Page 5 of 15
CM11.{2,6} | CM11.{2,6} | Occupational Health Services and Insurance — SDL Guide
Learning Objectives
- Describe the role, benefits, and functioning of the Employees' State Insurance (ESI) Scheme (CM11.2)
- Manage occupational health services at factory or industry level in a simulated environment (CM11.6)
INSTRUCTIONS
India's industrial workforce is protected by two interlocking systems: a social insurance scheme (ESI) that compensates illness and disability, and a factory health service that prevents them. A physician posted as a factory medical officer operates at the intersection of both — identifying hazards, surveilling the workforce, managing the ESI benefits process, and navigating the legal obligations of the Factories Act. This module builds the competency to function in that role, from knowing the exact ESI contribution rates to designing a pre-employment medical protocol for a chemical manufacturing unit.
References
- Employees' State Insurance Act 1948 (India) — as amended (statute)
- Factories Act 1948 (India) — Chapters on Health, Safety, and Welfare (statute)
- Park's Textbook of Preventive & Social Medicine, 26th ed. — Chapter: Occupational Health (textbook)
- ESIC Annual Report 2022–23 — coverage and benefits statistics (report)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are appointed as the Medical Officer at a garment manufacturing unit in Tiruppur, Tamil Nadu, employing 800 workers — 650 women and 150 men. On your first day, you discover: no pre-employment medical records, the first-aid room has expired medications and no trained person, the ambient noise level exceeds 90 dB(A), and 200 workers earn less than Rs 15,000 per month and have never been registered under ESI despite the factory being an ESI-covered establishment. A worker presents with musculoskeletal pain that has caused her to miss 12 days of work, and she asks whether she is entitled to any payment for those days. You have one afternoon to develop an action plan. This module gives you the knowledge to act.
WHY THIS MATTERS
CM11.6 is a Skills competency — India's NMC expects Year-3 students to be able to manage occupational health services at the factory level in a simulated setting. This competency directly maps to roles graduates will hold: factory medical officer (FMO), occupational health consultant, district health officer monitoring industrial establishments, or clinician advising workers on entitlements. Understanding the ESI Scheme (CM11.2) is inseparable from this applied role — it determines what benefits workers receive, what the factory's obligations are, and how a physician certifies disease or disablement. Together, CM11.2 and CM11.6 form the 'health systems' layer of occupational medicine: knowing the hazards (CM11.1, CM11.3) is the clinical science; knowing the system (CM11.2, CM11.6) is the public health practice.
RECALL
Recall from the previous SDL (Occupational Illness, Hazards and Ergonomics): the five hazard categories (physical, chemical, biological, ergonomic, psychosocial); the hierarchy of controls (elimination → substitution → engineering → administrative → PPE); and the concept of occupational disease notification under the Factories Act. From your health systems lectures, recall the tripartite structure of social security — contributions from employers, employees, and government — a pattern you encountered in the National Health Mission and the Pradhan Mantri Jan Arogya Yojana. Also recall basic health administration: the role of inspectors, certifying surgeons, and the principle of notifiable diseases as a surveillance mechanism.
Occupational Health Services — Global Burden and India's Legislative Framework
Access to occupational health services remains profoundly unequal. The ILO estimates that fewer than 15% of workers globally — and a smaller fraction in low-and-middle-income countries — have access to any occupational health service. In India, the organised sector (factories, mines, railways, government) has regulated occupational health services under the Factories Act 1948 and sector-specific legislation; the unorganised sector — accounting for over 90% of India's workers — has almost no formal occupational health coverage.
This inequity has two legislative responses in India, which together form the backbone of the formal occupational health system:
The Employees' State Insurance (ESI) Act 1948 — enacted alongside independence as part of India's welfare state architecture — established a compulsory, contributory social health insurance scheme for workers in factories and specified establishments. It is administered by the Employees' State Insurance Corporation (ESIC), a statutory body under the Ministry of Labour and Employment. The ESI scheme provides comprehensive medical care plus cash benefits for sickness, maternity, disability, and death to insured workers and their dependants.
