Page 22 of 32
CM5.{12,16-17} | CM5.{12,16-17} | Breastfeeding Skills and Counselling — SDL Guide
Learning Objectives
- Demonstrate different types of breastfeeding holds, correct latching technique, and manual expression of breast milk using a baby model and breast model
- Describe the composition and benefits of breastfeeding and complementary feeding practices for infants
- Counsel mothers on breastfeeding with focus on attachment to breast and correct position of the newborn
- Identify and manage common breastfeeding problems using evidence-based counselling strategies
INSTRUCTIONS
Breastfeeding is the single most effective nutritional and immunological intervention for the newborn and infant. A doctor who cannot demonstrate correct latch and counsel a struggling mother cannot meet the OSCE competency requirement or the clinical need. This module combines the scientific evidence base with the practical skill of breastfeeding support.
References
- WHO/UNICEF — Infant and Young Child Feeding: Model Chapter for Textbooks, 2009 (guideline)
- WHO — Guideline: Protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services, 2017 (guideline)
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 11 — Nutrition and Health (IYCF section) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A first-time mother, 26 years old, is brought to the postnatal ward at 18 hours after an uncomplicated vaginal delivery. She is crying. 'The baby won't latch. She cried all night. I think I don't have enough milk.' The nurse has tried three times to help her feed but the infant is screaming. The baby's last weight is 3.2 kg (birth weight was 3.3 kg — a normal 3% physiological loss). The mother's breasts are engorged. On examination, the baby is being offered the nipple tip only — the areola is not in the baby's mouth, the lower lip is not flanged out, and the baby's chin is not touching the breast. The latch is incorrect — not the milk supply. This is one of the most common clinical encounters in postnatal care worldwide: a mother in distress because of a correctable technical problem that no one has taken 5 minutes to properly demonstrate and correct. This module gives you those 5 minutes.
WHY THIS MATTERS
Breastfeeding support is a clinical skill, not a midwifery nicety. CM5.12 is an OSCE skill competency — you will be asked to demonstrate breastfeeding holds and latching technique on a model. CM5.17 tests counselling competence specifically focused on attachment and position. CM5.16 tests the knowledge base. NFHS-5 (2019-21) reports India's exclusive breastfeeding rate at 63.7% — improved from 54.9% but still below the WHO global target of 70%. Early initiation of breastfeeding (within 1 hour) is at 41.8% nationally — meaning over half of Indian newborns do not receive early initiation. Every missed initiation opportunity represents lost colostrum (the newborn's 'first vaccine'), increased neonatal infection risk, and a higher likelihood of formula supplementation initiation that undermines the breastfeeding relationship.
RECALL
From cm-nutrition-requirements: recall that exclusive breastfeeding (EBF) provides all the nutrition a healthy infant needs for the first 6 months, including adequate iron (though breast milk iron is low in quantity, its bioavailability is ~50% — far higher than formula or food); Vitamin D is the only supplement recommended for exclusively breastfed infants in settings with limited sun exposure. From cm-nutrition-disorders: recall that Vitamin A in colostrum is a critical early source — colostrum is rich in Vitamin A, making early initiation and colostrum feeding a direct VAD prevention strategy. From your understanding of immunology: secretory IgA (sIgA) is the primary antibody in breast milk, providing mucosal immune protection against intestinal pathogens — the mechanism by which breastfeeding reduces diarrhoea and respiratory infection risk.
Burden of Suboptimal Breastfeeding and Its Public Health Impact
Suboptimal breastfeeding — defined as anything less than the WHO-recommended 6 months of exclusive breastfeeding followed by continued breastfeeding with complementary foods up to 2 years or beyond — is one of the leading causes of child mortality and morbidity globally. The Lancet Breastfeeding Series (2016) estimated that near-universal breastfeeding could prevent 823,000 deaths in children under 5 annually worldwide, including approximately 87,000 in South Asia, primarily through reduced diarrhoeal and respiratory mortality.
India's breastfeeding landscape (NFHS-5, 2019-21):
- Early initiation of breastfeeding (within 1 hour of birth): 41.8% — meaning 58% of Indian newborns miss the colostrum window; a WHO study (Edmond 2006) demonstrated that early initiation is associated with a 22% reduction in neonatal mortality.
- Exclusive breastfeeding (EBF) at 6 months: 63.7% — improved from 54.9% (NFHS-4), but below the WHO target of 70% and behind several smaller countries.
