Page 12 of 32
CM5.5-6 | CM5.5-6 | Nutrition Surveillance and National Programmes — SDL Guide
Learning Objectives
- Describe the methods of nutritional surveillance and their objectives in the context of socio-cultural factors
- Enumerate and discuss the National Nutrition Policy and important national nutritional programmes including ICDS, PM POSHAN, POSHAN Abhiyaan, NIDDCP, and WIFS
- Explain the principles of nutritional education and rehabilitation
- Describe the medical officer's role in implementing and monitoring national nutrition programmes at the community level
INSTRUCTIONS
Knowledge of national nutrition programmes is not optional for a community medicine physician — it is the operational toolkit for translating nutrition science into population-level action. This module covers the surveillance systems that detect nutritional problems and the programmes designed to solve them.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 11 — Nutrition and Health; Ch. 24 — National Programmes (textbook)
- National Nutrition Policy, Government of India, 1993 (revised framework under POSHAN Abhiyaan 2018) (policy)
- NFHS-5 2019-21 National Report, Ministry of Health and Family Welfare, Government of India (report)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a district-level health planning meeting in Rajasthan, the Chief Medical Officer presents the district's latest NFHS-5 data: stunting 42%, wasting 22%, anaemia in women 63% — all above the national average. An Anganwadi worker raises her hand: 'We give supplementary nutrition every day, but children are still wasting. Why?' The answer is multi-layered. Supplementary nutrition through ICDS is designed to provide 500 kcal and 12-15 g protein to at-risk children daily — but this alone cannot overcome poverty-driven food insecurity at home, poor water and sanitation driving diarrhoeal disease, or cultural practices that restrict which foods mothers introduce during complementary feeding. Nutrition programmes work not as single interventions but as coordinated systems — surveillance identifies who is malnourished, programmes deliver the response, education shifts behaviour, and socio-cultural engagement makes change sustainable. Understanding this system is essential to your role as a community medicine physician.
WHY THIS MATTERS
Every primary care physician in India works within the infrastructure of national nutrition programmes — whether they recognise it or not. The Anganwadi worker who brings a child to your PHC for referral is part of ICDS. The iron-folic acid tablets a pregnant woman brings to antenatal clinic came from the WIFS/ANC supply chain. The iodised salt in the district PDS distribution is mandated by NIDDCP. As a medical officer at a PHC, you will supervise NRC referrals, conduct VHSND sessions, monitor Anganwadi registers for growth-faltering children, and counsel families — all within the architecture of these programmes. CM5.5 and CM5.6 test whether you can describe and discuss these programmes in clinical and community examination settings.
RECALL
From the previous SDL (cm-nutrition-disorders): recall the major nutrition-related disorders that India's programmes address — PEM (stunting, wasting, SAM), Iron Deficiency Anaemia (IDA), Iodine Deficiency Disorders (IDD), and Vitamin A Deficiency (VAD). Recall the NFHS-5 burden statistics: stunting 35.5%, wasting 19.3% in under-5s; anaemia 57% in women 15-49. From cm-nutrition-requirements: recall that the 'first 1000 days' (conception to 24 months) is the critical window for irreversible nutritional programming — this period is the primary target of ICDS and other maternal-child nutrition programmes. Nutritional surveillance provides the epidemiological evidence base that drives programme design, targeting, and evaluation.
The Burden of Malnutrition that Programmes Address
India's national nutrition programmes were not designed in a vacuum — each addresses a specific, epidemiologically documented nutritional problem. Understanding which burden each programme targets is the first step to understanding why the programme is structured as it is, what it delivers, and how to evaluate it.
The first 1000 days — the period from conception to the child's second birthday — is the most critical nutritional window in human development. Nutritional deficits during this period produce irreversible consequences: stunted growth, reduced cognitive capacity, impaired immune function, and increased risk of chronic disease in adulthood. NFHS-5 (2019-21) shows that India's under-5 stunting prevalence (35.5%) and wasting prevalence (19.3%) remain among the highest in the world, despite significant reductions since 2005-06. The urgency of this burden is the rationale for the comprehensive investment in ICDS (targeting the 0-6 year age group) and the maternal nutrition components of PM POSHAN and POSHAN Abhiyaan.
