Page 10 of 32
CM5.3 | CM5.3 | Nutrition Related Disorders — SDL Guide (Part 2)
Control and Management of Nutrition-Related Disorders
Control of nutrition-related disorders operates on three levels: (1) Supplementation — providing the deficient nutrient directly to at-risk populations; (2) Fortification — adding nutrients to commonly consumed foods at the production stage; (3) Dietary diversification — improving diet quality through promotion and education. For severe cases, therapeutic management precedes long-term prevention strategies.
Management of Severe Acute Malnutrition (SAM) / Kwashiorkor/Marasmus: Follows the WHO 10-step protocol at Nutrition Rehabilitation Centres (NRCs):
1. Treat hypoglycaemia (50% glucose or sugar water if unconscious)
2. Treat hypothermia (warming)
3. Treat dehydration (ORS — special low-osmolarity SAM-ORS, NOT standard ORS which has excess sodium)
4. Correct electrolytes — potassium and magnesium supplementation (NOT sodium)
5. Treat infection (broad-spectrum antibiotics: amoxicillin for 7 days; gentamicin if severe)
6. Correct micronutrient deficiencies (multi-micronutrient supplement WITHOUT iron initially)
7. Initiate cautious feeding (F-75: 75 kcal/100 mL, low-protein starter formula) — 2-hourly small feeds
8. Achieve catch-up growth (F-100: 100 kcal/100 mL, higher protein, or RUTF — Ready-to-Use Therapeutic Food: Plumpy'Nut, 500 kcal/100 g peanut-based)
9. Provide sensory stimulation and emotional support
10. Prepare for follow-up after recovery
Control of Iron Deficiency Anaemia: Supplementation: IFA (Iron-Folic Acid) tablets to pregnant women (1 IFA = 60 mg elemental iron + 500 µg folic acid, daily for at least 180 days); WIFS (Weekly IFA Supplementation) for adolescent girls (India's NIPI programme: 1 IFA/week under supervision at schools and AWCs); iron supplementation with Vitamin C for children with diagnosed IDA. Fortification: rice fortification (Government of India from 2024 — fortified rice distributed through PDS and MDM with iron, folic acid, Vitamin B12). Dietary diversification: counsel on haem and non-haem iron sources; Vitamin C co-ingestion; avoid tea/coffee at meals.
Control of Iodine Deficiency Disorders: Universal Salt Iodisation (USI) is the cornerstone — mandatory iodisation of all edible salt to 15 ppm at consumer level under NIDDCP. Quality assurance through iodine spot testing kits distributed to community health workers. Monitoring via goitre prevalence surveys and urinary iodine concentration (UIC) surveys — target median UIC >100 µg/L in school-age children.
Control of Vitamin A Deficiency: National Vitamin A Supplementation Programme under VHSND — biannual oral vitamin A doses: 100,000 IU (children 6-11 months), 200,000 IU (12-59 months). For established corneal involvement (X2-X3): emergency Vitamin A treatment — 200,000 IU orally on Day 1, Day 2, and Day 8. Dietary promotion of orange/yellow fruits, vegetables, and dark-green leafy vegetables (provitamin A). Fortification of Vanaspati (vegetable ghee) with Vitamin A (mandatory in India).