- Continued breastfeeding at 12 months: 85.9%; at 2 years: 60.5%.
- Prelacteal feeds (honey, water, formula given before breastfeeding is established): prevalent in many Indian communities — these displace colostrum and delay breastfeeding initiation.
Exclusive breastfeeding (EBF) means breast milk only for the first 6 months — no water, juice, solid foods, other milk, or drinks except vitamins and medications. This definition is often misunderstood: water is not safe in infancy below 6 months (breast milk is 87% water and fully meets hydration needs even in hot climates); giving water to an exclusively breastfed infant is a form of non-exclusive feeding that increases infection risk by introducing waterborne pathogens.
The reasons mothers stop breastfeeding before 6 months are predominantly addressable through skilled counselling: perceived insufficient milk supply (usually a latch problem, not a milk supply problem), nipple pain (a latch problem), engorgement (a drainage and positioning problem), and return to work (addressable through expressed breast milk and workplace lactation facilities). This is why physician-level counselling competence matters.
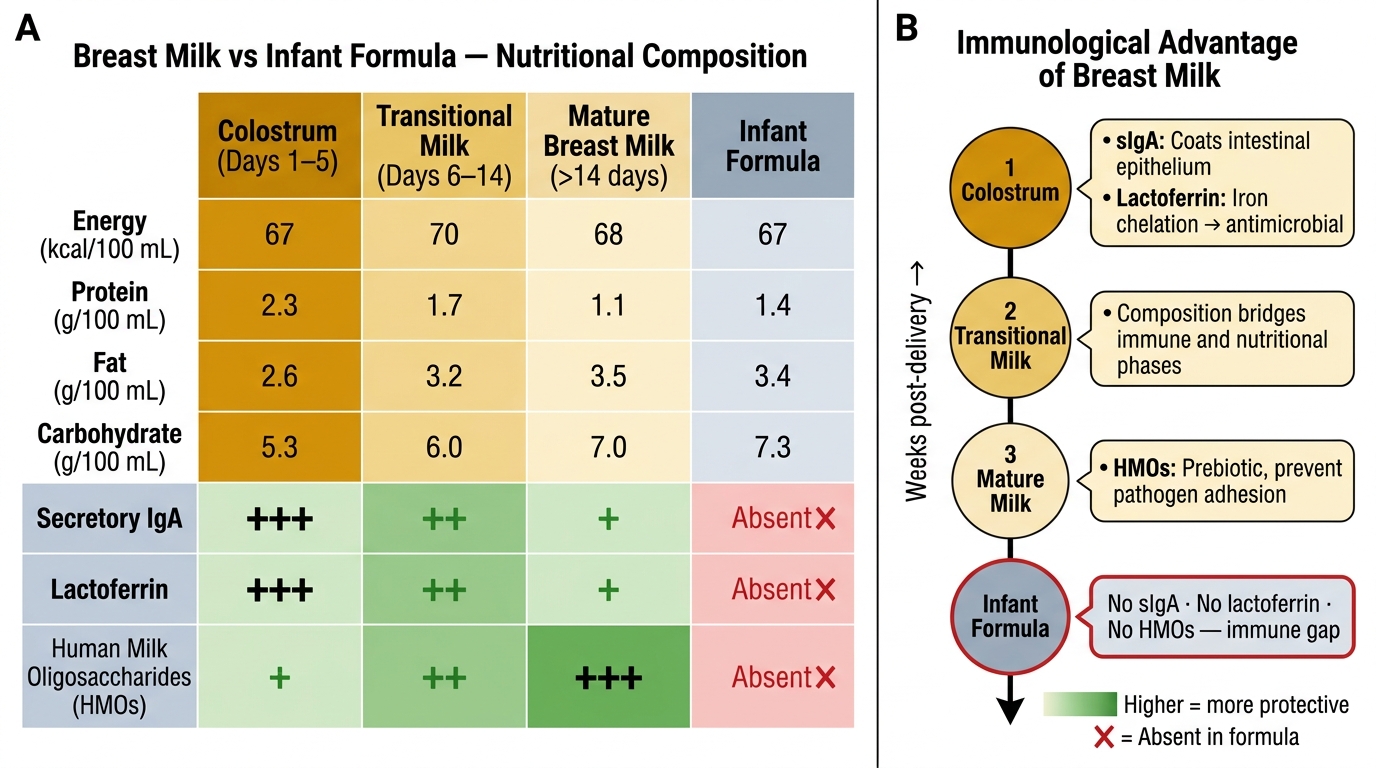
Breast Milk Composition Across Lactation Stages vs Infant Formula
Breast Milk Composition and the Science of Breastfeeding Benefits
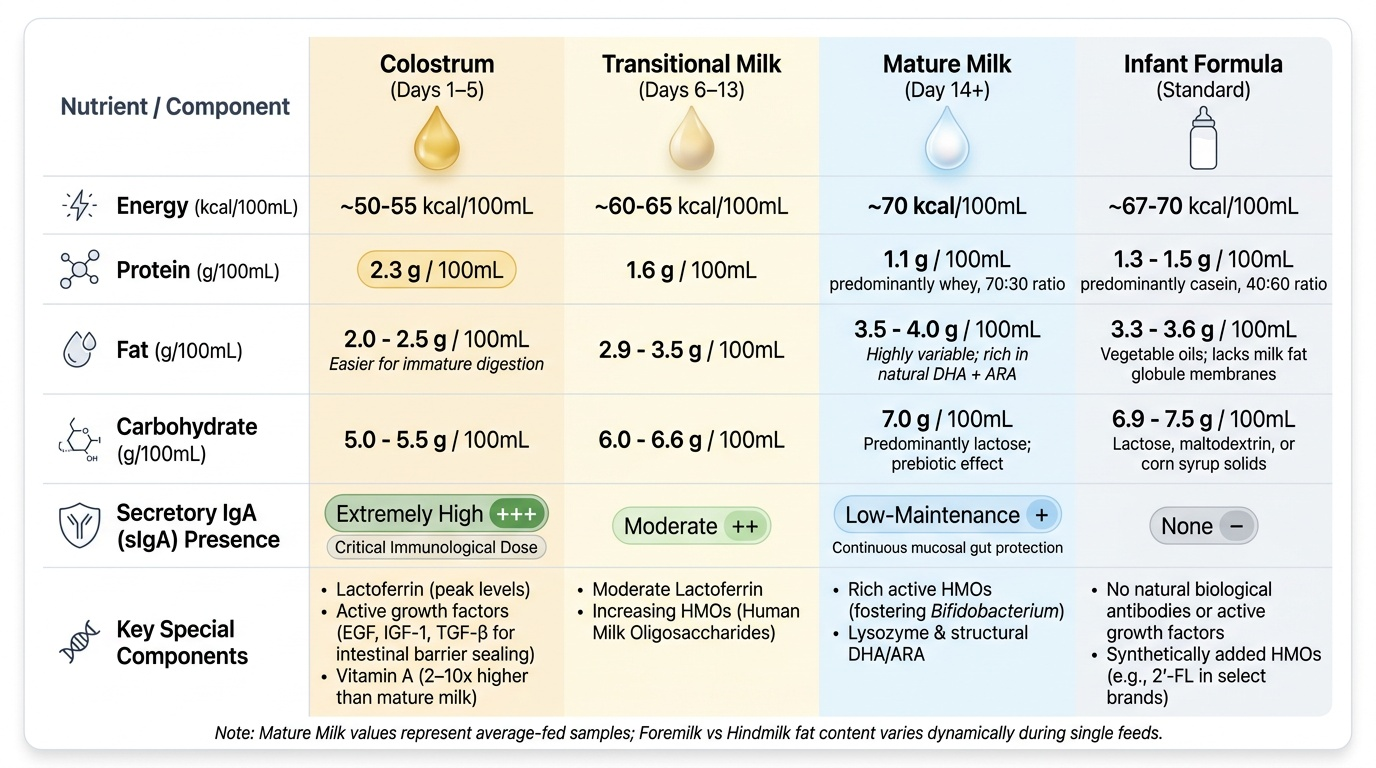
Provided image
Breast milk is not a uniform substance — it changes in composition across the feeding session (foremilk vs hindmilk), across the first weeks of lactation (colostrum → transitional → mature milk), and in response to the infant's gestational age and developmental needs. Understanding this composition is the scientific basis for counselling.