The Factories Act 1948 — India's primary occupational safety and health law — imposes direct obligations on factory occupiers (owners/managers) to provide health, safety, and welfare facilities. Chapter III of the Factories Act specifically addresses health provisions: cleanliness, disposal of wastes, ventilation and temperature, lighting, sanitary conveniences, and employment of a certifying surgeon to conduct medical examinations. The Act also mandates specific facilities based on workforce size (ambulance room, canteen, crèche), and requires notification of occupational diseases listed in Schedule III.
These two statutes interact in practice: a worker with an occupational disease may receive medical treatment through the ESI system, while the factory is simultaneously required to notify the inspector of factories under the Factories Act and may face enforcement action. The factory medical officer sits at the junction of both systems — clinician, administrator, and public health officer simultaneously.
The ESI Scheme — Structure, Coverage, and Benefits
The Employees' State Insurance Scheme is a tripartite, contributory social insurance system — meaning its funds come from three sources: employers, employees, and the government. Understanding the contribution structure is essential because eligibility for benefits is tied to contribution compliance.
Contribution rates (as revised in 2019):
- Employer contribution: 3.25% of the worker's wages
- Employee contribution: 0.75% of wages
- Government contribution: bears cost of medical benefit administration (approximately 1/8th of total medical benefit costs) and provides land/buildings for ESIC facilities in some states
Coverage eligibility — Wage Ceiling:
Workers earning up to Rs 21,000 per month are compulsorily covered under ESI (Rs 25,000 for persons with disabilities). Once insured, a worker retains full ESI benefits regardless of wage changes during the benefit period. Workers earning above the ceiling may opt out or are covered under the Employees' Compensation Act instead.
Who is covered: All employees (including contract workers) in:
- Factories employing ≥10 persons (with or without power, as extended by state governments)
- Specified establishments: shops, hotels, restaurants, roads, motor transport undertakings, printing presses, newspaper establishments, educational/medical/cinema institutions employing ≥10 persons
- ESIC has extended coverage progressively — all 36 states and union territories are now covered
The Six Categories of ESI Benefits:
1. Medical benefit: Full medical care for insured persons and their dependants from day 1 of insurable employment. No premium deductible, no co-payment. Provided through ESIC hospitals (157 hospitals), dispensaries (1,500+), and panel clinics. Includes outpatient, inpatient, specialist, diagnostic, pharmaceutical, and rehabilitative care.
2. Sickness benefit: Cash payment of 70% of daily average wages for a maximum of 91 days in two consecutive benefit periods (each benefit period = 6 months). Eligibility: insured for ≥70 days in the corresponding contribution period. Covers certified sickness requiring absence from work.
- Extended sickness benefit: For 34 specified long-term diseases (TB, malignancy, mental illness, stroke, cardiac disease, etc.) — 70% wages for up to 2 years at the full rate, after exhausting ordinary sickness benefit.
- Enhanced sickness benefit: 100% wages for up to 7 days for male insured persons undergoing vasectomy / 14 days for female insured persons undergoing tubectomy.
3. Maternity benefit: 100% wages for 26 weeks (as per Maternity Benefit Amendment Act 2017, which extended from 12 to 26 weeks for first two children). 12 weeks for women with 2 or more children. Requires 70 days of insurable employment in the two preceding contribution periods.
4. Disablement benefit:
- Temporary disablement benefit: 90% of wages for the entire period of certified temporary disablement (no maximum period). Payable from day 1 of injury — does not require a minimum contribution period (unlike sickness benefit).
- Permanent disablement benefit: Pension for life at 90% wages, proportional to the assessed degree of permanent disability. If disablement is ≥40%, it is treated as permanent total disablement.
5. Dependants' benefit: Pension to dependants (widow + children) of an insured worker who dies from employment injury or occupational disease, at 90% of wages distributed per family.
6. Other benefits: Funeral expenses (Rs 15,000 lump sum); rehabilitation allowance; vocational rehabilitation.
ESIC administrative structure: The ESI Corporation is governed by a tripartite General Body (representatives of workers, employers, government, medical profession). Regional offices manage State-level administration. Medical Services are provided through ESIC's own hospitals and dispensaries plus panel doctors under the MOU.