Among school-age children and adolescents, the burden shifts to micronutrient deficiency — particularly iron (anaemia) and iodine. Adolescent girls who are anaemic enter pregnancy with already-depleted iron stores, perpetuating the intergenerational cycle of maternal anaemia and low birth weight. This is the burden that WIFS (Weekly Iron and Folic Acid Supplementation) and school health programmes address.
The National Nutrition Policy (1993) — India's first overarching nutrition policy — identified these problems and articulated a multi-sectoral framework for addressing them through agriculture, food distribution, education, public health, and social welfare. POSHAN Abhiyaan (2018) operationalises this framework with time-bound targets, real-time monitoring, and district-level accountability. The policy goal is not just to reduce malnutrition prevalence but to eliminate stunting as a public health problem — defined as reducing stunting to <25% by 2022 (a target that was not fully met but drove significant momentum).
India's National Nutrition Programmes: Comparative Overview
Nutritional Surveillance — Methods and Objectives
Nutritional surveillance is defined as 'the continuous monitoring of the nutritional status of the population in order to provide information for making decisions that lead to improvement in nutritional status' (FAO/WHO). The key word is continuous — surveillance is not a one-time survey but an ongoing system that generates actionable data.
Objectives of nutritional surveillance:
1. Early warning — detect early deterioration in nutritional status before it reaches crisis proportions (e.g. seasonal famine early warning, growth faltering detection before SAM)
2. Programme monitoring — track whether nutrition programmes are reaching their targets and beneficiaries
3. Programme evaluation — measure impact of programmes on nutritional outcomes over time
4. Policy planning — provide evidence for designing new programmes, allocating resources, and targeting vulnerable populations
Methods of nutritional surveillance:
Nutritional surveys: Cross-sectional measurement of nutritional status indicators in a representative sample. India's key surveys: NFHS (National Family Health Survey, conducted every 5 years; NFHS-5 = 2019-21); NNMB (National Nutrition Monitoring Bureau under NIN — conducts dietary intake and clinical surveys in rural India, 10 states); CNNS (Comprehensive National Nutrition Survey 2016-18, for children 0-19 years). These surveys provide population-level denominators for programme planning.
Routine health information systems: HMIS (Health Management Information System) captures IFA supplementation coverage, Vitamin A dose coverage, institutional delivery rates, and child growth monitoring data from AWCs via the POSHAN Tracker app. This is continuous, real-time surveillance but depends on quality of data entry by frontline health workers.
Food balance sheets: National-level data on food production, imports, exports, and consumption, maintained by MoAFW; used to estimate per capita energy availability and identify gaps between food production and nutritional requirements.
Vital statistics: Infant mortality rate (IMR), under-5 mortality rate (U5MR), low birth weight (LBW) rate, and maternal mortality ratio (MMR) are indirect indicators of nutritional status. A community with IMR >50 or LBW >15% is signalling likely undernutrition. These indicators are routinely collected through civil registration and SRS (Sample Registration System).
Sentinel surveillance sites: Fixed sites (typically AWCs, PHCs, schools) where periodic, standardised nutritional assessments are conducted to track trends over time. ICDS growth monitoring at AWCs functions as sentinel surveillance for under-5 nutritional status.
