Page 2 of 15
CM11.{1,3-4} | CM11.{1,3-4} | Occupational Illness, Hazards and Ergonomics — SDL Guide (Part 2)
Prevention and Control of Occupational Hazards
Prevention of occupational disease follows an internationally recognised hierarchy of controls, which ranks interventions from most to least effective. This hierarchy is mandated under the Factories Act 1948 and endorsed by NIOSH (National Institute of Occupational Safety and Health) and the ILO. Moving down the hierarchy increases reliance on worker behaviour; moving up relies on engineering and design, which are more robust.
The hierarchy, from most to least effective:
1. Elimination — completely remove the hazardous agent or process. Example: banning asbestos (India banned chrysotile asbestos imports in 2011). This is the most effective control because it removes the hazard entirely.
2. Substitution — replace the hazardous substance with a safer alternative. Example: replace benzene with toluene (less leukemogenic) in rubber industries; substitute water-based paints for lead-based paints.
3. Engineering controls — modify the workplace or equipment to reduce exposure without relying on worker behaviour. This is the most feasible preventive tier in most workplaces:
- Enclosure of the dust-generating process (enclosed grinding units for stone cutting)
- Local exhaust ventilation (LEV): suction hoods at the point of dust/fume generation
- Wet drilling or wet-process grinding: water suppresses respirable silica dust by 80–90%
- Sound enclosures around noisy machinery (NIHL prevention)
4. Administrative controls — change work practices, schedules, or procedures:
- Job rotation to reduce individual exposure duration
- Work-rest schedules in heat stress environments
- Hazard Communication (HazCom): MSDS (Material Safety Data Sheets) for all chemicals; training workers on hazard recognition
- Pre-employment and periodic medical examinations (legally required under the Factories Act for specified occupations)
- Threshold Limit Values (TLVs): maximum ambient concentrations deemed safe for 8-hour daily, 40-hour weekly exposure, set by ACGIH (American Conference of Governmental Industrial Hygienists). Workplaces must monitor ambient air and ensure exposures remain below TLVs.
5. Personal Protective Equipment (PPE) — the last line of defence, used when engineering controls are insufficient. PPE does not reduce hazard — it reduces worker exposure:
- Respiratory: N95 particulate respirators (dusts), powered air-purifying respirators (PAPs) for higher concentrations
- Hearing protection: earmuffs or earplugs (required when noise > 85 dB(A))
- Gloves, aprons, boots: chemical hazards
- Eye and face protection: chemical splash, radiation
PPE must be appropriate, correctly fitted, consistently worn, and maintained — failure at any of these points renders it ineffective.
Specific preventive measures for agriculture: Pesticide safety requires: protective clothing during mixing and application (impervious gloves, boots, mask); prohibition of eating/drinking in pesticide-contaminated areas; safe storage (locked, labelled, away from food); use of low-toxicity formulations; worker training; biological control methods as substitution.