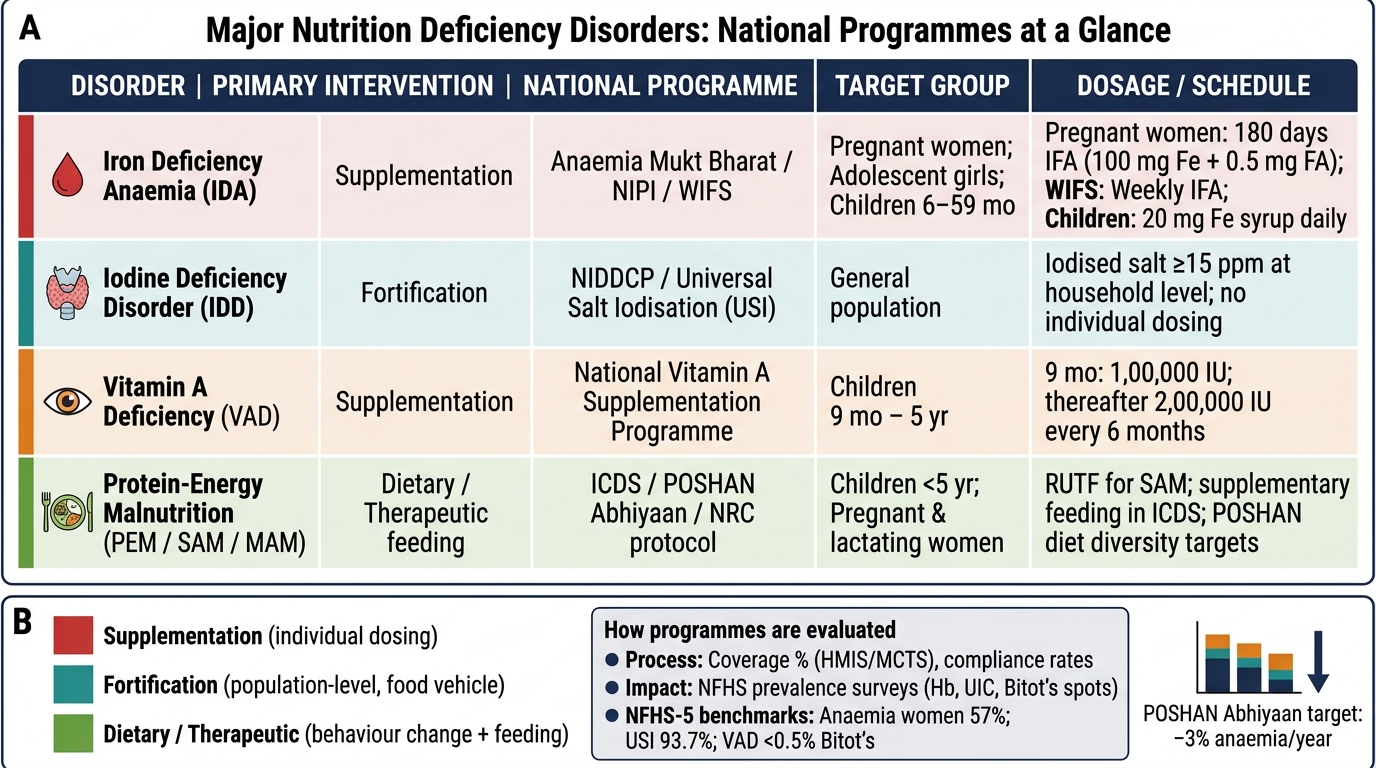
National Nutrition Deficiency Programmes: Summary Reference Table
Evaluation of Nutrition Programme Effectiveness
National nutrition programmes are evaluated using a combination of process indicators (coverage, compliance) and impact indicators (change in nutritional status at the population level). Effective evaluation allows programmes to be scaled, modified, or redirected based on evidence.
For IDA control, key evaluation indicators are: prevalence of anaemia by haemoglobin estimation in NFHS surveys (target: reduce anaemia in children, women, and pregnant women by 3% per year under POSHAN Abhiyaan); IFA supplementation coverage in pregnant women (HMIS/MCTS data); WIFS coverage in adolescent girls (school health reporting). NFHS-5 shows anaemia in women aged 15-49 increased from 53% (NFHS-4) to 57% (NFHS-5) — a setback attributed partly to COVID-19 disruptions and partly to improved haemoglobin measurement methodology.
For IDD control: goitre prevalence surveys (district-level); urinary iodine concentration (UIC) surveys in school-age children — WHO target is median UIC 100-299 µg/L (optimal range); iodised salt coverage (NFHS indicator: 'household uses iodised salt'). NFHS-5 shows 93.7% of households using iodised salt — a major success of USI.
For VAD control: Bitot's spots prevalence in children 1-5 years <0.5% = no longer a public health problem (WHO criterion); night blindness prevalence <1% in children; NFHS surveys on child dietary diversity (minimum dietary diversity score ≥4 food groups in children 6-23 months). The national biannual Vitamin A distribution coverage at VHSND sessions is tracked via HMIS.
For PEM control: stunting (HAZ <-2), wasting (WHZ <-2), and underweight (WAZ <-2) prevalence from NFHS and NNMB (National Nutrition Monitoring Bureau) surveys; NRC admission, discharge, and default rates; programme coverage for SAM children (India's CMAM — Community-based Management of Acute Malnutrition programme). POSHAN Abhiyaan's POSHAN Tracker app provides near-real-time data from AWCs, enabling district-level monitoring of weight-gain trajectories in children under 5.
Clinical Application — Recognising and Managing Deficiency in Practice
Translating knowledge of nutrition-related disorders into clinical practice requires the ability to: (1) recognise deficiency syndromes from clinical or community presentations; (2) confirm with targeted investigation; (3) initiate appropriate management; and (4) counsel on prevention and follow-up. The following case-structured approach organises this skill.
