Page 16 of 32
CM5.{7-8,19} | CM5.{7-8,19} | Food Hygiene, Fortification and Food Labels — SDL Guide (Part 2)
Reading Food Labels — Nutritional Content and Regulatory Standards
Food labels are the primary interface between food science and consumer decision-making. Under FSSAI regulations (FSS Labelling and Display Regulations 2011, amended 2020), all packaged foods sold in India must carry specific mandatory label information. As a physician counselling patients — particularly those with diabetes, hypertension, or obesity — you need to read and interpret food labels fluently.
Mandatory label elements under FSSAI:
1. Product name (and common/generic name)
2. List of ingredients (in decreasing order of weight at the time of manufacture; allergens highlighted)
3. Nutritional information (per 100 g or 100 mL, AND per serving, in a standardised table format):
- Energy (kcal)
- Total fat (g); saturated fat (g); trans fat (g)
- Total carbohydrates (g); sugars (g); added sugars (g)
- Protein (g)
- Sodium (mg)
4. % Recommended Dietary Allowance (%RDA): For each nutrient listed in the nutrition panel, the percentage it contributes to the daily reference value (FSSAI uses 2000 kcal/day as the reference energy).
5. Allergen declaration (bold in the ingredient list or separate allergen statement): milk, eggs, tree nuts, peanuts, wheat, soy, fish, shellfish.
6. 'Best before' or 'use by' date and manufacturing date
7. FSSAI license number (14-digit number; mandatory for all food business operators)
8. Country of origin (for imported foods)
9. Net quantity (weight, volume, or count)
Key elements for clinical counselling:
- Added sugars: Distinguish from 'total sugars' (which includes naturally occurring sugars in fruit/dairy). Added sugars contribute empty calories and drive dental caries, obesity, and diabetes. WHO recommends <10% of total energy from free sugars (<5% for additional benefit); for 2000 kcal diet, this is <50 g/day (ideally <25 g/day). In ingredients list: 'sugar,' 'sucrose,' 'high-fructose corn syrup,' 'glucose syrup,' 'dextrose,' 'maltose,' 'fruit juice concentrate' are all added sugars regardless of their technical name.
- Trans fat: <0.5 g per serving is labelled as 'zero trans fat' in many countries; FSSAI limit for fats and oils is <2% trans fatty acids (from 2022). In packaged foods: 'partially hydrogenated vegetable oil' in the ingredient list indicates trans fat presence even if the nutrition panel says '0 g.'
- Sodium: Indian adults consume on average ~10-12 g salt/day vs WHO recommendation of <5 g. For hypertensive patients: aim for <1500 mg sodium/day (sodium × 2.5 = approximate salt equivalent). A single portion of many packaged snacks contains >500 mg sodium — one-third of the daily target.
- %RDA interpretation: A product claiming '25% of daily calcium needs per serving' means 4 servings would provide 100% of the reference RDA — but check the serving size; it is often set artificially small.
Front-of-Pack Nutrition Labels (FOPNL): FSSAI has proposed (and is deliberating on) mandatory front-of-pack labelling for packaged foods exceeding thresholds for fat, sugar, or sodium. Multiple formats exist globally (traffic light, nutri-score, warning labels). India's deliberations are ongoing; as of 2024, voluntary 'high in sugar/fat/sodium' icons are recommended.
