Page 4 of 11
CM2.3-5 | CM2.3-5 | Health Seeking Behaviour and Community Relationships — SDL Guide
Learning Objectives
- Describe and assess barriers to good health and health-seeking behaviour in individuals and communities
- Explain social psychology, community behaviour, and community relationships and their impact on health and disease
- Describe poverty and social security measures in India and their relationship to health and disease
INSTRUCTIONS
Why do patients delay seeking care even when they know something is wrong? Why do communities reject vaccines despite evidence of their effectiveness? This module explores the psychological, social, and economic forces that shape health-seeking behaviour — and gives you the tools to assess and address those forces in your practice.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 26th ed. Bhanot Publishers, 2023. Chapters: Social Psychology in Community Health; Poverty and Health; Social Security in India; Health Behaviour and Health Education (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Meena is a 35-year-old woman in a peri-urban settlement near Pune. She noticed a breast lump four months ago but told no one. When she finally came to the government hospital, she was diagnosed with Stage III breast cancer. She delayed because she feared what her husband would say, because she could not afford the bus fare and the lost day of wages, because she did not know this hospital offered free care, and because a neighbour told her the lump was 'just fatty tissue.' Four separate barriers — social, economic, informational, and cultural — conspired to steal four crucial months. Understanding why Meena delayed, and how to systematically assess these barriers, is what this module is about.
WHY THIS MATTERS
Health-seeking behaviour is not primarily a matter of individual willpower or intelligence — it is shaped by a complex web of social, psychological, and economic forces that lie mostly outside the clinic. Community medicine's power lies in identifying and modifying these forces before they result in preventable death and disability. India's NFHS-5 data show stark differentials in care utilisation by wealth quintile, education, gender, and region — differentials that cannot be explained by disease burden alone. Competencies CM2.3, CM2.4, and CM2.5 equip you to assess these forces systematically: to identify barriers in individual patients, understand community dynamics that amplify or dampen health behaviour, and connect vulnerable patients to the social security architecture that exists to support them.
RECALL
From the previous SDL on socio-cultural assessment (CM2.1–2.2), you learned that social determinants of health operate at structural and intermediary levels, and that socio-economic status profoundly shapes a family's access to resources. You also learned that cultural beliefs and family structure influence health decisions. This SDL builds directly on those foundations: the barriers to health seeking are the operational face of the structural and intermediary determinants you have already mapped. Recall also the WHO definition of health as a state of complete physical, mental, and social well-being — the social dimension is front and centre in what you are about to learn.
Magnitude of Under-utilisation: How Many Seek Care and Why It Matters
Health service under-utilisation is a quantitatively large and well-documented problem in India. National Family Health Survey-5 (NFHS-5, 2019–21) data reveal that a substantial proportion of Indians who are ill do not seek formal medical care, particularly in rural areas, among women, and in the lowest wealth quintiles. The consequences are measurable: delayed treatment of tuberculosis extends transmission; delayed presentation of maternal complications drives India's maternal mortality ratio; delayed cancer diagnosis (as in Meena's case) collapses five-year survival rates. Understanding the magnitude of under-utilisation is the necessary first step — it justifies the investment in identifying and removing barriers.
Under-utilisation is not a homogeneous problem: it operates differently across conditions, communities, and health system levels. For preventive care (immunisation, antenatal visits, cancer screening), utilisation gaps are well-documented and wide. For curative care, the pattern depends on cost, severity perception, and provider availability. A community medicine practitioner must quantify both the extent of the problem (what proportion of the target population is not accessing a service) and its patterning (which sub-groups are systematically excluded and by what mechanism).
Population surveys using structured questionnaires measure health-seeking behaviour at community level. Key metrics include: the proportion of ill persons who sought formal care within 48 hours; the proportion who completed a recommended treatment course; and the proportion who utilised preventive services (antenatal care ≥4 visits, full immunisation by age 12 months). These metrics, when disaggregated by sex, education, SES class, and geography, reveal the social gradient in utilisation that drives the community health diagnosis.
- NFHS-5: key data source for India-level and state-level utilisation patterns
- Under-utilisation: measurable gap between need and actual care sought
- Metrics: proportion seeking care within 48 hrs, treatment completion, preventive service coverage
- Patterning by SES, gender, geography reveals which barriers are operating
SELF-CHECK
In a village survey, 100 children under-5 were found to have diarrhoea in the past two weeks. Of these, 62 received treatment from a qualified practitioner. 20 used home remedies only, and 18 received no treatment. Which metric best quantifies the health-seeking behaviour gap?
A. Disease burden — 100 children with diarrhoea
B. Treatment completion rate — proportion who finished the course
C. Formal care utilisation rate — 62% sought qualified care
D. Incidence rate — new diarrhoea cases per 1000 children
Reveal Answer
Answer: C. Formal care utilisation rate — 62% sought qualified care
The formal care utilisation rate (62%) directly quantifies the health-seeking gap — it shows that 38% of sick children did not receive formal care. Disease burden describes magnitude of illness, not of behaviour. Treatment completion applies after care is sought. Incidence measures disease occurrence, not care-seeking.
