic implants. Includes: discarded laboratory glassware (flasks, test tubes, pipettes) that is unbroken or is broken but non-contaminated; metallic body implants removed during surgery (plates, screws, prostheses). Treatment: disinfection (chemical or autoclaving) followed by disposal through an authorised metal recycler. Contaminated broken glass goes into the white puncture-proof container instead.
A fifth informal stream — general/municipal solid waste (food waste, packaging, newspapers, uncontaminated disposable cups) — does not carry a biomedical colour code and enters the municipal waste chain. The critical skill is ensuring general waste is never co-mingled with biomedical waste before collection.
Provided image
| Category | Colour code | Waste types (examples) | Treatment |
|---|---|---|---|
| Anatomical/pathological, chemical, discarded medicines | Yellow bag/container | Organs, soiled dressings, expired drugs, lab cultures | Incineration; deep burial |
| Contaminated recyclable plastics | Red bag | IV bags, tubing, gloves (no sharps) | Autoclave → shred → recycle |
| Sharps | White/translucent puncture-proof container | Needles, lancets, blades, contaminated glass | Autoclave / dry heat / encapsulation |
| Glassware and metallic implants | Blue box + bag | Lab glassware, surgical implants | Disinfect → authorised recycler |
SELF-CHECK
A used syringe with its needle attached has just been withdrawn from a patient. Into which container should it be discarded?
A. Red bag (contaminated recyclable plastics)
B. Yellow bag (anatomical/chemical waste)
C. White/translucent puncture-proof container (sharps)
D. Blue cardboard box (glassware/metals)
Reveal Answer
Answer: C. White/translucent puncture-proof container (sharps)
An attached needle makes the entire syringe-needle unit a sharp. The BMW Rules 2016 assign all sharps — needles, lancets, scalpel blades, syringes WITH needles — to the white/translucent puncture-proof container. If the needle is first removed using a needle-cutter/destroyer, the hub and plastic barrel (now without a sharp point) can then be segregated into the red bag for autoclaving and recycling. Never recap a needle; never discard sharps into a bag that can be punctured.
Treatment Methods for Biomedical Waste
Treatment converts hazardous biomedical waste into a safer form before final disposal. The BMW Rules 2016 specify which methods are permissible for which waste categories. Understanding the scientific basis of each method helps you choose correctly and audit compliance in your future facility.
1. Incineration is high-temperature combustion (≥800°C in the primary chamber; ≥1,050°C in the secondary chamber). It is mandated for yellow-bag anatomical waste, cytotoxic/pharmaceutical waste, and soiled linen that cannot be autoclaved. Incineration reduces volume by 90–95% and renders infectious agents non-viable, but generates ash and flue gases (including dioxins/furans if temperature control fails). Incinerators must meet the pollution control standards set by the Central Pollution Control Board (CPCB).
2. Autoclaving (moist heat, steam sterilisation) subjects waste to pressurised steam — typically 121°C at 15 psi for 30–60 minutes. It is the method of choice for red-bag (recyclable plastics) and white-container (sharps) waste. Post-autoclaving, red-bag waste can be shredded and sent to recyclers; sharps can be encapsulated or shredded. Autoclaving cannot adequately treat anatomical waste, cytotoxic waste, or mercury-containing items.
3. Dry-heat sterilisation uses hot air at 160°C for 60 minutes (or 180°C for 30 minutes) and is an acceptable alternative to autoclaving for sharps treatment, particularly in facilities without access to pressurised steam.
4. Microwave treatment uses electromagnetic energy to heat water molecules in the waste, achieving disinfection. It is an accepted alternative to autoclaving for non-anatomical infectious waste (red-bag category). Microwave treatment is not suitable for anatomical waste, metallic items, or large volumes.
5. Deep burial is used in facilities too remote for incineration. Anatomical waste or placenta may be buried ≥2 metres deep in a site at least 50 metres from any water body, lined to prevent leaching, and covered with lime and soil. BMW Rules 2016 permit deep burial only for facilities in areas without access to common biomedical waste treatment facilities (CBWTFs).
6. Encapsulation involves filling a sharps container — when three-quarters full — with a solidifying agent (cement, lime, or molten plastic) and sealing it. Once hardened, it becomes a rigid monolith that cannot be reopened and is disposed of in a secured landfill. It is an alternative to autoclaving for sharps, particularly in resource-limited settings.