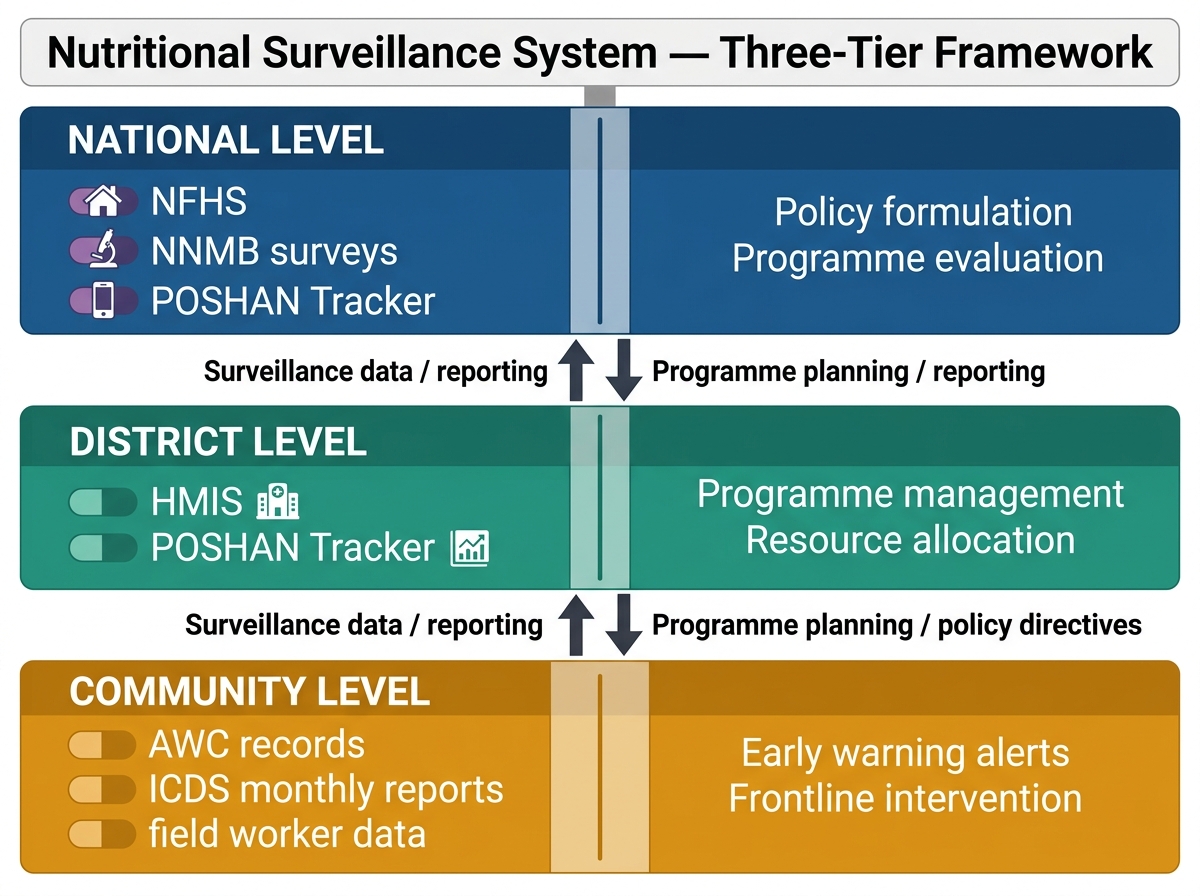
India's Three-Tier Nutritional Surveillance System: Data Sources and Information Flow
SELF-CHECK
A district nutrition officer wants to assess whether the ICDS programme in her district is achieving its nutritional targets. She collects monthly weight-for-age Z-scores from all Anganwadi Centres. Which level and method of nutritional surveillance does this represent?
A. National-level periodic survey (NFHS method)
B. Community-level sentinel surveillance using routine programme data
C. Food balance sheet analysis
D. Ecological/indirect indicator surveillance
Reveal Answer
Answer: B. Community-level sentinel surveillance using routine programme data
Monthly weight-for-age measurement at Anganwadi Centres using programme data represents community/district-level sentinel surveillance — fixed sites (AWCs) with periodic, standardised data collection. This is distinct from national cross-sectional surveys (NFHS, NNMB), which are population-representative but less frequent. Food balance sheets estimate per capita food availability from production data, not individual nutritional status. Ecological indicators (IMR, LBW) are indirect proxies for nutritional status, not direct measurements.
