Page 25 of 32
CM5.{13,18,21-22} | CM5.{13,18,21-22} | Complementary Feeding Counselling — SDL Guide
Learning Objectives
- Counsel a mother about complementary feeding for different age groups of the child, covering the 8 dietary diversity food groups, quantity, frequency, and consistency of food
- Counsel mothers on complementary feeding using National IYCF guidelines while being sensitive to cultural and socioeconomic influences
- Plan and conduct a health education session on nutrition in an NCD clinic or community setting
- Counsel mothers on both breastfeeding and complementary feeding in an integrated manner
INSTRUCTIONS
The 6-to-23-month period is the most nutritionally demanding and vulnerable window in a child's life outside of intrauterine life. Breastfeeding alone is no longer sufficient after 6 months, but introducing the wrong foods in the wrong way can be as harmful as introducing no foods. This module covers the science and the skill of complementary feeding counselling.
References
- WHO/UNICEF — Complementary Feeding: Family Foods for Breastfed Children, 2000 (guideline)
- National Institute of Nutrition (NIN/ICMR) — National Guidelines on Infant and Young Child Feeding, 2004 (guideline)
- WHO — Infant and Young Child Feeding: Model Chapter, 2009 (guideline)
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 11 — Nutrition and Health (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a well-child visit, an ASHA worker presents a 9-month-old girl who has been exclusively breastfed since birth and has never received any complementary food. Her weight-for-age Z-score is -2.3 (underweight), her haemoglobin is 8.9 g/dL, and she has pallor. The mother says: 'She is still small. I will start feeding her when she has teeth. Also, my mother-in-law says eggs and meat are 'hot' foods — the baby is too young.' The baby is missing 3 months of the complementary feeding window (6-9 months), has iron deficiency anaemia, and is stunting — all from a combination of delayed initiation, cultural food taboos, and inadequate dietary diversity. The physician's response requires simultaneously: correcting the timing (9 months is not 'too late' — but start immediately), addressing the cultural belief (reframe, not dismiss), and prescribing a practical, culturally acceptable, nutritionally adequate complementary feeding plan.
WHY THIS MATTERS
Complementary feeding is the nutritional bridge between exclusive breastfeeding and the family diet — and India is failing at this bridge. NFHS-5 (2019-21) shows that only 20.7% of Indian children aged 6-23 months receive a Minimum Acceptable Diet (MAD) — meaning 4 in 5 Indian children do not receive adequate complementary feeding. Minimum Dietary Diversity (MDD-C: ≥5 of 8 food groups) is met by only 44.6% of children. This translates directly into stunting (35.5%), anaemia (67.1% in under-5s), and impaired neurodevelopment. CM5.13 requires you to counsel a mother on the 8 dietary diversity food groups, quantity, frequency, and consistency — an OSCE-testable skill. CM5.18, CM5.21, and CM5.22 extend this to culturally sensitive counselling, group health education, and integrated breast + CF counselling — all clinical competencies you will exercise in community postings, antenatal/postnatal clinics, and ICDS/AWC visits.
RECALL
From the cm-nutrition-breastfeeding SDL: recall that exclusive breastfeeding (EBF) is breast milk ONLY for the first 6 months, and that continued breastfeeding alongside complementary foods up to 2 years is the WHO recommendation. Breastfeeding does NOT stop at 6 months — complementary foods are added to, not substituted for, breast milk. From cm-nutrition-disorders: recall that a term infant's iron stores from birth are sufficient for approximately 6 months — after this, complementary foods MUST include iron-rich foods to prevent IDA; breast milk alone (low iron, high bioavailability) is no longer sufficient to meet the growing infant's iron demands after 6 months. From cm-nutrition-requirements: the 8 dietary diversity food groups are the practical framework for ensuring micronutrient adequacy in complementary feeding.
Burden of Suboptimal Complementary Feeding in India
The 6-23 month period — from the start of complementary feeding to age 2 years — is the second most critical nutritional window in human development (after the intrauterine/early infancy period). Dietary deficiencies during this window produce stunting (irreversible height loss) and micronutrient deficiencies that impair brain development, immune function, and long-term productivity. NFHS-5 (2019-21) documents the scale of India's complementary feeding failure across four WHO IYCF indicators.