Colostrum (days 1-5 post-delivery): thick, yellow, and produced in small volumes (2-20 mL per feed in the first days). Despite its small volume, colostrum is precisely calibrated to the newborn's needs:
- High protein (~2.3 g/100 mL vs 1.1 g in mature milk) — primarily lactoferrin (iron-binding, antimicrobial) and secretory IgA (sIgA)
- Rich in secretory IgA — coating the newborn's gut mucosa, preventing pathogen adhesion; the newborn has not yet established its own intestinal immune barrier
- High Vitamin A — colostrum Vitamin A content is 2-10 times higher than mature milk; early initiation provides a critical dose of Vitamin A to the newborn
- Growth factors (EGF, IGF-1, TGF-β) — stimulate intestinal maturation, reducing intestinal permeability ('leaky gut')
- Lower fat than mature milk — easier for the newborn's immature pancreatic lipase system to digest
- Laxative effect — promotes passage of meconium, reducing neonatal jaundice (enterohepatic recirculation of bilirubin)
Mature breast milk (from ~day 14 onward): approximately 70 kcal/100 mL, containing protein ~1.1 g/100 mL (predominantly whey, with casein; whey:casein ratio in human milk 70:30 vs formula 40:60 or 60:40 depending on type), fat ~3.5-4 g/100 mL (variable — hindmilk is fat-rich; essential fatty acids DHA and ARA for brain and retinal development are present at higher levels than in most formula), lactose ~7 g/100 mL (primary carbohydrate; prebiotic effect via human milk oligosaccharides, HMOs, promoting growth of Lactobacillus and Bifidobacterium in infant gut microbiome).
Foremilk vs hindmilk: Foremilk (early in a feed) is watery, lower in fat — quenches thirst. Hindmilk (later in the same feed from the same breast) is higher in fat — provides energy satiety. This dynamic means: the infant should be allowed to drain one breast fully before offering the second — premature switching deprives the infant of hindmilk fat and causes watery green stools from lactose overload (often mistaken by mothers for diarrhoea).
Benefits for the infant:
- Diarrhoea: RR 0.36 compared to non-breastfed infants (Victora 2016)
- Acute respiratory infection: RR 0.57
- Necrotising enterocolitis in preterm infants: significantly reduced
- Childhood obesity: OR 0.78 (meta-analysis)
- IQ: ~3.4 IQ points higher in breastfed vs non-breastfed children after controlling for confounders (Victora 2015)
- Type 1 and Type 2 diabetes: risk reduction in multiple meta-analyses
Benefits for the mother:
- Breast cancer: RR 0.78 per 12 months of breastfeeding (IARC)
- Ovarian cancer: reduced risk
- Lactational amenorrhoea: 98% contraceptive efficacy if exclusively breastfeeding, baby <6 months, and no menstrual period resumed (Lactational Amenorrhoea Method, LAM)
- Faster postpartum uterine involution (oxytocin release during breastfeeding)
- Postpartum depression: some evidence of protective effect
SELF-CHECK
A mother of a 3-day-old newborn is concerned that her colostrum looks yellow and watery and that 'real milk has not come in yet.' She is considering supplementing with formula. What is the most accurate and reassuring response?
A. She is correct — colostrum is insufficient nutritionally and formula supplementation is appropriate from day 3
B. Colostrum is the ideal first food for the newborn: despite its small volume (2-20 mL per feed), it provides high IgA, Vitamin A, growth factors, and is precisely matched to the newborn's gastric capacity
C. Colostrum should be discarded as it contains impurities — real milk is what the baby needs
D. Formula has higher protein and caloric density than colostrum, so supplementation will accelerate the infant's weight recovery
Reveal Answer
Answer: B. Colostrum is the ideal first food for the newborn: despite its small volume (2-20 mL per feed), it provides high IgA, Vitamin A, growth factors, and is precisely matched to the newborn's gastric capacity
Colostrum is often described as the 'first vaccine' — it is nutritionally and immunologically perfect for the newborn. Its small volume (2-20 mL per feed) is appropriate for the newborn's stomach capacity (~5-7 mL on day 1, increasing to ~30-40 mL by day 3). It is rich in secretory IgA (coating gut mucosa to prevent infection), Vitamin A (2-10× higher than mature milk), and growth factors that stimulate intestinal maturation. Formula supplementation at this stage displaces colostrum, introduces foreign proteins, disrupts colonisation with beneficial bacteria, and undermines the breastfeeding relationship. The 3% physiological weight loss (up to 7-10% is normal) is expected and does not indicate nutritional failure if the latch is correct and feeding is frequent.