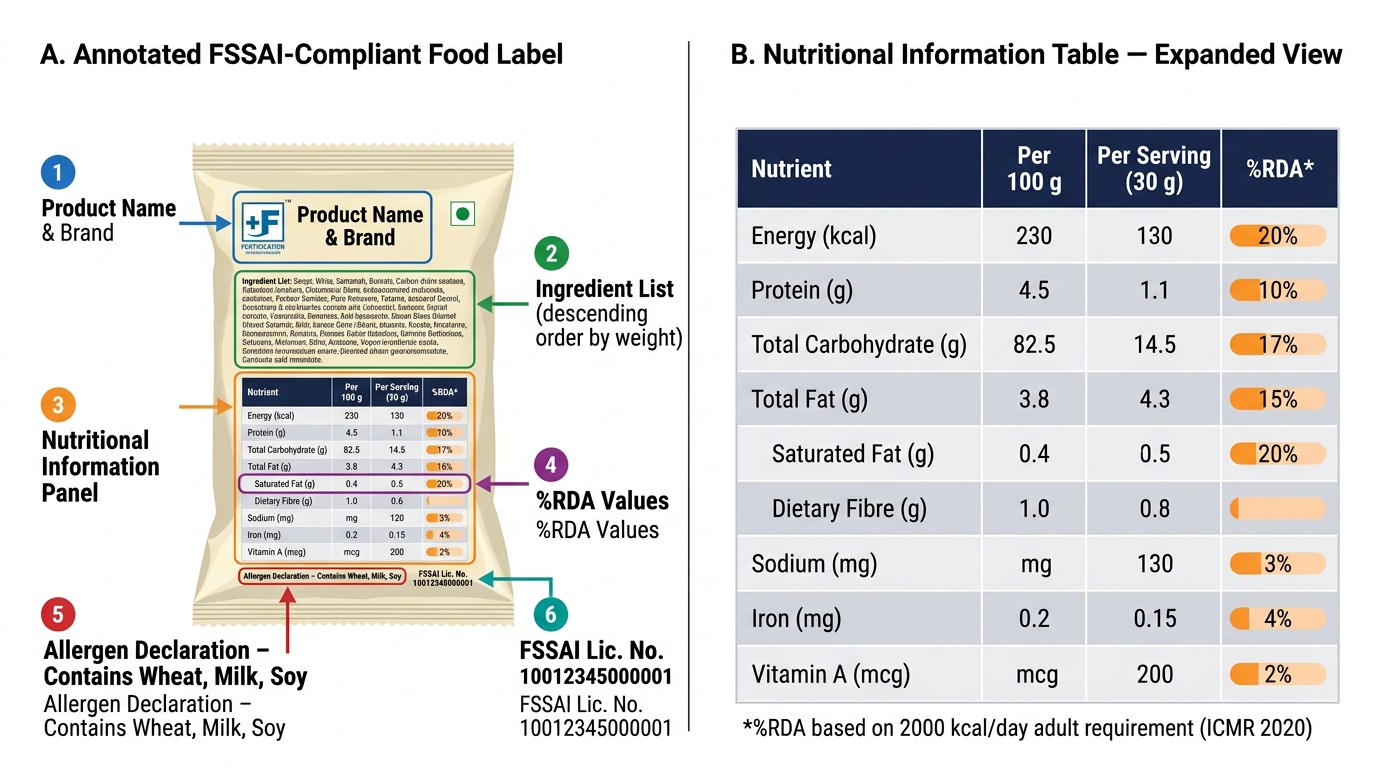
Anatomy of an FSSAI-Compliant Food Label
Evaluating Food Safety and Fortification Programmes
Food safety programme evaluation uses surveillance sampling — FSSAI's State Food Safety Officers collect food samples from markets, processing units, and retail outlets for laboratory testing at NABL-accredited food testing laboratories. Key indicators: percentage of samples tested that are 'not conforming' (adulterated or sub-standard); major adulterant detection rates; pesticide residue exceedance rates; aflatoxin contamination rates in groundnut and cereal samples. FSSAI publishes annual 'State of Food Safety' reports. Community-level rapid tests: adulteration detection kits (e.g. iodine test for starch adulteration in milk, 'synthetic milk' detection by sodium hydroxide + copper sulphate colour test) are distributed to PHCs and can be demonstrated to community health workers.
Fortification programme evaluation measures: (a) process — fortification coverage (% of salt/rice/oil meeting minimum fortification standards at point of sale, tested by FSSAI sampling); iodised salt household coverage (NFHS indicator, 93.7% in NFHS-5); (b) impact — micronutrient deficiency prevalence trends (anaemia NFHS, VAD surveys, NNMB iodine surveys). The government's PDS rice fortification programme is being evaluated through a large-scale intervention study tracking haemoglobin trends in ICDS and school children.
Key challenge: quality loss during the food chain. Iodine is lost from salt during storage, cooking (especially in the presence of moisture), and when exposed to sunlight — the consumer-level standard (15 ppm) accounts for this loss from the production standard (30 ppm). Similarly, Vitamin A in oil and milk can degrade if storage is improper (heat, light exposure). A fortification programme with high production-level compliance can fail to deliver if storage and distribution conditions are poor — an operational insight that community physicians should relay during outreach.