7. Plasma pyrolysis is an emerging technology used for cytotoxic drugs and some chemical waste streams, using a high-temperature plasma arc (>5,000°C) that breaks complex molecules into simpler, less toxic gases. It is energy-intensive but achieves near-complete destruction of organic chemicals.
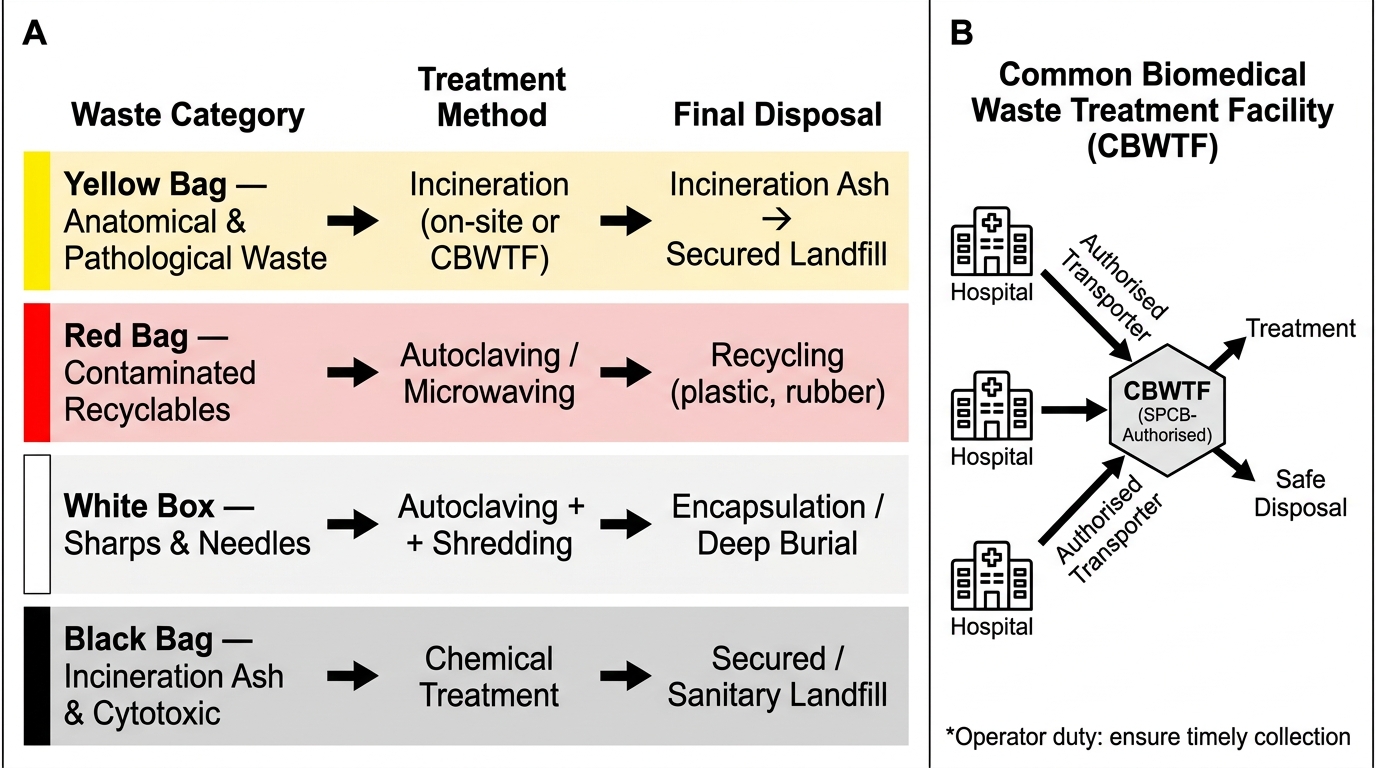
Biomedical Waste Treatment Pathways and CBWTF System
Most healthcare facilities (particularly in urban areas) do not have on-site incinerators. They use a Common Biomedical Waste Treatment Facility (CBWTF) — a centralised facility authorised by the State Pollution Control Board (SPCB) that collects biomedical waste from multiple healthcare facilities, treats it, and disposes of it. The healthcare facility operator's duty is to ensure timely collection by the authorised transporter.