Page 12 of 27
CM10.5 | CM10.5 | Immunization and Childhood Illness Programmes — SDL Guide
Learning Objectives
- Describe the Universal Immunization Programme including the current vaccine schedule, cold chain requirements, and monitoring indicators
- Describe the IMNCI programme and its Assess-Classify-Treat approach for integrated management of childhood illnesses
INSTRUCTIONS
India's Universal Immunization Programme is one of the largest public health programmes in the world, targeting approximately 27 million newborns annually. Yet one in four Indian children remains incompletely immunized (NFHS-5), and each missed dose represents a preventable death. As a community medicine practitioner you will manage immunization sessions, maintain the cold chain, calculate dropout rates, and conduct catch-up campaigns. This module gives you the technical foundation to do all of these — and to explain to a parent exactly why each vaccine is given at its specific age.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch 5 (Immunology) & Ch 11 (RMNCH) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An ANM at a sub-centre is conducting the monthly Village Health and Nutrition Day session. A mother arrives with her 14-month-old child for the first time — no immunizations given since birth. The ANM has OPV, DPT booster, and MR vaccine in her carrier. She is unsure: can she give multiple vaccines today, or must she follow the original schedule? And she has no IPV in her carrier — is IPV catch-up required at 14 months? The mother has to travel 8 km to reach the CHC for IPV. The ANM must make a decision on the spot, with limited supplies and a queue of 15 other children waiting.
WHY THIS MATTERS
Immunization is the highest-impact preventive intervention in child survival — the WHO estimates that vaccines prevent 2-3 million deaths globally every year. As a PHC medical officer you are legally and programmatically responsible for the immunization coverage in your catchment: if an unimmunized child dies of measles in your jurisdiction, it is an adverse programme outcome that the district CMO will investigate. Beyond the ethics, understanding the UIP schedule cold — every vaccine, every age, every route, every dose — is essential for MCQs, the IMNCI certification examination, and field competency.
RECALL
From your physiology and immunology sessions, recall that vaccines work by stimulating active immunity — they prime the immune system to generate antigen-specific memory B and T cells without causing clinical disease. Herd immunity protects unvaccinated individuals when the proportion immune in a population exceeds the herd immunity threshold (which varies by vaccine: measles requires ~95% coverage because of its high R₀ of 12-18). From the cold chain module, recall that vaccines are biological products that denature irreversibly if exposed to temperatures above 8°C (for most antigens) or freeze damage (for DTP, Hepatitis B, Pentavalent — shake test detects freeze damage). Vaccine Vial Monitor (VVM) is a heat-sensitive label on each vaccine vial that changes colour when cumulative heat exposure exceeds safe limits — always check VVM before using any vaccine.
Disease Burden Addressed by UIP and Childhood Illness Programmes
The diseases targeted by the UIP represent the major vaccine-preventable causes of under-5 mortality and morbidity in India's epidemiological profile. Tuberculosis: despite the BCG vaccine not preventing adult pulmonary TB, it is highly effective (70-80%) at preventing the severe childhood forms — tuberculous meningitis and miliary TB — which carry high mortality and neurological morbidity. Poliomyelitis: before 1985 and the onset of the Universal Immunization Programme, tens of thousands of children in India were paralysed by wild poliovirus annually; India was certified polio-free by WHO in 2014, with the last wild case in January 2011 (West Bengal). The risk of vaccine-derived poliovirus emergence now requires continued IPV supplementation alongside OPV. Diphtheria, Tetanus, Pertussis: diphtheria causes a fibrinous membrane in the throat (bull-neck, myocarditis); pertussis (whooping cough) kills through apnoeic spells in infants under 6 months; neonatal tetanus kills through generalised spasms — all three are preventable with DTP vaccination. Measles: a highly contagious paramyxovirus with R₀ of 12-18 (requiring 95%+ coverage for herd immunity); causes pneumonia, diarrhoea, encephalitis, and blindness through vitamin A depletion; India accounted for a disproportionate share of global measles deaths before MR vaccine scale-up. Hepatitis B: vertical (mother-to-child at delivery) and horizontal transmission drives high HBsAg carrier rates in India; Hepatitis B birth dose prevents perinatal infection in 90%+ of cases when given within 24 hours. For childhood illnesses, IMNCI targets the five major causes of under-5 mortality: diarrhoea (leading cause in early childhood), acute respiratory infection/pneumonia, malaria (in endemic districts), malnutrition, and ear infection (a significant cause of childhood deafness).