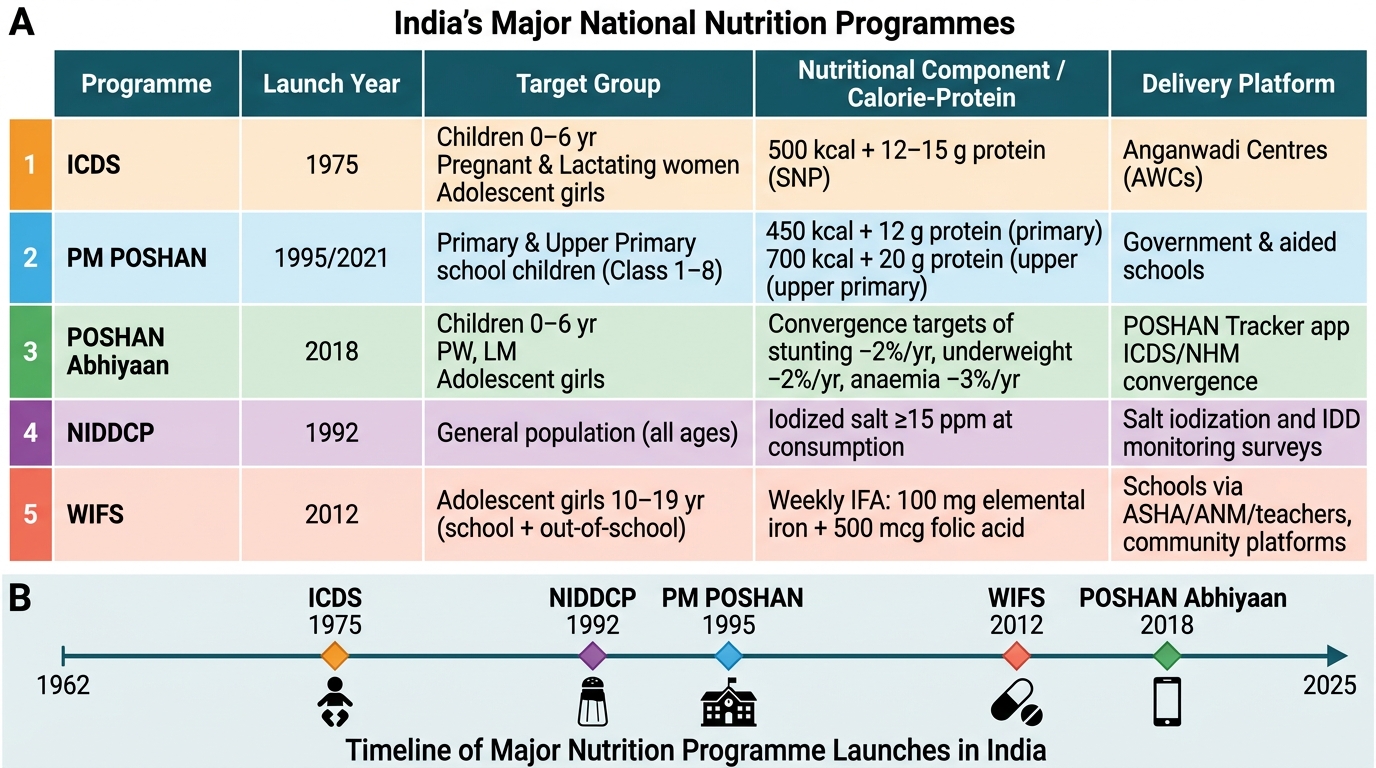
India's Major National Nutrition Programmes
India's national nutrition programmes form a comprehensive but complex system, each targeting specific populations and addressing specific nutritional deficiencies. Understanding each programme's target group, nutritional content, delivery mechanism, and evaluation indicator is essential for both examination and clinical practice.