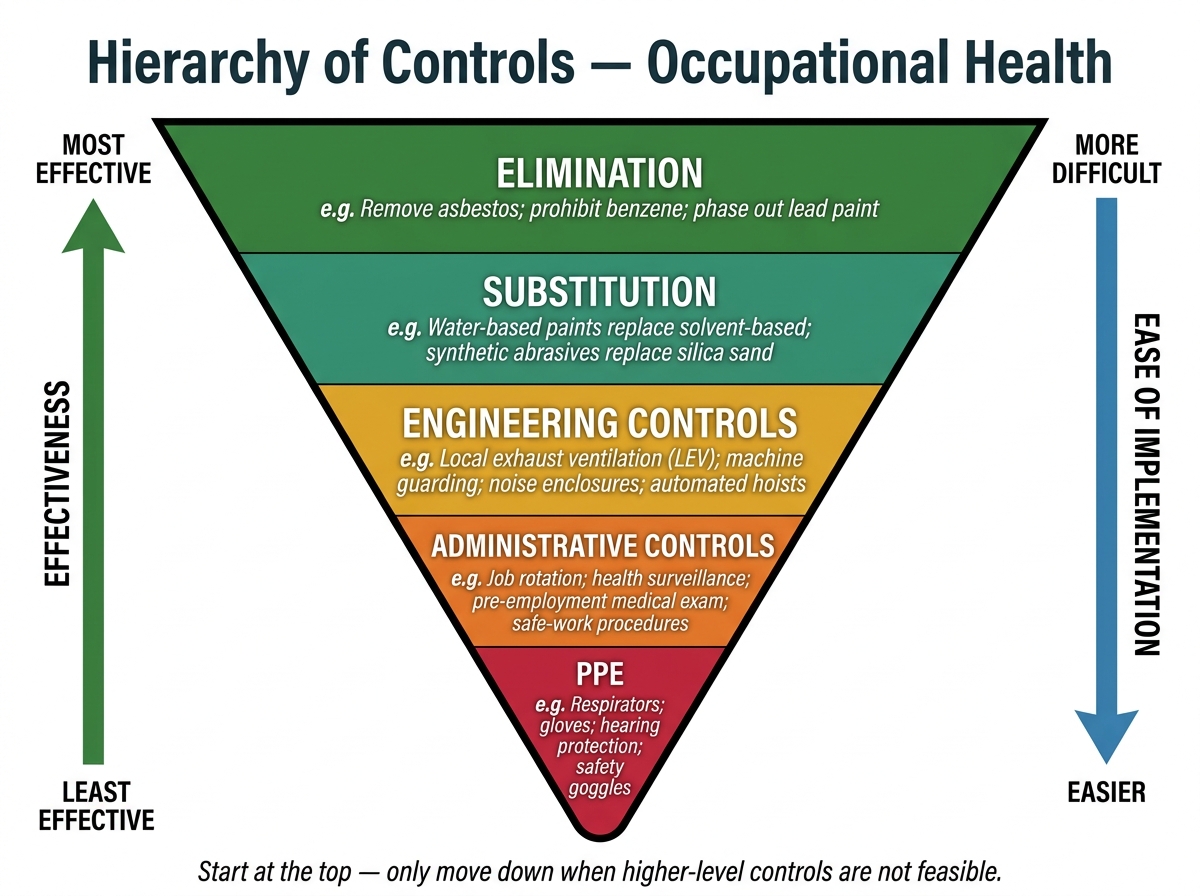
Hierarchy of Controls in Occupational Health
Ergonomics — Principles for Health Preservation
Ergonomics (from the Greek ergon = work, nomos = laws) is the scientific discipline concerned with designing the man-machine-environment system to optimise human performance and prevent injury. Its central principle is 'fit the job to the worker' rather than 'fit the worker to the job' — a foundational inversion that shifts responsibility from the individual to the system. Park's Textbook emphasises ergonomics as an upstream prevention strategy that complements engineering controls in reducing occupational musculoskeletal disorders (MSDs).
The man-machine-environment interface has three interacting components:
- The worker (anthropometric dimensions, physical capacity, cognitive load, fatigue)
- The machine/tool/task (tool design, force requirements, repetition rate, posture demands)
- The environment (illumination, temperature, noise, space, time pressure)
Mismatches at any interface generate ergonomic risk. The principal ergonomic risk factors for MSDs are:
- Repetition: high-frequency repeated movements deplete muscle glycogen and promote micro-tears (assembly-line workers, data entry operators)
- Awkward postures: sustained wrist flexion/extension (carpal tunnel syndrome), sustained neck flexion (cervical spondylosis in microscopists), prolonged forward trunk flexion (lumbar disc disease in farmers)
- Force: high grip force (pneumatic tool operators), manual materials handling (warehouse workers)
- Vibration: segmental vibration → vibration white finger (Raynaud's); whole-body vibration → lumbar disc degeneration
- Static loading: prolonged static muscle contraction without movement impedes blood flow and accelerates fatigue
Ergonomic Assessment Tools:
- RULA (Rapid Upper Limb Assessment): scores posture, force, repetition for upper limb MSDs; generates a risk score 1–7 (scores ≥4 require immediate investigation)
- NIOSH Lifting Equation (1994): calculates the Recommended Weight Limit (RWL) for a specific manual lifting task from six variables (horizontal distance, vertical height, lift frequency, asymmetry angle, coupling quality, lift duration). The Lifting Index (LI = actual load ÷ RWL) indicates injury risk — LI >1 means the task exceeds safe limits for the average worker.
- OWAS (Ovako Working Posture Analysis System): classifies trunk, arm, and leg postures into risk categories from observation
Workstation Design Principles (sitting workstations):
- Monitor at eye level, arm's length away (prevent cervical strain)
- Keyboard at elbow height with wrist in neutral (prevent carpal tunnel syndrome)
- Lumbar support at natural lordosis; feet flat on floor or footrest
- Frequent micro-breaks (5 min in every hour) to relieve static loading
Standing workstations (surgeons, dentists, factory floor workers): anti-fatigue mats, correct counter height, compression stockings, alternating weight shifting.