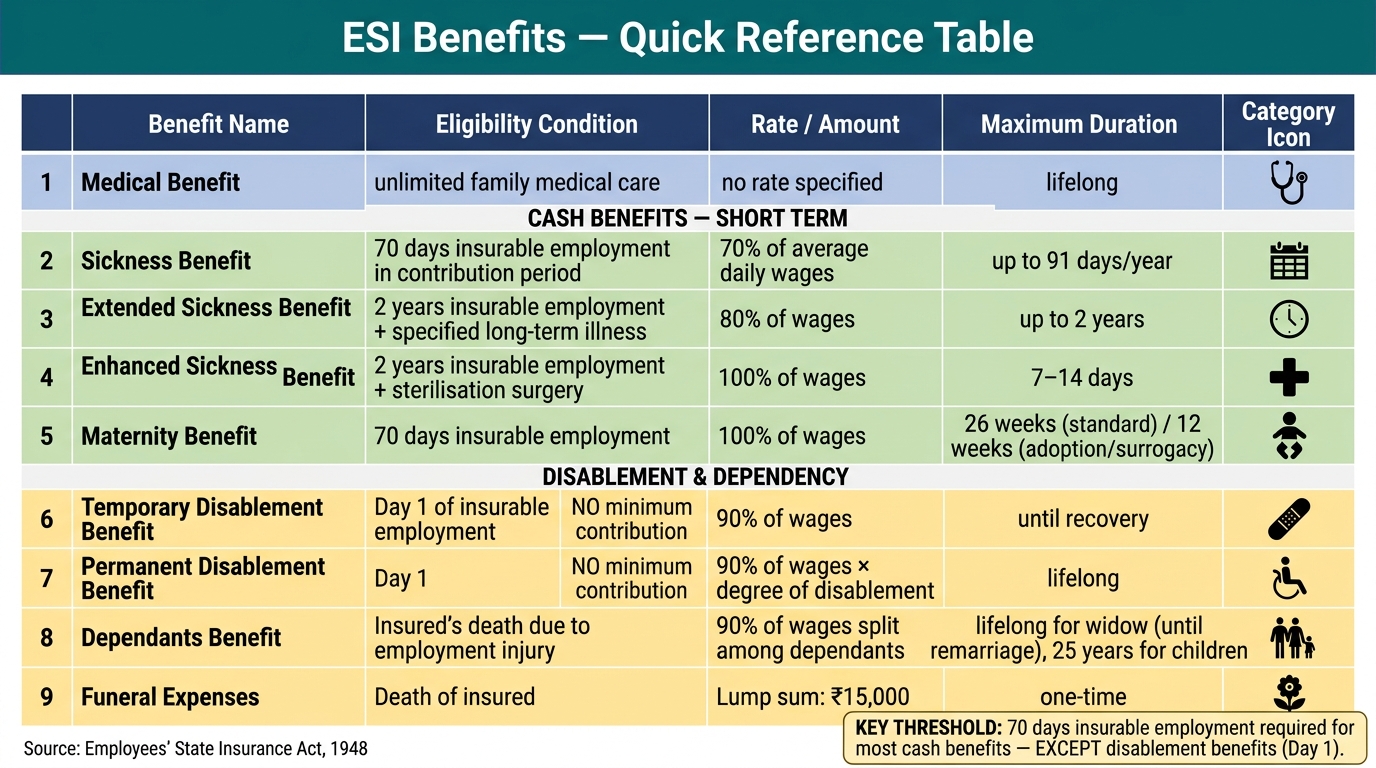
ESI Benefits — Summary Reference Table
SELF-CHECK
An insured worker sustains a machinery injury on her first day of work in a factory. She is temporarily disabled for 45 days. Which ESI benefit applies, and what is the payment rate?
A. Sickness benefit at 70% of wages; requires 70 days of prior contributions
B. Temporary disablement benefit at 90% of wages; payable from day 1 without minimum contribution period
C. Medical benefit only; cash benefits require 3 months of contributions
D. Disablement benefit at 70% of wages; requires employer notification within 48 hours
Reveal Answer
Answer: B. Temporary disablement benefit at 90% of wages; payable from day 1 without minimum contribution period
Temporary disablement benefit under ESI is payable from day 1 of insurable employment for employment-related injuries — no minimum contribution period is required. The rate is 90% of daily average wages (not 70%, which applies to sickness benefit). Sickness benefit requires 70 days of insurable employment in the preceding contribution period. The 90% rate for disablement reflects the higher severity and work-attributable cause.
