Page 5 of 13
DR1.1 | Acne Recognition and Grading — SDL Guide
Learning Objectives
- Recognise and correctly name the primary acne lesions — open and closed comedones, papules, pustules, nodules, and cysts
- Explain the four pillars of acne pathogenesis (sebum, follicular hyperkeratinisation, Cutibacterium acnes, inflammation) and link each to a treatment target
- Identify the major risk factors and triggers for acne, including hyperandrogenic states warranting investigation
- Grade acne severity using the IGA and GAGS scales and distinguish acne vulgaris from its common mimics
INSTRUCTIONS
Acne is the commonest skin disease of adolescence and one of the most frequent reasons a young person consults any doctor in India. The diagnosis is made by looking carefully and naming what you see, and the severity grade you assign determines the entire treatment plan that follows. This module builds the recognition-and-grading skill from the ground up — lesion morphology, the four-pillar pathogenesis that explains both the lesions and their treatment, the risk factors that sharpen recognition, formal severity grading, and the differentials that masquerade as acne — so that you can convert a vague complaint of 'pimples' into a precise, defensible clinical assessment.
References
- Neena Khanna. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Acne (textbook)
- IADVL Textbook of Dermatology. Ch: Acne and Acneiform Eruptions (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 17-year-old boy is brought to your skin OPD by his mother. For the past year he has had spots on his face that 'come and go,' but lately the cheeks have developed tender red lumps that leave dark marks for weeks. He has stopped going to college functions, sits at the back of the classroom, and his mother quietly tells you he barely speaks at home anymore. On examination you see scattered blackheads over the forehead, several red papules and pustules on both cheeks, and two deep tender nodules along the jaw. This is acne vulgaris — the most common skin disease of adolescence, affecting up to 80% of people between 11 and 30 years. The diagnosis is made entirely by looking carefully and naming what you see. This module teaches you to recognise each lesion type and to grade severity, because that grade is what will determine the entire treatment plan.
WHY THIS MATTERS
Acne is one of the commonest reasons a young person walks into any clinic in India — general practice, paediatrics, or dermatology — so every MBBS graduate must be able to recognise and grade it confidently. Getting the grade right matters far beyond cosmetics: a mild comedonal acne needs only a topical agent, whereas a severe nodulocystic acne left under-treated will scar permanently and can cause profound psychological distress, including depression and social withdrawal, exactly as you saw in the boy above. Misjudging severity in either direction wastes months — under-treatment lets scars form, over-treatment exposes a patient to needless drug risk. The ability to look at a face, name the lesions, and assign a severity grade is therefore the single most decision-relevant skill in managing acne, and it is the foundation for the management SDL that follows.
RECALL
Before we begin, recall from your earlier Physiology and Anatomy learning the structure of the pilosebaceous unit — the hair follicle together with its attached sebaceous gland, densely distributed over the face, chest, and back. Recall that sebaceous glands are holocrine glands whose secretion (sebum) is driven by androgens (testosterone converted to the more potent dihydrotestosterone by 5α-reductase within the sebocyte). Recall too the basic inflammatory cascade — how chemotactic signals recruit neutrophils to produce a pustule, and how deeper dermal inflammation produces a nodule. These prior concepts are exactly the machinery that goes wrong in acne, so keeping them in mind will make the pathogenesis section feel like revision rather than new material.
