Page 4 of 27
CM10.3 | CM10.3 | Pregnancy, Childbirth and Feeding Practices — SDL Guide
Learning Objectives
- Describe local customs and practices during pregnancy, childbirth, lactation, and child feeding, and classify them by health impact
- Explain why harmful traditional practices persist and outline a community-based approach to modifying them
INSTRUCTIONS
Cultural practices around pregnancy and childbirth are not abstract sociological curiosities — they are direct determinants of neonatal tetanus rates, breastfeeding coverage, and malnutrition prevalence in your catchment population. A PHC medical officer who cannot distinguish beneficial from harmful traditions, or who lacks the communication skills to counsel families without causing offence, will fail to reduce the avoidable deaths in their jurisdiction. This module bridges community medicine and behavioural science through the lens of India's feeding and birthing traditions.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch 11 & Ch 20 (Nutrition) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An ANM in a Rajasthan village documents that of the last 20 deliveries in her area, 14 were conducted at home by a local dai using a shared, unsterilised blade to cut the cord. Twelve of those 20 babies were denied colostrum because the family believed the 'first milk is dirty.' Seven of the 20 mothers had avoided dal and eggs throughout pregnancy on the advice of their mother-in-law, who said protein foods 'make the baby too big.' Three newborns had died in the neonatal period — two from neonatal tetanus, one from neonatal diarrhoea. What systematic changes in community engagement could have prevented these deaths?
WHY THIS MATTERS
Traditional practices around pregnancy, delivery, and feeding are not random — they are coherent belief systems with deep social roots, and they respond poorly to lecturing. As a public health physician you will encounter them daily: in ANC sessions, in ASHA supervision meetings, in community health education. Understanding which practices cause harm, why families persist with them, and how to counsel respectfully and effectively is one of the most applied skills in this curriculum — and one of the few that requires as much social intelligence as medical knowledge.
RECALL
From your nutrition module, recall that protein-energy malnutrition in the first 1,000 days (conception to age 2) causes irreversible stunting and cognitive deficits. From immunology, recall that maternal IgG crosses the placenta to provide neonatal passive immunity for the first few months, and that secretory IgA is the primary antibody in human breast milk — meaning that colostrum and mature breast milk are immunological shields that formula cannot replicate. From epidemiology, recall that neonatal tetanus (caused by Clostridium tetani contaminating the cord stump) is preventable both by TT immunisation of the mother and by clean cord-cutting practices — and that it is a notifiable disease with a near-100% case fatality in home settings without intensive care.
Burden of Harmful Traditional Practices on RMNCH Outcomes
Harmful traditional practices are not a minor modifying factor in RMNCH mortality — in many rural communities they explain a substantial fraction of neonatal and infant deaths. The clearest pathway is from unclean cord-cutting practice to neonatal tetanus: when a dai uses a shared, unsterilised blade, sickle, or bamboo sliver to cut the umbilical cord and applies cow dung, ash, or untreated oil to the stump, Clostridium tetani spores enter the wound. Neonatal tetanus (trismus neonatorum) presents at 3-10 days of life with jaw stiffness, inability to feed, and generalised spasms; without ventilatory support its case fatality exceeds 90%. India has nearly eliminated neonatal tetanus at national level (NNT elimination declared 2015), but pockets persist in states with low TT coverage and high home-delivery rates. The second major pathway is nutritional: dietary taboos during pregnancy that restrict protein foods (fish, eggs, dal in some communities), milk, and fruit because of cultural beliefs (e.g., 'eggs make the baby bald,' 'papaya causes abortion') contribute directly to maternal protein deficiency, iron deficiency anaemia, and low birth weight. The third pathway involves prelacteal feeding — giving honey, sugar water, formula, or goat's milk before the first breastfeed: this delays milk let-down, introduces early pathogen exposure, and is associated with a three-fold higher risk of neonatal diarrhoea. Finally, early weaning before 6 months removes the protective effect of exclusive breastfeeding, leading to early introduction of contaminated complementary foods and a sharp increase in diarrhoeal and respiratory illness incidence.
Determinants: Why Traditional Practices Persist
Traditional practices around birth and feeding persist not because communities are irrational but because they are embedded in social structures that confer authority, identity, and perceived safety. The dai occupies a position of trusted expertise that has been built over generations — she is present at every delivery, she charges less than a facility, she speaks the local language, and she practises in the home where the woman feels safe. Displacing her without replacing her social function creates a vacuum, not a solution. Elder authority in joint families — particularly mothers-in-law — shapes nearly every decision about diet, delivery location, and newborn care: a young pregnant woman who ignores her mother-in-law's dietary advice faces social consequences within the household. Poverty forces trade-offs: institutional delivery requires transport money, facility fees (even if theoretically free), lost wages, and the cost of staying near the facility — all of which drive families back to home delivery. Low health literacy means that the germ theory of neonatal tetanus is not intuitive — the connection between a blade and a death ten days later is not visible. Religious and ritual beliefs attach meaning to specific practices: colostrum denial may be linked to a belief that the spirit enters the baby only after a ritual is performed, and applying turmeric or oil to the cord stump may be a protective ritual in the family's cultural framework. Effective behaviour change communication must engage these determinants, not dismiss them.
SELF-CHECK
A mother gives her 4-day-old baby a teaspoon of honey before the first breastfeed. What is the most significant immediate health risk?