Factory-Level Occupational Health Services — Structure and Functions
A factory occupational health service is the operational unit through which preventive, curative, and rehabilitative occupational health care is delivered at the workplace. The Factory Medical Officer (FMO) — also called the certifying surgeon in the context of the Factories Act — is the physician responsible for this service. The FMO must be a qualified medical practitioner certified by the Chief Inspector of Factories. India requires one FMO per factory with specific worker thresholds (details vary by state rules under the Factories Act).
The functions of a factory health service span five domains:
1. Health Surveillance — Pre-employment and Periodic Medical Examinations
Pre-employment examination establishes baseline health status before workplace exposure begins. It includes: full medical history, physical examination, vision and hearing assessment, spirometry (for dust-exposed work), X-ray chest (for silica/asbestos-exposed), and baseline blood/urine biochemistry. The purpose is dual: (a) identify pre-existing conditions that increase susceptibility to specific hazards (e.g., asthma contraindicates silica-exposed work); (b) establish individual baselines for future comparison.
Periodic medical examination monitors for early signs of occupational disease at mandated intervals:
- Annual: for workers exposed to specified hazardous processes (Schedule 2 of the Factories Act — 29 hazardous processes including lead, asbestos, chrome, manganese, silica)
- 6-monthly: for certain high-risk exposures
- Examinations include job-specific tests: spirometry for dust-exposed workers, audiometry for noise-exposed workers, blood lead for battery/paint workers, cholinesterase activity for pesticide applicators
Under the Factories Act, the certifying surgeon must maintain a health register for each worker in scheduled hazardous processes and report cases of occupational disease to the Inspector of Factories.
2. Treatment and First Aid
The Factories Act mandates first-aid provision based on workforce size:
- All factories: First-aid box (one per 150 workers), stocked per the prescribed list, in charge of a trained person
- Factories with ≥500 workers: Ambulance room with prescribed equipment and a qualified nurse; the room must be in charge of a qualified medical practitioner during working hours
- Factories with ≥1,000 workers: Full factory hospital
The FMO manages these treatment services: acute workplace injuries, occupational disease treatment initiation, ESI benefit certification, and referral coordination.
3. Occupational Hygiene and Environmental Monitoring
The FMO must liaise with the factory safety officer and safety committee to ensure regular environmental monitoring:
- Dust concentrations (silica, asbestos, coal) measured against TLVs/OELs
- Noise measurements compared against the 85 dB(A) permissible limit
- Chemical air sampling for toxic gases, solvents, and fumes
- Temperature and humidity control in heat-stress industries (steel, ceramics, bakeries)
The FMO reviews monitoring reports and triggers control upgrades when values exceed limits — this is the feedback link between occupational hygiene and the hierarchy of controls.
4. Rehabilitation and Return-to-Work Programmes
Following occupational illness or injury, the FMO coordinates: fitness-for-work assessment, phased return-to-work planning, job modification or temporary alternative placement, and liaison with ESIC for disablement benefit certification. The Factories Act requires modified duty for workers recovering from scheduled process exposures.
5. Health Promotion and Education
Factories are a captive setting for targeted health promotion. The FMO organises: hazard communication training (Material Safety Data Sheets, correct PPE use), anti-tobacco programmes, blood pressure/diabetes screening in workers, nutrition education, and mental health awareness (shift work, stress). The Factories Act mandates welfare officers for factories with ≥500 workers — the FMO and welfare officer together constitute the core of the factory health system.