Only 20.7% of children aged 6-23 months receive a Minimum Acceptable Diet (MAD) — defined as meeting both minimum dietary diversity (≥5 of 8 food groups) AND minimum meal frequency. The other 79.3% — approximately 75 million Indian children — receive nutritionally inadequate complementary feeding at this critical developmental stage. Minimum Dietary Diversity (MDD-C) — ≥5 of 8 food groups in the previous 24 hours — is achieved by only 44.6% of children. Minimum Meal Frequency (MMF) — the age-appropriate number of complementary meals per day — is achieved by 71.4%, making dietary diversity the bigger gap (fewer children receive diverse foods than receive enough meals).
The nutritional consequences are documented in the same NFHS-5 survey: stunting 35.5%, wasting 19.3%, underweight 32.1%, and anaemia 67.1% in children 6-59 months — all significantly attributable to poor complementary feeding practices in this critical window. Stunting in this period is driven by inadequate protein, zinc, and caloric intake from complementary foods. Anaemia is driven by the transition from birth-store iron (adequate to ~6 months) to dietary iron dependence — at precisely the age when complementary feeding should be introducing iron-rich foods but often is not.
The determinants of poor CF in India are layered: poverty and food insecurity limit food diversity; cultural food taboos exclude nutritionally valuable foods (eggs, meat, fish) from infant diets in many communities; mothers receive insufficient CF counselling from healthcare workers; and the transition to complementary feeding at 6 months coincides with a drop in the frequency of healthcare contact (the antenatal-to-postnatal contact gap).
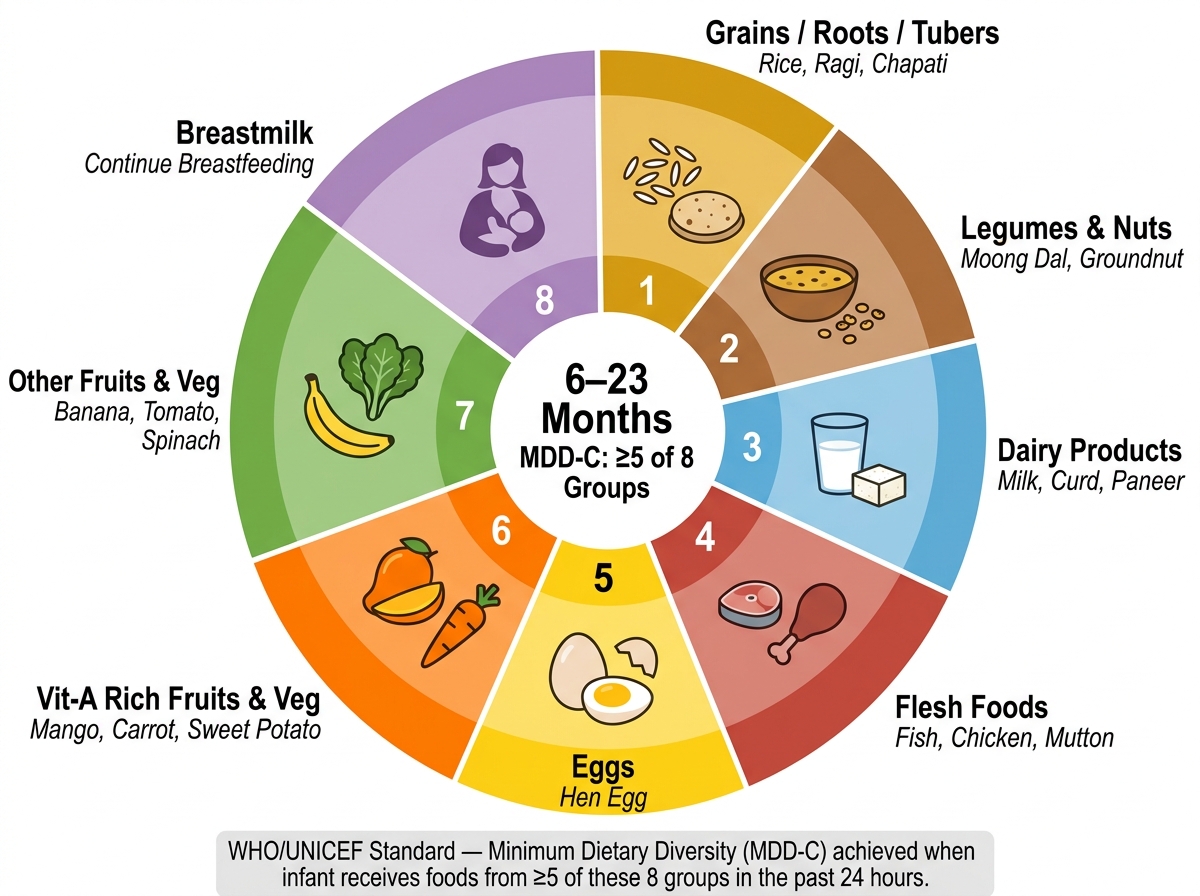
The 8 IYCF Dietary Diversity Food Groups for Infants 6–23 Months (WHO/UNICEF) with Indian Food Examples
The 8 Dietary Diversity Food Groups and WHO IYCF Guidelines
The WHO/UNICEF 8 dietary diversity food groups for children aged 6-23 months form the international standard framework for assessing and counselling on complementary feeding quality. A child who receives foods from ≥5 of these 8 groups in the previous 24 hours is classified as meeting Minimum Dietary Diversity (MDD-C) — a validated proxy indicator of micronutrient adequacy of the diet.