Barriers to Health Seeking Behaviour
The most widely used framework for understanding health service utilisation is the Andersen Behavioural Model (Ronald Andersen, 1968, updated 1995). This model organises the determinants of health care use into three categories: predisposing factors (characteristics of individuals that exist before the onset of illness and increase or decrease the probability of using services), enabling factors (resources that allow or prevent the use of services), and need factors (the actual or perceived health problem that motivates service use). A barrier to health seeking is anything within these categories that reduces utilisation below the level needed for good health.
Predisposing factors include socio-demographic characteristics (age, sex, education, marital status, family size), social structure (occupation, ethnicity, social networks), and health beliefs (attitudes toward modern medicine, perceived severity of illness, fatalism). In the Indian context, predisposing barriers are especially prominent: women may need a husband's or in-law's permission to seek care; men may be conditioned to deny illness as weakness; lower-caste individuals may distrust a system they have historically experienced as discriminatory. Education level is a powerful predisposing factor — it shapes a person's ability to recognise symptoms, navigate the health system, and understand medical advice.
Enabling factors are the practical means by which a person accesses care: household income and the ability to pay out-of-pocket costs, health insurance coverage, physical distance to a facility, availability of transport, waiting times, and availability of a same-sex provider. In India, the most critical enabling barriers are economic (out-of-pocket expenditure is among the highest in the world as a proportion of health spending) and geographic (facility distribution skewed toward urban areas). The PM-JAY health insurance scheme attempts to address the economic enabling barrier for low-income families; however, awareness of entitlement and ability to navigate the scheme are themselves barriers within the enabling domain.
Need factors represent the perceived or evaluated health need that triggers utilisation. Perceived need (the individual's own sense of illness) may differ radically from evaluated need (the clinician's assessment). If a person does not perceive a symptom as serious, they will not seek care regardless of enabling resources. Cultural explanations of illness (attributing symptoms to supernatural causes, a dietary imbalance in Ayurvedic terms, or the 'evil eye') can suppress perceived need for biomedical care even when evaluated need is high.
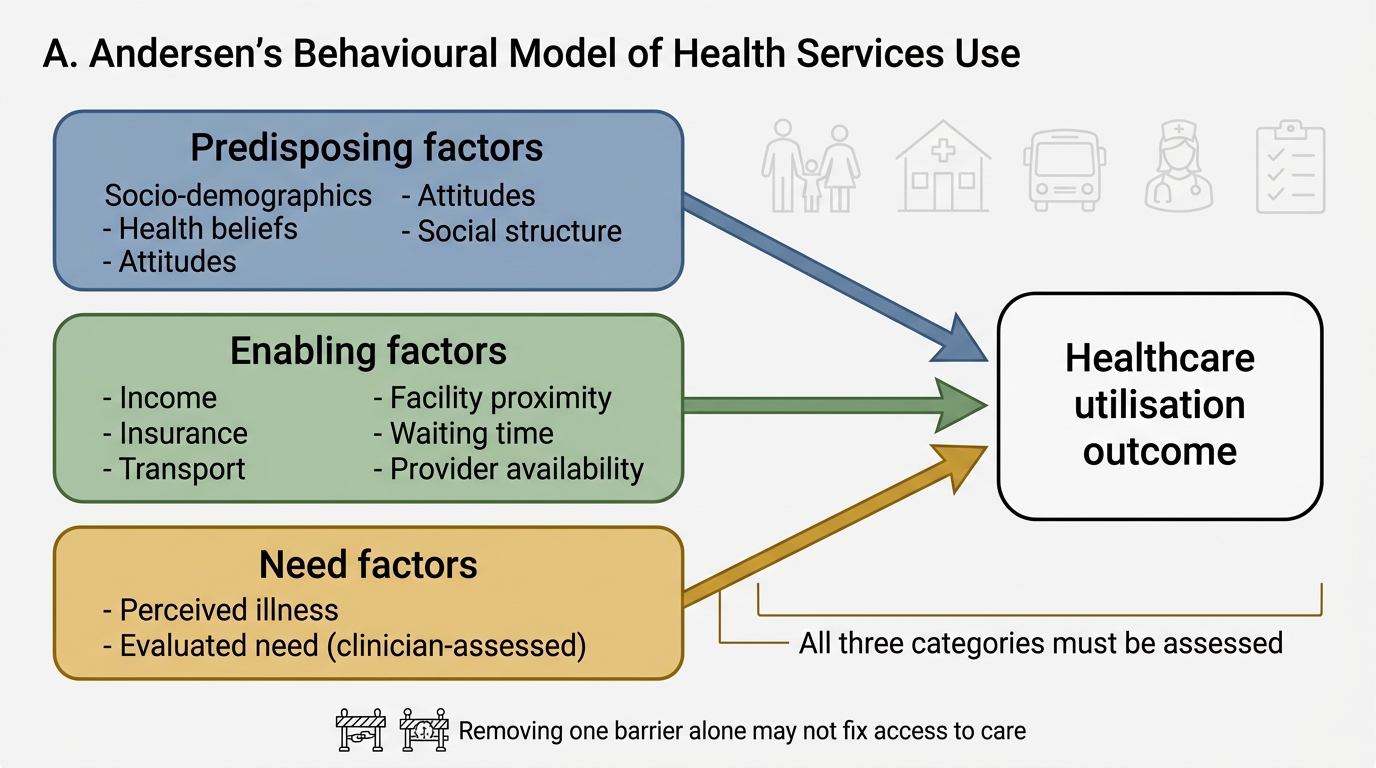
Andersen's Behavioural Model of Health Services Use
- Predisposing: socio-demographics, health beliefs, attitudes, social structure
- Enabling: income, insurance, transport, facility proximity, waiting time, provider availability
- Need: perceived illness vs evaluated (clinician-assessed) need
- All three categories must be assessed — removing one barrier does not fix the system
Social Psychology, Community Behaviour, and Community Relationships
Social psychology studies how individuals' thoughts, feelings, and behaviours are influenced by others — whether real, imagined, or implied. Its concepts are directly relevant to community health because health behaviour is fundamentally social: what people eat, whether they vaccinate their children, whether they seek care, and how they respond to health messages are all shaped by social forces that operate at the community level.