Determinants of Immunization Coverage and Cold Chain Integrity
Achieving and sustaining high immunization coverage requires simultaneously addressing supply-side and demand-side barriers, plus maintaining the technical integrity of the cold chain. Supply-side determinants include: reliability of vaccine supply (stock-outs at sub-centre level are a common cause of missed sessions); functional cold chain equipment (a broken ice-lined refrigerator at the CHC can fail an entire district's monthly session); availability of trained staff on immunization session days; and consistent scheduling of VHND sessions so communities can plan. Demand-side determinants include: awareness of the immunization schedule (first-generation literate families often do not know that the 9-month and 14-16 month visits are necessary after the 14-week series is complete); distance to outreach session (sub-centres serving large geographic areas have catchments where some families must walk 5+ km to reach a session); vaccine hesitancy (a growing concern after rumours about polio drops in some communities); and opportunity cost (agricultural families avoid sessions during harvest season — effective scheduling accounts for the local agricultural calendar). The dropout rate — calculated as (DTP1 coverage minus DTP3 coverage) / DTP1 coverage × 100 — is the single most actionable immunization programme indicator at PHC level: a dropout rate above 10% signals a systemic barrier between the early visits (6 weeks) and the completion visit (14 weeks), usually either cold chain breakdown, missed outreach sessions, or loss of follow-up for migrant families.
SELF-CHECK
A sub-centre has DTP1 coverage of 85% and DTP3 coverage of 62% among children under 1 year. What is the dropout rate, and what programme action is indicated?
A. Dropout rate = 27%; this is acceptable as coverage is above 60%
B. Dropout rate = 27%; this exceeds the 10% threshold and requires investigation of barriers between 6-week and 14-week sessions
C. Dropout rate = 23%; acceptable because the absolute DTP3 coverage is above 50%
D. Dropout rate = 23%; requires immediate suspension of outreach sessions pending investigation
Reveal Answer
Answer: B. Dropout rate = 27%; this exceeds the 10% threshold and requires investigation of barriers between 6-week and 14-week sessions
