Page 3 of 13
DR1.2 | Acne Management Planning — SDL Guide (Part 3)
Hormonal and Adjunctive Therapies in Female Acne
Hormonal Therapy for Female Acne
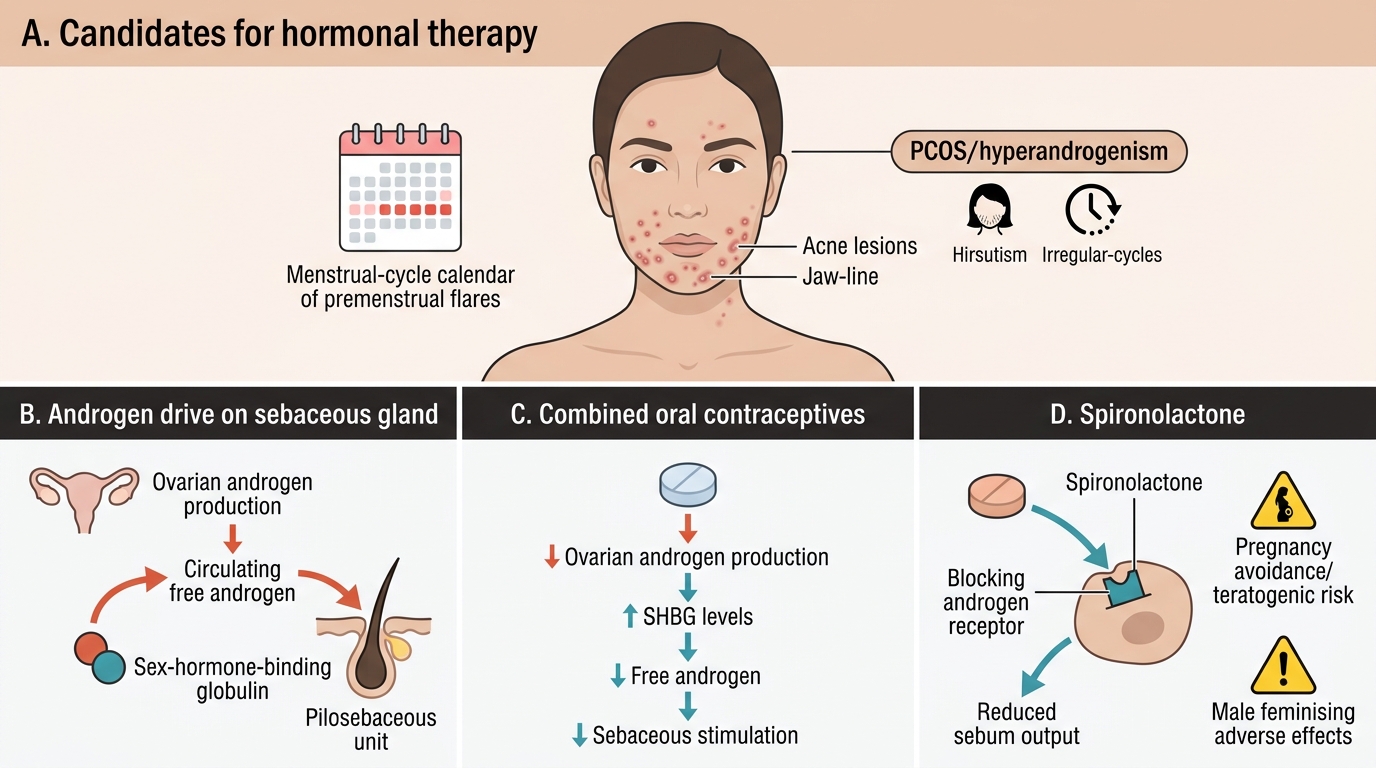
Hormonal therapy is a valuable and often under-used option for women whose acne has a hormonal pattern, and recognising when to reach for it rounds out the management toolkit. It is particularly suited to adult women with acne distributed over the lower face and jaw-line, premenstrual flares, persistence beyond adolescence, or frank signs of hyperandrogenism such as hirsutism and irregular cycles — including those with PCOS. The two main approaches both reduce the androgenic drive on the sebaceous gland. Combined oral contraceptives (COCs) lower circulating free androgens (by suppressing ovarian androgen production and raising sex-hormone-binding globulin), and certain progestins add anti-androgenic effect. Spironolactone, an aldosterone antagonist, blocks the androgen receptor and reduces sebum; it is used off-label for female acne and is not given to men for this purpose because of feminising effects. These agents are slow to act and are typically combined with standard topical therapy rather than used alone. Their contraindications must be respected: spironolactone is teratogenic-risk and is avoided in pregnancy, and COCs are contraindicated in women with thromboembolic risk, certain migraines, or other standard contraindications.
Key points for hormonal therapy:
- Best candidates: adult women with jaw-line/hormonal-pattern acne, premenstrual flares, or hyperandrogenism (including PCOS).
- Combined oral contraceptives: reduce free androgens and raise SHBG; respect thromboembolic and other standard contraindications.
- Spironolactone: androgen-receptor blocker, off-label, effective in women; avoid in pregnancy; not used in men for acne.
- Expect a slow response (several cycles) and combine with topical therapy; these are adjuncts, not stand-alone cures.
For a woman with severe or refractory hormonally-driven acne, hormonal therapy and isotretinoin are not mutually exclusive choices but options to be weighed with the patient and the dermatologist.