The 8 groups with Indian food examples:
1. Grains, white roots, tubers, and plantains: Rice, wheat/chapati, ragi, bajra, oats, potato, sweet potato, banana (green cooked). These provide energy and some B vitamins. This group is the most commonly consumed across India.
2. Legumes and nuts: Dal (moong, masoor, toor, chana, rajma), groundnut, cashew, almond. Provide protein, iron (non-haem), zinc, and healthy fats. Critical for vegetarian families as a protein and iron source.
3. Dairy products: Milk, curd, paneer, cheese. Provide calcium, protein, and Vitamin B12 (the only B12 source for vegetarians). IMPORTANT: cow's milk as a drink is NOT recommended before 12 months (displaces breast milk, high renal solute load, low iron, may cause occult GI bleeding); however, dairy as an ingredient (curd, paneer, milk in porridge) is appropriate from 6 months.
4. Flesh foods (meat, poultry, fish, seafood, organ meat/offal): Chicken, mutton, fish, liver (especially organ meat/liver). The most bioavailable source of iron, zinc, and Vitamin B12. Liver (~7 mg iron/100 g, haem iron at ~25% bioavailability) is the single most nutrient-dense complementary food available — one small serving of liver per week can significantly reduce IDA risk. Fish provides DHA for brain development.
5. Eggs: Provide complete protein (high biological value), iron, choline (brain development), Vitamin B12. One egg per day (from 6 months in non-allergic infants, can be introduced with the first complementary foods).
6. Vitamin A-rich fruits and vegetables: Orange/yellow/red fruits and vegetables and dark leafy greens — mango, papaya, carrot, pumpkin, tomato, sweet potato (orange-flesh), spinach, methi (fenugreek leaves), drumstick leaves. Provide β-carotene (pro-vitamin A), Vitamin C, folate. Drumstick leaves (Moringa oleifera): exceptional density — 6.8 mg iron, 440 mg calcium, 0.44 mg riboflavin per 100 g — an affordable, culturally familiar green in South India.
7. Other fruits and vegetables: Banana, apple, guava, cucumber, lauki (bottle gourd), cauliflower, okra. Provide various vitamins, minerals, and dietary fibre. Complete the dietary diversity requirement alongside Group 6.
8. Breastmilk: Counted as a food group for infants/children who are still breastfed; continues to provide significant nutrition (immunological, DHA, lactoferrin) even after 6 months.
Complementary feeding start timing: WHO recommendation is 'around 6 months' (minimum 180 days). NOT before 4 months (the infant's gut is not developmentally ready; risk of allergies, infections, and aspiration). Not delaying beyond 6-7 months (the iron-store cliff, developmental window for food acceptance, delayed oral-motor skill development).
Key IYCF indicators:
- MDD-C: ≥5 of 8 food groups in 24 hours (national rate 44.6%, NFHS-5)
- MMF: Minimum meal frequency by age (see next section)
- MAD: Meets both MDD-C AND MMF (national rate 20.7%, NFHS-5)
SELF-CHECK
An Anganwadi worker conducts a 24-hour dietary recall for an 8-month-old infant. The recall shows: rice porridge (Group 1), moong dal (Group 2), breast milk (Group 8), mashed banana (Group 7). The mother says she does not give eggs or meat 'for cultural reasons.' How many food groups has this infant received, does it meet MDD-C, and what is the single most nutritionally important food group missing?