In agricultural settings, ergonomics addresses tool handle design (long-handled tools to prevent stooped posture), load-carrying methods (head-loading vs backpack carriers), and appropriate-technology interventions for smallholder farmers.
The public health dividend of ergonomics is substantial: MSDs are the leading cause of work disability in developed nations and a growing cause in India. An ergonomically designed workstation pays back in reduced absenteeism, worker retention, and productivity — arguments that factory managers and industrial health officers can use to justify investment.
Evaluation and Monitoring of Occupational Health Programmes
Evaluation of occupational health protection requires two complementary surveillance strategies: environmental monitoring (measuring hazards in the workplace) and biological monitoring (measuring hazard uptake in the worker). Together they provide a complete picture of actual worker exposure and enable early intervention before symptomatic disease develops.
Environmental monitoring involves systematic measurement of workplace air concentrations of chemical hazards (dusts, fumes, gases), physical parameters (noise levels, illumination, temperature), and biological agents. Results are compared against Threshold Limit Values (TLVs) (ACGIH) or Permissible Exposure Limits (PELs) (OSHA) or Occupational Exposure Limits (OELs) (Indian standards, NIOH). When environmental levels exceed limits, engineering controls must be upgraded — monitoring thus functions as a feedback mechanism for the control hierarchy.
Biological monitoring measures the internal dose in the worker's body — blood, urine, exhaled breath, or body tissue. Biological Exposure Indices (BEIs) correspond to the biomarker level when environmental exposure equals the TLV. Key biomarkers:
- Blood lead (Pb): BEI = 30 µg/dL (blood); workers above this level must be removed from exposure
- Urinary arsenic: BEI = 35 µg/g creatinine
- Cholinesterase activity (plasma or RBC): monitored in workers with organophosphate exposure; ≥20% reduction from individual baseline indicates significant exposure
- Urinary mandelic acid: toluene/styrene exposure marker
Biological monitoring is especially valuable for chemicals that are absorbed through skin (circumventing air-based monitoring) — organophosphates, solvents, and heavy metals are classic examples.
Medical surveillance of workers comprises three components:
1. Pre-employment medical examination: establishes individual baseline health status; identifies pre-existing conditions that increase susceptibility (e.g., pre-existing respiratory disease contraindicates silica-exposed jobs); legally required under the Factories Act for specified hazardous occupations.
2. Periodic medical examinations: conducted at mandated intervals (annual for most hazardous occupations; 6-monthly for high-risk categories under the Factories Act). Include targeted assessments — spirometry for dust-exposed workers, audiometry for noise-exposed workers, blood lead for battery workers, chest X-ray for miners.
3. Return-to-work examination: after occupational illness or injury; ensures fitness before re-exposure.
Notification of Occupational Diseases: Under Schedule III of the Factories Act 1948, 29 specific occupational diseases are notifiable — including silicosis, asbestosis, byssinosis, lead poisoning, mercury poisoning, and several others. The certifying surgeon (factory medical officer) must notify the chief inspector of factories within a defined period. Notification feeds the national occupational disease surveillance system and triggers investigation of the source workplace.
Programme evaluation indicators for an occupational health programme include: incidence rate of occupational injuries/diseases (primary outcome), absenteeism rate, compliance with TLV/OEL (process measure), coverage of pre-employment examinations, and employee satisfaction with health services.
SELF-CHECK
Which of the following is the MOST effective level in the hierarchy of controls for preventing silicosis in a stone-crushing unit?
A. Providing N95 respirators to all workers
B. Rotating workers between dusty and non-dusty tasks
C. Wet grinding process with enclosed crushing units and local exhaust ventilation
D. Conducting annual chest X-rays for all workers
Reveal Answer
Answer: C. Wet grinding process with enclosed crushing units and local exhaust ventilation
Engineering controls — wet grinding to suppress dust generation, enclosure of the process, and local exhaust ventilation — sit at the third (and most practical) tier of the control hierarchy, above administrative controls (job rotation) and PPE (respirators). Annual chest X-ray is medical surveillance, not a preventive control. N95 respirators are last-resort PPE. Wet drilling combined with enclosure/LEV is the highest-impact feasible intervention for stone-crushing silica control.