Breastfeeding Holds, Latch, and Manual Expression — The Clinical Skill
Breastfeeding position and attachment are the technical foundation of successful breastfeeding. Most problems with breastfeeding — nipple pain, perceived insufficient milk, engorgement, mastitis — have incorrect positioning or poor latch as their root cause. Correcting latch is therefore the single highest-yield intervention a physician or nurse can make in a breastfeeding support encounter.
The four classical breastfeeding holds:
1. Cradle hold: The most commonly used position. Infant lies horizontally on the mother's forearm, facing the breast; the infant's head rests in the bend of the mother's elbow on the same side as the breast being offered; the mother's hand supports the infant's bottom. Best for experienced mothers and older infants.
2. Cross-cradle hold (transitional hold): Infant's body lies across the mother's abdomen but the head is supported by the OPPOSITE hand (not the same-side hand). The mother holds the infant's head with thumb and fingers behind the ears, allowing more control of head positioning. Best for newborns and for teaching correct attachment — the most useful teaching hold.
3. Football hold (clutch hold): The infant is tucked under the mother's arm like a football, with the infant's legs pointing backward and the infant's head at the breast. The mother uses the hand on the same side to support the infant's head, freeing the opposite hand. Best for mothers after caesarean section (keeps infant weight off the abdominal incision), mothers with large breasts, premature infants, or twins.
4. Laid-back hold (biological nurturing): The mother reclines at a comfortable angle (approximately 45°); the infant is placed prone on the mother's chest and abdomen, with gravity assisting the infant to lie symmetrically on the mother. The infant's primitive rooting and feeding reflexes are activated by body contact and gravity. Evidence supports this as a particularly effective position for painful nipples and initial latching difficulties.
Signs of correct latch (OSCE checklist):
- Infant's mouth is wide open (>100-130° gape angle) before attaching — like a yawn, not a small circle
- Lower lip is turned outward (everted/flanged) — curled away from the breast, not tucked in
- More areola visible above the mouth than below (more areola is taken below the nipple)
- Chin touching the breast; nose clear of the breast (not blocked) or just touching
- Cheeks are full and rounded (not dimpled or sucked in)
- Mother hears audible swallowing — rhythmic suck-swallow-breathe pattern
- No nipple pain after the first few seconds of initial attachment (transient discomfort at attachment is normal; sustained pain = incorrect latch)
Signs of poor latch (correct the latch immediately):
- Clicking sound during feeding (infant losing vacuum, taking in air)
- Dimpled cheeks (infant is sucking cheek muscles, not breast)
- Nipple pain throughout the feed
- Visible nipple tip shape after feeding: nipple appears flattened, compressed, or creased (indicates the nipple was not deep enough in the mouth)
- Insufficient infant weight gain despite frequent feeding attempts
Manual expression of breast milk (Marmet technique):
Used when direct feeding is not possible (premature infant in NICU, maternal medication contraindication, infant separation). Steps:
1. Wash hands. Place thumb above the areola-nipple junction (not the nipple) and first two fingers below, forming a 'C' shape with the fingers about 2-3 cm from the nipple tip (at the edge of the areola).
2. Push back toward the chest wall (not squeezing the nipple).
3. Roll the thumb and fingers together toward the nipple — this mimics the infant's tongue peristaltic action compressing the milk sinuses.
4. Repeat rhythmically. Milk letdown usually occurs within 1-2 minutes. Rotate the finger position around the areola to drain all milk ducts.
5. Expression should be done at least 8-10 times per day to establish and maintain milk supply for an infant who cannot directly feed.