1. Integrated Child Development Services (ICDS) — launched 1975:
Target: children 0-6 years, pregnant and lactating women, and adolescent girls (in some states). Delivery platform: Anganwadi Centres (AWCs) — approximately 14 lakh (1.4 million) centres across India, making it the world's largest integrated nutrition programme. Services: (a) Supplementary nutrition — children 6 months-6 years receive 500 kcal + 12-15 g protein/day; pregnant/lactating women receive 600 kcal + 18-20 g protein/day; (b) Immunisation; (c) Health check-up; (d) Referral services; (e) Pre-school education (3-6 years); (f) Nutrition and health education for mothers. The AWC is the 'first mile' of the MCH system — where growth monitoring, supplementary nutrition, and referral for SAM happen at the community level.
2. PM POSHAN (National Mid-Day Meal Scheme) — launched 1995, renamed PM POSHAN 2021:
Target: children in Classes 1-8 in government and government-aided schools. Nutritional content: primary classes (1-5): 450 kcal + 12 g protein/meal; upper primary classes (6-8): 700 kcal + 20 g protein/meal. Covers >11.8 crore (118 million) children daily. Dual objective: nutritional and educational (improves enrolment, attendance, and retention, especially for girls).
3. POSHAN Abhiyaan (National Nutrition Mission) — launched 2018:
Time-bound targets: reduce stunting by 2% per year, wasting by 2% per year, anaemia by 3% per year (children <6 years, adolescent girls, pregnant/lactating women), LBW by 2% per year. Approach: convergence across ICDS, health (RMNCH+A), WASH, agriculture, and social protection. Key innovation: POSHAN Tracker app — real-time monitoring of ICDS data from AWCs using smartphones, enabling district-level accountability and programme management. 'Jan Andolan' (people's movement) component promotes community-level behaviour change.
4. National Iodine Deficiency Disorders Control Programme (NIDDCP):
Strategy: Universal Salt Iodisation (USI) — mandatory iodisation of all edible salt to 30 ppm at production, 15 ppm at consumer level. Key achievement: household iodised salt coverage rose from ~51% (NFHS-3, 2005-06) to 93.7% (NFHS-5, 2019-21). Monitoring: urinary iodine concentration surveys, goitre prevalence surveys, spot testing kits distributed to community health workers. India's legislation: Prevention of Food Adulteration Act covers salt iodisation standards.
5. Weekly Iron and Folic Acid Supplementation (WIFS):
Target: adolescent girls (10-19 years) in school and out-of-school settings, and adolescent boys (in some states). Dose: one IFA tablet per week (100 mg elemental iron + 500 µg folic acid), supervised at schools and AWCs. Also includes biannual deworming. Implemented under RBSK (Rashtriya Bal Swasthya Karyakram) and POSHAN Abhiyaan. Rationale: adolescent girls who enter pregnancy with depleted iron stores have higher rates of maternal anaemia and low birth weight infants.
6. National Food Security Act (NFSA) 2013:
Legal entitlement to subsidised food for 67% of India's population (75% rural, 50% urban) through the Public Distribution System (PDS): 5 kg of rice/wheat/millets per person per month at ₹1-3. This food security legislation is the nutritional safety net underlying all targeted nutrition programmes — without food adequacy, supplementary nutrition alone cannot address PEM.
SELF-CHECK
An Anganwadi worker provides supplementary nutrition to a 4-year-old child under ICDS. What is the correct daily caloric and protein provision under the ICDS supplementary nutrition norms for a child in this age group?
A. 300 kcal and 8 g protein
B. 500 kcal and 12-15 g protein
C. 600 kcal and 18-20 g protein
D. 700 kcal and 20 g protein
Reveal Answer
Answer: B. 500 kcal and 12-15 g protein
ICDS supplementary nutrition norms for children aged 6 months to 6 years: 500 kcal and 12-15 g protein per day. The higher allocation (600 kcal + 18-20 g protein) is for pregnant and lactating women. The 700 kcal + 20 g protein figure applies to PM POSHAN (MDM) for children in classes 6-8 (upper primary). The 300 kcal / 8 g protein figure does not correspond to any standard Indian programme norm. A 4-year-old falls in the 6-month to 6-year category (children's supplementary nutrition tier).