A. 4 food groups; does NOT meet MDD-C (need ≥5); missing Group 4 (flesh foods) is most important
B. 4 food groups; does NOT meet MDD-C (need ≥5); missing Group 6 (Vitamin A-rich fruits/vegetables) is the most important single addition
C. 5 food groups; meets MDD-C; no critical food groups missing
D. 3 food groups; does NOT meet MDD-C; missing Groups 3, 4, and 5 equally
Reveal Answer
Answer: B. 4 food groups; does NOT meet MDD-C (need ≥5); missing Group 6 (Vitamin A-rich fruits/vegetables) is the most important single addition
The infant receives Groups 1 (rice), 2 (dal), 7 (banana), and 8 (breastmilk) = 4 food groups. MDD-C requires ≥5 groups — this infant does NOT meet MDD-C. While flesh foods (Group 4) and eggs (Group 5) are absent due to cultural reasons, the most nutritionally impactful single addition within the cultural constraint is a Vitamin A-rich orange/yellow vegetable or dark leafy green (Group 6) — such as mashed pumpkin, carrot, or drumstick leaves. This would bring the count to 5 (meeting MDD-C) and add pro-vitamin A, Vitamin C (which also enhances the non-haem iron bioavailability from the dal), and other micronutrients. If cultural constraints are addressed, organ meat/liver once a week would be the highest single nutritional impact food for iron — but Group 6 is the most achievable within stated constraints.
Quantity, Frequency, Consistency and Food Safety in Complementary Feeding
Complementary feeding must be age-appropriate in three dimensions simultaneously: the consistency must match the infant's oral-motor developmental stage; the quantity must meet the energy gap as breast milk's caloric contribution decreases; and the frequency must deliver enough meals to achieve the daily nutritional targets.
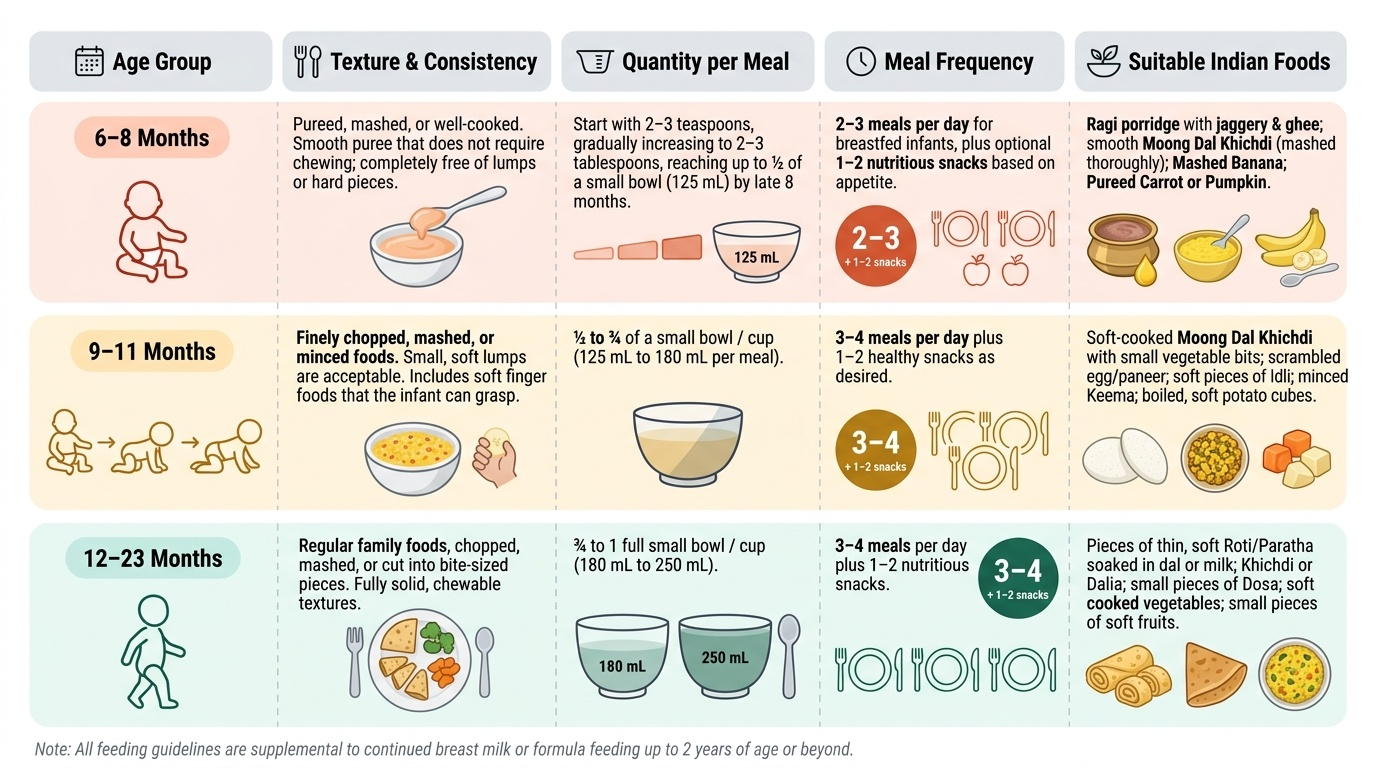
Age-wise complementary feeding guide (India/WHO guidelines):
6-8 months:
- Consistency: Pureed, mashed, or well-cooked — smooth puree that does not require chewing; no lumps or hard pieces. Start with thick pureed single-ingredient foods (rice porridge, mashed ragi, dal purée, mashed banana) before moving to mixed purees.