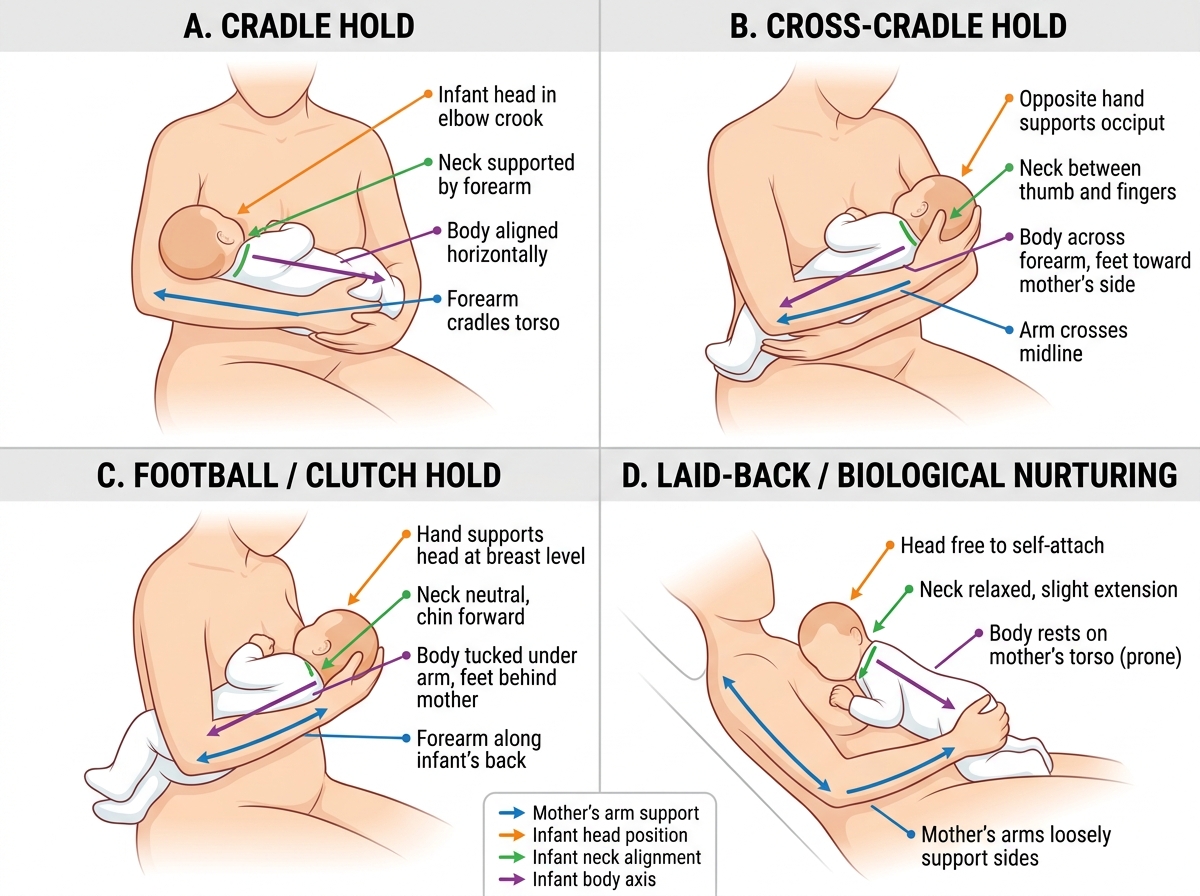
Four Breastfeeding Positions: Infant and Maternal Arm Positioning
SELF-CHECK
During an OSCE station, a mother (using a breast model and baby doll) is attempting to breastfeed. You observe: the baby doll's lower lip is tucked inward (not flanged out), the mother reports pain throughout feeding, and clicking sounds are audible. What is the correct assessment and intervention?
A. Normal breastfeeding; clicking sounds indicate efficient sucking
B. Poor latch — coach the mother to break the seal (little finger in corner of mouth), reposition with wider mouth gape, and ensure lower lip flange and chin-to-breast contact
C. Milk supply insufficiency — recommend formula supplementation
D. Engorgement — advise the mother to apply warm compresses before feeding
Reveal Answer
Answer: B. Poor latch — coach the mother to break the seal (little finger in corner of mouth), reposition with wider mouth gape, and ensure lower lip flange and chin-to-breast contact
The combination of tucked-in lower lip, sustained maternal pain, and clicking sounds = poor latch. The intervention is: (1) break the current seal by inserting a clean little finger gently into the corner of the baby's mouth to release the vacuum; (2) repositioning — ensure the infant's nose and chin are close to the breast, the head is tilted back slightly to open the mouth wide, and the lower lip is flanged outward before the nipple enters; (3) re-attach with the full areola — not just the nipple tip — deep in the infant's mouth. Clicking indicates air entering due to loss of vacuum (poor seal), not efficient sucking. Milk supply and engorgement are not the primary issues when latch is the problem.