Welfare facilities mandated by the Factories Act (workforce thresholds):
- ≥150 workers: First-aid box (one per 150)
- ≥250 workers: Canteen (subsidised meals)
- ≥500 workers: Ambulance room, Welfare officer
- ≥30 female workers: Crèche (day care for children up to 6 years)
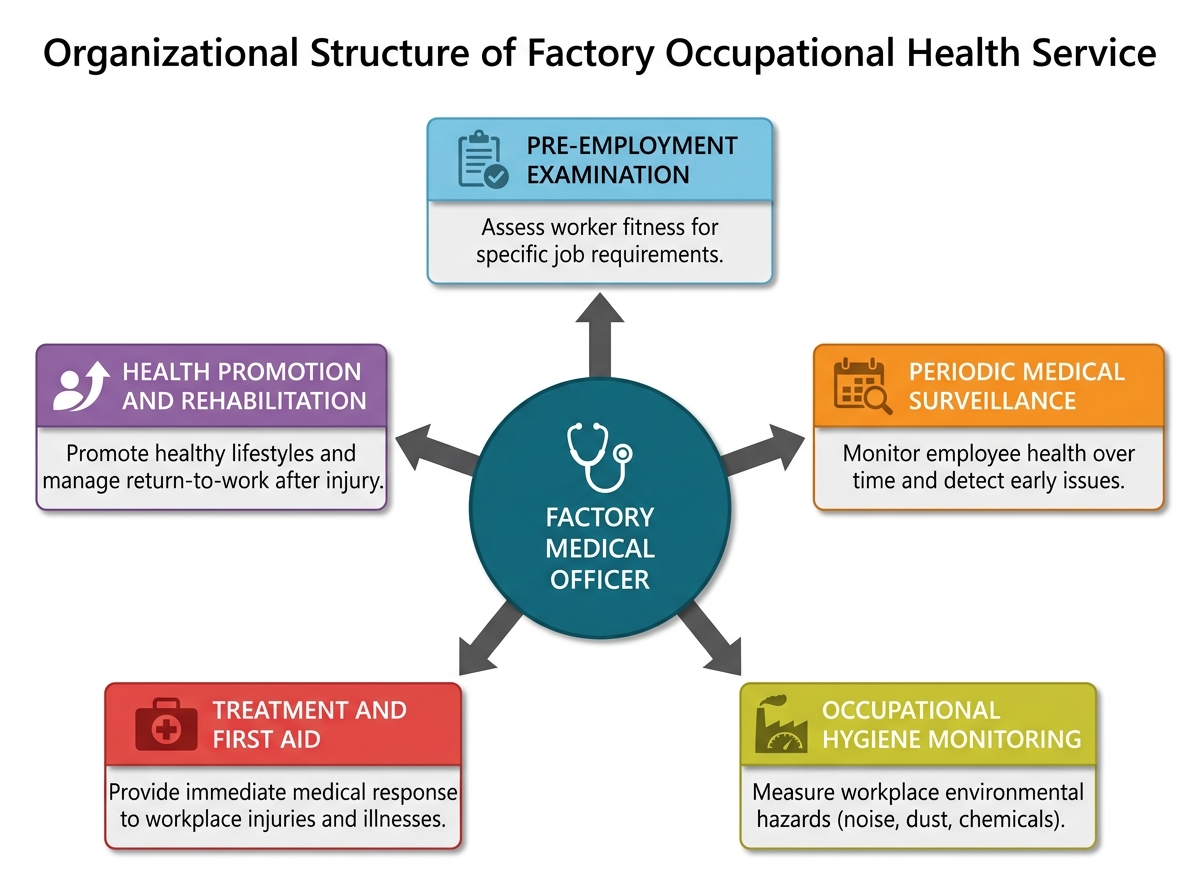
Organizational Structure of a Factory Occupational Health Service
SELF-CHECK
Under the Factories Act 1948, which of the following welfare facilities is mandated for a factory employing 300 workers?
A. Ambulance room and a qualified nurse
B. Canteen providing subsidised meals
C. Factory hospital with resident doctor
D. Crèche for children of all workers
Reveal Answer
Answer: B. Canteen providing subsidised meals
A canteen is mandatory for factories employing ≥250 workers. An ambulance room is required for ≥500 workers. A factory hospital is required for ≥1,000 workers. A crèche is required for factories employing ≥30 female workers (not all workers, and not tied to 300 as a threshold). At 300 workers, only the canteen threshold (≥250) is crossed in this list.