- Quantity: Start with 2-3 teaspoons per meal, increasing gradually to 2-3 tablespoons per meal by 8 months, then to half a small bowl (125 mL) by late 8 months.
- Frequency: 2-3 meals per day for breastfed infants + 1-2 nutritious snacks as desired.
- Examples: Ragi porridge with jaggery + ghee; moong dal khichdi (rice + dal, mashed); mashed banana; pureed carrot or pumpkin.
9-11 months:
- Consistency: Finely chopped, mashed, or minced foods — small soft lumps are acceptable; soft finger foods that the infant can pick up and self-feed (important for oral-motor development and responsive feeding).
- Quantity: Half a bowl to one full small bowl (125-175 mL) per meal.
- Frequency: 3-4 meals per day for breastfed infants + 1-2 nutritious snacks.
- Examples: Soft khichdi with vegetables; mashed roti soaked in dal; small pieces of soft ripe fruit; egg scrambled with vegetables; minced chicken/fish if family accepts.
12-23 months:
- Consistency: Family foods, finely chopped or soft — the toddler joins the family meal with minor modification (low salt, low spice). Whole family diet should be nutritious; if the family eats high-salt, high-spice foods, prepare a milder portion before adding seasoning.
- Quantity: 3/4 to one full bowl (175-250 mL) per meal.
- Frequency: 3-4 meals per day + 1-2 healthy snacks for breastfed; 4-5 meals + snacks for non-breastfed toddlers.
- Examples: Full family meal (dal-rice-sabzi + small piece of roti); banana and curd as snack; small pieces of chicken or fish.
Responsive feeding: Caregivers should feed infants actively but responsively — responding to hunger and satiety cues, making eye contact, talking, and making feeding a positive experience. Avoid force-feeding (increases food refusal, undermines self-regulation of appetite), distractions (screen time during meals → reduced attention to hunger cues), and using food as reward/punishment. During illness: continue breastfeeding; offer foods even if appetite is reduced; increase meal frequency during recovery to restore nutritional losses.
Food safety in CF preparation: Prepare complementary foods fresh or immediately before feeding (bacteria multiply rapidly at room temperature). Wash hands before food preparation. Store complementary foods in clean, covered containers; do not store for more than 2 hours at room temperature. Boil or purify water used in food preparation. Clean all utensils and feeding cups with soap and water.
Provided image
SELF-CHECK
A mother asks how often she should feed her 10-month-old breastfed baby complementary foods per day, and what texture is appropriate. According to WHO/IYCF and India's National Guidelines, which answer is correct?
A. 1 meal per day of pureed food — the infant is too young for more
B. 3-4 meals per day of finely chopped or mashed foods plus 1-2 nutritious snacks
C. 5 meals per day of fully mashed and sieved food without lumps
D. 2 meals per day of pureed food, increasing to 3 at 12 months
Reveal Answer
Answer: B. 3-4 meals per day of finely chopped or mashed foods plus 1-2 nutritious snacks
A 10-month-old falls in the 9-11-month age group. WHO/IYCF guidelines recommend: 3-4 complementary meals per day for a breastfed infant (plus 1-2 nutritious snacks). Texture at 9-11 months = finely chopped, mashed, or minced foods with small soft lumps; finger foods are appropriate and support oral-motor development and self-feeding skills. Sieved/smooth purée is appropriate only at 6-8 months (earlier developmental stage). A 10-month-old fed only 1-2 meals of pureed food is receiving inadequate complementary feeding — insufficient frequency AND inappropriate texture for developmental stage.