A. Hyperglycaemia due to high sugar content
B. Increased risk of neonatal diarrhoea and delayed milk let-down
C. Suppression of neonatal immunity by interfering with maternal IgG
D. Neonatal botulism from Clostridium botulinum spores in honey
Reveal Answer
Answer: D. Neonatal botulism from Clostridium botulinum spores in honey
Honey given to a neonate carries the specific risk of infant botulism — Clostridium botulinum spores in honey can germinate in the neonatal gut, producing botulinum toxin that causes descending flaccid paralysis. This is a unique neonatal risk (the adult gut resists germination). Option B (diarrhoea and delayed milk let-down) also occurs with prelacteal feeds generally, but is not the 'most significant immediate' risk of honey specifically. Honey is explicitly contraindicated in children under 1 year for this reason.
Practices During Pregnancy
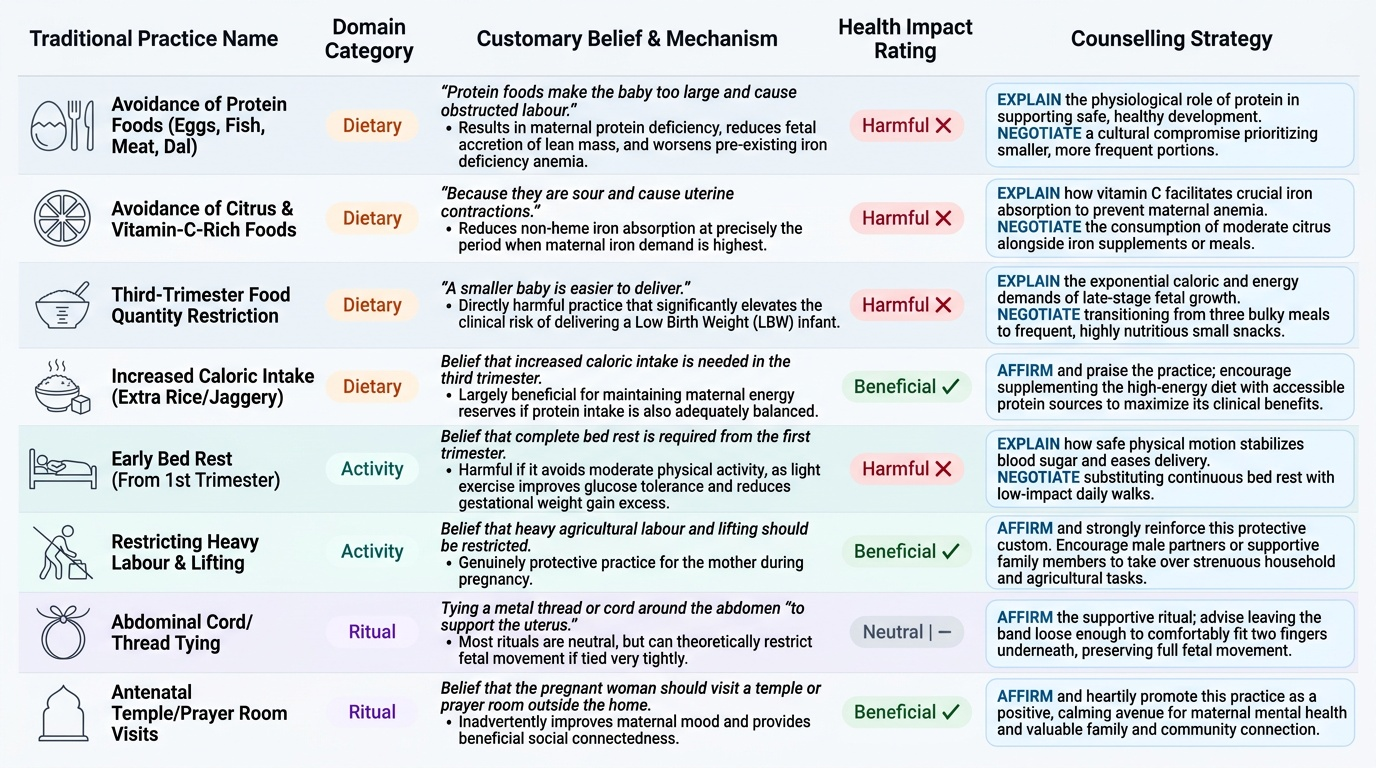
Pregnancy practices span dietary, activity, and ritual domains, and their health impact ranges from beneficial to neutral to frankly harmful. A structured assessment of local customs begins with this three-category framework. Dietary taboos are the most nutritionally consequential: avoidance of protein foods (eggs, fish, meat, dal) based on beliefs such as 'protein foods make the baby too large and cause obstructed labour' results in maternal protein deficiency, reduces foetal accretion of lean mass, and worsens pre-existing iron deficiency anaemia. Avoidance of citrus and vitamin-C-rich foods 'because they are sour and cause uterine contractions' reduces non-haem iron absorption at precisely the period when iron demand is highest. Some communities restrict food quantity in the third trimester based on the belief that a smaller baby is easier to deliver — this is directly harmful and increases LBW risk. Conversely, some communities prescribe increased caloric intake (extra rice, jaggery) in the third trimester — this is largely beneficial if protein intake is also adequate. Activity restrictions: complete bed rest from the first trimester is harmful if it extends to avoidance of all moderate physical activity, as light exercise improves glucose tolerance and reduces gestational weight gain excess. But restrictions on heavy agricultural labour and lifting are genuinely protective. Ritual practices: tying a metal thread or cord around the abdomen 'to support the uterus' can theoretically restrict fetal movement if very tight; most cord-tying rituals are neutral. Antenatal rituals that require the woman to visit a temple or prayer room (outside the home) may inadvertently improve her mood and social connectedness — a neutral-to-beneficial effect. The counselling principle is to affirm the beneficial and neutral practices, explain the mechanism of harm for the harmful ones, and negotiate a culturally acceptable modification.
Provided image