Recognising PEM in a community setting: Apply the WHO SAM criteria — MUAC <11.5 cm OR WHZ <-3 OR bilateral pitting oedema in a child 6-59 months. If any criterion is met → SAM → refer to NRC or initiate outpatient therapeutic care (RUTF if no medical complication). Kwashiorkor (oedema + hair/skin changes) vs marasmus (severe wasting, no oedema) changes the urgency of oedema management and the feeding protocol (F-75 vs immediate F-100/RUTF).
Recognising IDA clinically: Pallor of conjunctiva, palmar creases, nail beds; confirm with haemoglobin (finger-prick or venous). If Hb <12 g/dL (non-pregnant woman): prescribe IFA (60 mg elemental iron + 500 µg folic acid) once daily on empty stomach (or with Vitamin C) for 3-6 months; repeat Hb at 4 weeks (expect rise of ≥1 g/dL if iron-responsive). Simultaneously: counsel on iron-rich foods (liver, meat, green leafy vegetables, horse gram, bajra) and co-ingestion with Vitamin C; exclude hookworm (stool examination); ensure menstrual hygiene and inter-pregnancy spacing.
Recognising VAD in a community setting: Night blindness (ask specifically: 'Does the child bump into things or fall at dusk?'), Bitot's spots (look at temporal bulbar conjunctiva in daylight), or conjunctival/corneal xerosis. Corneal involvement (stage X2 and above) → emergency megadose Vitamin A (200,000 IU orally, repeat on Day 2 and Day 8). Bitot's spots (X1B) → megadose Vitamin A (200,000 IU) + dietary counselling (orange/yellow foods, dark greens).
Recognising IDD in a community setting: Goitre (visible neck swelling, larger in females, adolescents, pregnant women) → confirm by palpation (WHO grading) → enquire about iodised salt use → assess UIC if survey context → counsel on universal use of iodised salt. Cretinism in a newborn or infant — hypothyroid features (constipation, delayed milestones, coarse features, macroglossia, umbilical hernia) — → refer for thyroid function testing and early thyroid hormone replacement (critical: the earlier the treatment, the better the neurodevelopmental outcome).
SELF-CHECK
An NRC nurse identifies a 3-year-old child with SAM (MUAC 10.8 cm) who is alert but has diarrhoea. She gives oral rehydration. Which ORS formulation is specifically recommended for SAM children, and why?
A. Standard WHO-ORS (311 mOsmol/L), as it is the only validated formulation
B. ReSoMal (Rehydration Solution for Malnutrition), which has lower sodium and added potassium and magnesium
C. Plain water and sugar only, to avoid electrolyte overload
D. IV normal saline, since oral rehydration is contraindicated in SAM with diarrhoea
Reveal Answer
Answer: B. ReSoMal (Rehydration Solution for Malnutrition), which has lower sodium and added potassium and magnesium
SAM children have abnormal cellular electrolyte balance — intracellular potassium and magnesium deficiency, and reduced capacity to handle excess sodium due to impaired Na/K-ATPase activity. Standard ORS (311 mOsmol/L, 90 mmol/L sodium) can cause hypernatraemia in SAM. ReSoMal is specifically formulated for SAM rehydration: lower sodium (~45 mmol/L), higher potassium (~40 mmol/L), added magnesium, and glucose at 125 mmol/L. It is the WHO-recommended rehydration solution for SAM children. IV fluid in SAM carries a high risk of fluid overload and cardiac failure — restrict to truly unresponsive cases under close monitoring.
CLINICAL PEARL
The nutrition-infection vicious cycle is the mechanistic basis of why malnourished children die from measles, diarrhoea, and respiratory infections — not just starvation. Protein-energy malnutrition impairs every arm of the immune system: thymic atrophy reduces T-cell production, secretory IgA declines (opening mucosal barriers), complement activity falls, phagocyte function is impaired. A child with moderate PEM who contracts measles has a 400-fold higher case fatality rate than a well-nourished child with the same measles virus exposure. Similarly, Vitamin A deficiency reduces epithelial integrity in the respiratory and GI tracts, increasing severity of respiratory infections and diarrhoea. This is why the WHO '10-step protocol' for SAM management treats infection empirically with antibiotics even in the absence of clinical signs — subclinical infections are universal in SAM and are rapidly fatal if not treated simultaneously with nutritional rehabilitation. The practical clinical implication: always assess nutritional status when managing childhood infections, and always assess infection status when managing childhood malnutrition.