Counselling Patients on Food Safety and Informed Food Choices
The application of food hygiene, fortification, and label literacy knowledge is the clinical counselling encounter. Three patient scenarios illustrate the complete clinical skill:
Scenario 1 — A family presenting after a wedding feast gastroenteritis: Establish the timeline (incubation period), identify the likely food vehicle (shared meal, time-temperature violation), advise oral rehydration therapy. Counsel for future prevention: refrigerate cooked food within 2 hours, reheat to steaming hot (≥70°C), use safe water for cooking. Report to local FSSAI/Food Safety Officer if a catering establishment is implicated.
Scenario 2 — A pregnant woman asking which salt to buy: Confirm she is using iodised salt (NIDDCP mandate). Show her how to identify iodised salt on the label ('contains iodine' or 'iodised salt'). Explain the FSSAI +F logo. Reassure that iodised salt is mandatory for all licensed salt manufacturers and that almost all branded salt in India meets the standard. If she uses rock salt (sendha namak) or special artisanal salts — explain these are often NOT iodised and should be replaced with iodised salt during pregnancy (iodine requirement 220 µg/day in pregnancy).
Scenario 3 — A diabetic patient buying packaged biscuits: Walk through the nutrition label: check serving size (often 3-4 biscuits = one serving, but patients eat 8-10), multiply nutrient values by actual consumption. Identify added sugars in the ingredient list (glucose syrup, maltodextrin). Check sodium content (some 'healthy' biscuits have high sodium). Look for 'partially hydrogenated oil' indicating trans fat. Recommend whole grain, lower-sugar alternatives; teach the '5-20 rule' for %RDA: <5% = low, >20% = high for any nutrient. Empower the patient to make this comparison at the supermarket — this is CM5.19 in action.
Key counselling messages for all patients:
- Use only iodised salt for all cooking
- Look for FSSAI +F logo on purchased rice, oil, and flour for added micronutrients
- Avoid foods with 'partially hydrogenated oil' in the ingredient list
- Limit added sugar to <50 g/day (WHO recommendation); identify hidden sugars by name in ingredient lists
- For suspected adulteration (discolouration, unusual smell, texture): use FSSAI's free consumer app to report and get rapid testing guidance
SELF-CHECK
A patient with hypertension asks you about a popular packaged snack. The nutrition information panel states: serving size = 30 g, sodium = 380 mg per serving, servings per pack = 2.5. If the patient eats the entire pack, what is the total sodium intake, and how does this compare to the WHO recommended daily sodium limit?
A. 380 mg total; within WHO recommended limit of <2300 mg
B. 950 mg total; within WHO limit of <2000 mg
C. 950 mg total; represents approximately 47% of WHO recommended daily sodium limit of <2000 mg
D. 1140 mg total; exceeds the recommended daily limit of <1000 mg for hypertensives
Reveal Answer
Answer: C. 950 mg total; represents approximately 47% of WHO recommended daily sodium limit of <2000 mg
Total sodium = 380 mg/serving × 2.5 servings = 950 mg per full pack. WHO recommends <2000 mg sodium/day for adults (equivalent to <5 g salt/day). Therefore, 950 mg represents 950/2000 = 47.5% of the daily limit from a single snack — leaving only ~1050 mg sodium for the rest of the day's meals. For a hypertensive patient, many guidelines target ≤1500 mg/day, making this single snack-pack 63% of their daily allowance. This calculation demonstrates why label reading is a clinical skill: understanding per-serving vs per-pack values changes the clinical recommendation.
CLINICAL PEARL
'Partially hydrogenated vegetable oil' in the ingredient list is a red flag even when the nutrition panel says 0 g trans fat — and here is why. FSSAI regulations allow products with <0.5 g trans fat per serving to claim '0 g' on the nutrition label. If a serving size is set small enough, a product that actually contains 0.4 g trans fat per serving (within a single pack that contains 5 servings = 2 g trans fat total) can legally display '0 g trans fat' per serving. The only reliable way to detect trans fat presence is to look for 'partially hydrogenated oil' or 'hydrogenated fat' in the ingredient list. For patients with cardiovascular disease or high LDL: any food with 'partially hydrogenated' in the ingredient list should be avoided, regardless of what the nutrition panel says. This is why ingredient list literacy — not just nutrition panel literacy — is the complete clinical skill.