Dropout rate = (DTP1 - DTP3) / DTP1 × 100 = (85 - 62) / 85 × 100 = 27.1%. A dropout rate above 10% is the programme threshold for investigation. The correct action is to audit the reasons for dropout: are there missed outreach sessions? A cold chain failure that made families distrust the vaccine? A high proportion of migrant families? DTP3 coverage of 62% is well below the 90% national target, confirming this is a priority sub-centre. Option C and D have an arithmetic error — the correct dropout rate is 27%, not 23%.
Universal Immunization Programme: Schedule and Vaccines
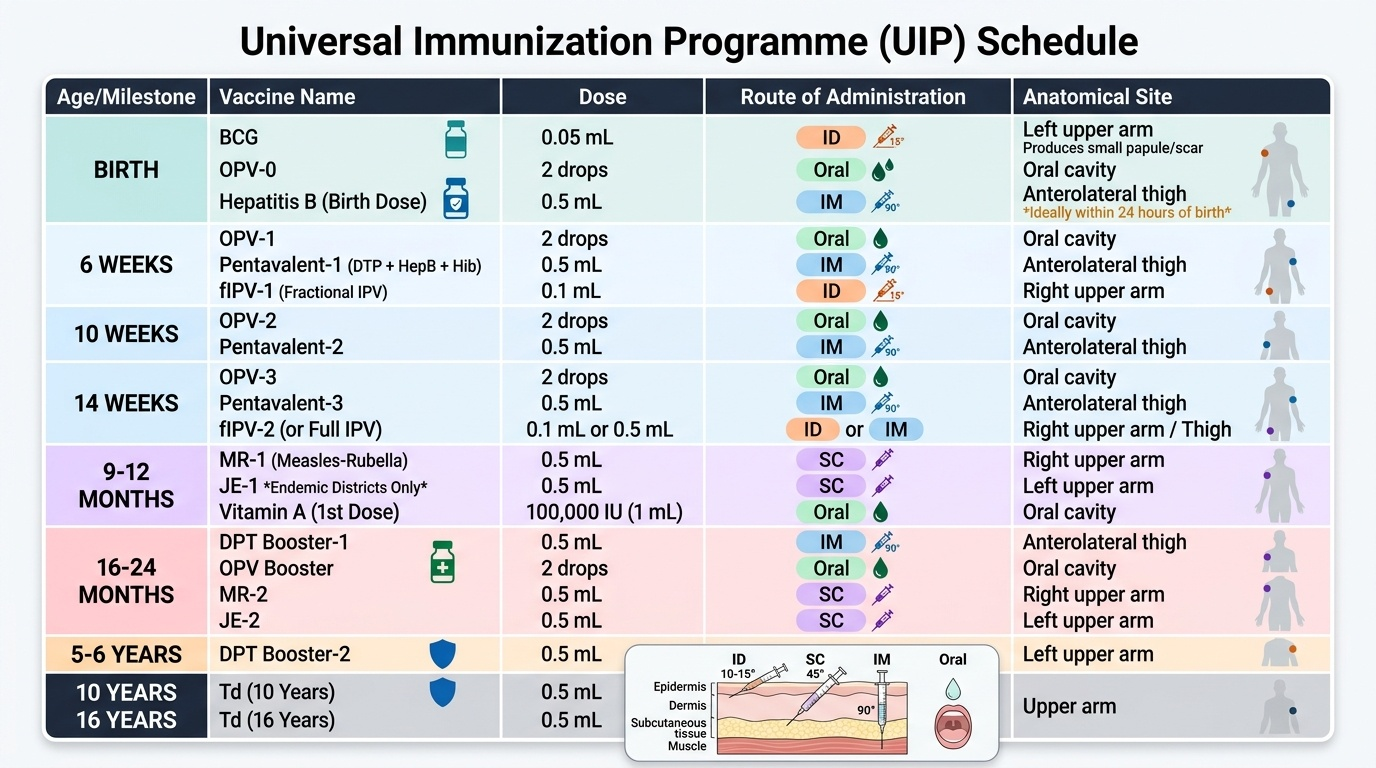
The UIP schedule is organised by age of administration, and the sequencing reflects the age-specific vulnerability to each disease and the timing of maternal antibody wane. At birth (or as early as possible up to age 1 year), the following vaccines are given: BCG (0.05 mL intradermal into the left upper arm, using a 26-gauge needle angled at 15°, producing a bleb that becomes a local papule and scar); OPV-0 (2 drops oral); and Hepatitis B birth dose (0.5 mL IM into the anterolateral thigh). The Hepatitis B birth dose must ideally be given within 24 hours of birth to maximise prevention of perinatal infection. At 6, 10, and 14 weeks, the following are given at each visit: OPV (2 drops oral), Pentavalent vaccine (0.5 mL IM into the anterolateral thigh — contains DTP + Hepatitis B + Hib combined), and IPV (0.1 mL fractional intradermal dose at 6 weeks, in states with fractional-dose IPV schedule, or 0.5 mL IM at 14 weeks in full-dose schedules — state protocols vary). At 9-12 months: MR vaccine (Measles-Rubella, 0.5 mL subcutaneous), Japanese Encephalitis (JE) vaccine (in JE-endemic districts — SA-14-14-2 live attenuated, 0.5 mL subcutaneous), and Vitamin A first dose (100,000 IU oral). At 16-24 months: DPT booster (0.5 mL IM), OPV booster (2 drops oral), MR second dose (0.5 mL subcutaneous), and Vitamin A second dose (200,000 IU oral). At 5-6 years: DPT second booster (0.5 mL IM). At 10 years and 16 years: TT (Tetanus Toxoid, 0.5 mL IM). For children coming late without any prior immunisation, a catch-up schedule is used: all vaccines appropriate for age are given simultaneously on a single visit, then the remaining doses are completed at minimum intervals — there is no need to restart the series.
Provided image