Three foundational social psychology concepts govern community health behaviour. Attitudes are evaluative predispositions — a person's learned tendency to respond favourably or unfavourably toward a health behaviour, service, or provider. Attitudes are shaped by direct experience, observation of others (social learning), and social norms. A negative attitude toward institutional delivery (e.g. believing hospitals are cold and impersonal while home births are natural and safe) is a predisposing barrier to skilled birth attendance. Beliefs are cognitive acceptances — propositions held to be true, often without empirical verification. Health-relevant beliefs include beliefs about disease causation (germ theory vs supernatural causation vs humoral imbalance), treatment efficacy (antibiotic effectiveness vs traditional remedies), and one's own susceptibility to illness. The Health Belief Model explicitly places these as determinants of health behaviour. Social norms are the shared rules and expectations that govern behaviour in a group; they may be descriptive (what most people do) or injunctive (what people are expected to do). In a community where male sterilisation is socially stigmatised (an injunctive norm), even men who might personally be willing to accept vasectomy will resist for fear of social consequences.
Community relationships encompass the patterns of interaction, trust, authority, and reciprocity within a community. Communities have formal leadership structures (elected local bodies like gram panchayat, village health committees, self-help groups) and informal leadership (respected elders, religious leaders, traditional healers). Health programmes that engage community leaders achieve better uptake because they work with existing authority structures rather than against them. Social capital — the network of relationships and the associated norms of trust and reciprocity — is a health-protective resource: communities with strong social capital show better communicable disease control, better maternal and child health outcomes, and greater resilience to health shocks.
Negative community dynamics can amplify disease. Discrimination against individuals from stigmatised groups (persons with HIV, tuberculosis patients, persons with disabilities) drives them away from care-seeking and creates hidden pockets of untreated disease. Rumours and misinformation — particularly potent in high-social-cohesion communities where word-of-mouth is trusted — can collapse immunisation coverage rapidly, as seen in vaccine hesitancy episodes in India. The community health worker (ASHA) and the Village Health, Sanitation and Nutrition Committee (VHSNC) are the front-line structures for harnessing positive community dynamics and monitoring negative ones.
- Attitudes: evaluative predispositions shaped by experience, social learning, and norms
- Beliefs: cognitive propositions about disease causation, susceptibility, and treatment efficacy
- Social norms: descriptive (what people do) and injunctive (what people are expected to do)
- Community relationships: formal leadership (panchayat, VHSNC) + informal (elders, healers) + social capital
- Negative dynamics: stigma, rumour, misinformation — amplify disease and suppress care-seeking
SELF-CHECK
In a rural community, the gram panchayat president publicly states that measles vaccination is not needed because 'the disease has always come and gone on its own.' Vaccination coverage in the village drops by 30% within a month. Which social psychology mechanism best explains this effect?
A. Perceived need — villagers no longer believe they are susceptible
B. Injunctive social norm — a respected authority figure has communicated what the community is expected to do
C. Enabling barrier — the panchayat has withheld transport to the vaccination site
D. Predisposing factor — the villagers have a negative attitude toward vaccination by nature
Reveal Answer
Answer: B. Injunctive social norm — a respected authority figure has communicated what the community is expected to do
The panchayat president's statement functions as an injunctive norm signal — it communicates the socially expected behaviour (not vaccinating). The drop in coverage follows social conformity to that expectation, not a change in perceived susceptibility (which would be a need-factor mechanism) or transport access (enabling barrier). Attitudes can change from social norm signals, but the primary mechanism described here is normative social influence.