CLINICAL PEARL
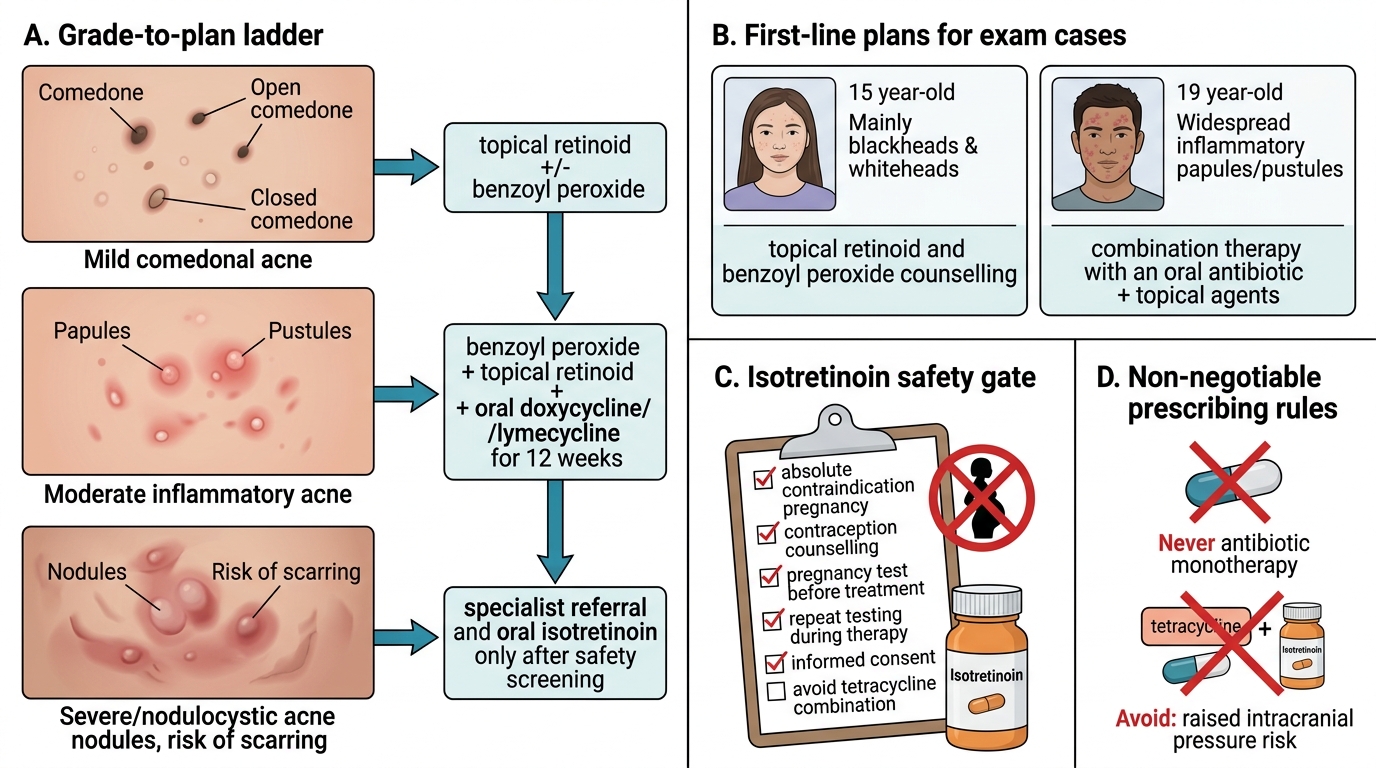
The most important single rule in all of acne management is that isotretinoin is absolutely contraindicated in pregnancy and demands rigorous pregnancy prevention. Before prescribing it to any woman of childbearing potential, confirm a negative pregnancy test, ensure effective contraception (ideally two methods) is in place, and arrange repeat testing during treatment, following your local programme. A second, frequently-tested pearl: never use oral antibiotics as monotherapy and never combine an oral tetracycline with isotretinoin — antibiotic monotherapy breeds C. acnes resistance, and the tetracycline–isotretinoin combination risks benign intracranial hypertension. A third practical pearl: most apparent 'treatment failure' is really poor adherence or too short a trial — confirm the patient actually used the regimen for 8–12 weeks before escalating.
Self-Assessment: Building an Acne Management Plan
Acne Management Plan: Grade-to-Treatment and Safety Rules
Use the following structured prompts to consolidate your ability to convert a severity grade into a safe, individualised management plan and to handle the safety-critical decisions that surround systemic therapy. For each prompt, commit to a concrete plan — name the drugs, state the combinations and the duration, and articulate the counselling and safety steps you would give the patient — and then check yourself against the principles in this module. The aim is to make the grade-to-plan reasoning automatic and to embed the non-negotiable safety rules so firmly that you would never, for example, hand isotretinoin to a woman without addressing pregnancy prevention, or prescribe an antibiotic alone. These self-checks deliberately mirror the short-answer, case, and reasoning questions you will meet in examinations and in the everyday outpatient department.
- For a 15-year-old with mainly blackheads and whiteheads and only a few small papules, write the first-line plan and the key counselling points.
- For a 19-year-old man with widespread inflammatory papules and pustules (moderate), write the plan including the antibiotic rule and its duration.
- State the absolute contraindication of oral isotretinoin and list, from memory, the mandatory pregnancy-prevention steps for a woman of childbearing potential.
- Explain why oral antibiotics are never used as monotherapy in acne, and why a tetracycline must not be combined with isotretinoin.
- For a 26-year-old woman with jaw-line acne, premenstrual flares, and irregular cycles whose acne failed topical therapy, give the best adjunctive options and one investigation you would consider.