What Acne Looks Like: Primary Lesion Types
Primary Acne Lesion Types
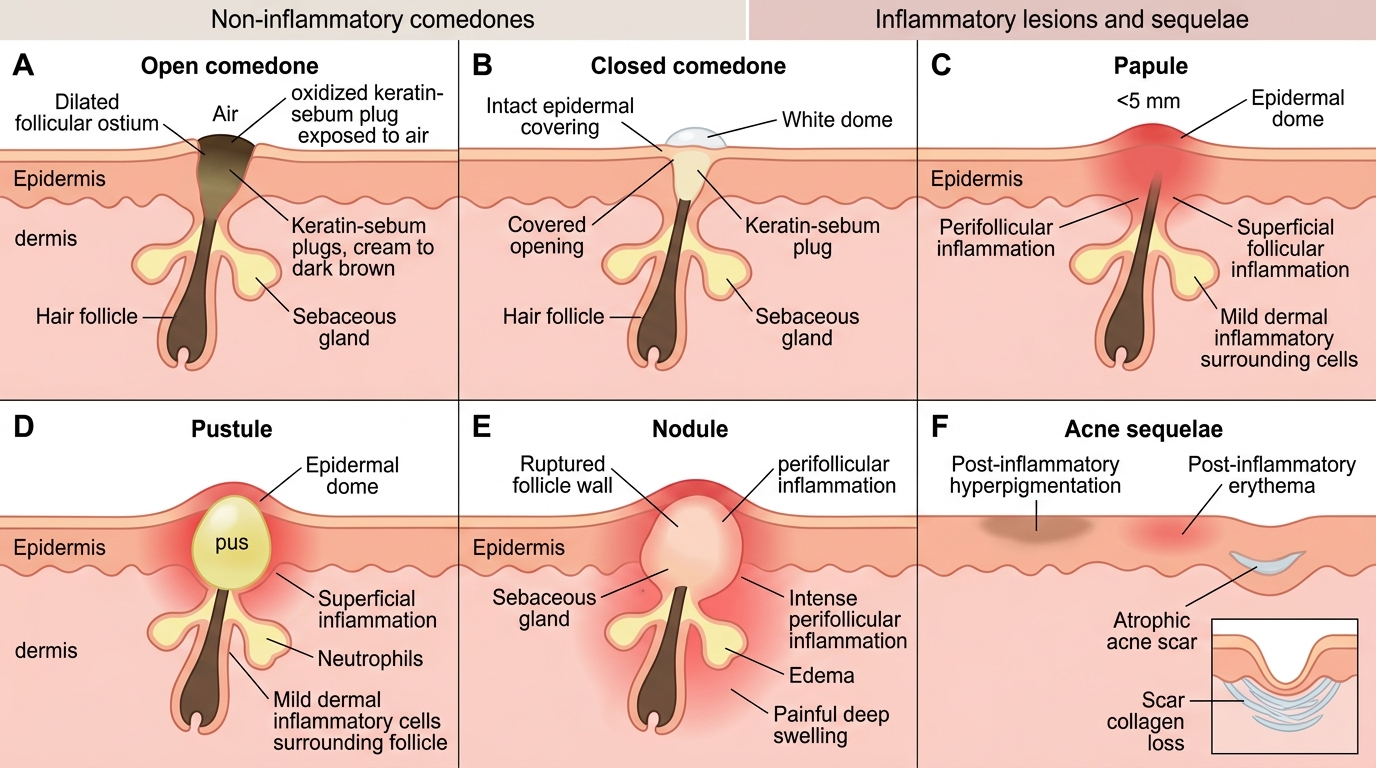
The whole of acne recognition rests on confidently naming the lesions you see, because the mix of lesion types is what defines both the diagnosis and the grade. Acne lesions fall into two broad families that you must be able to tell apart at a glance: non-inflammatory comedones and inflammatory lesions. A comedone is the primary, defining lesion of acne — a plugged pilosebaceous follicle filled with keratin and sebum — and it comes in two forms. An open comedone, the everyday 'blackhead,' is a dilated follicular opening whose plug is exposed to air; the black colour is oxidised keratin and melanin, not dirt, a point worth telling patients who scrub their skin raw. A closed comedone, or 'whitehead,' has a narrow covered opening so the plug is not oxidised and appears as a small skin-coloured or pale bump. When the follicle wall ruptures and inflammation follows, you get the inflammatory lesions, in increasing order of depth and severity.
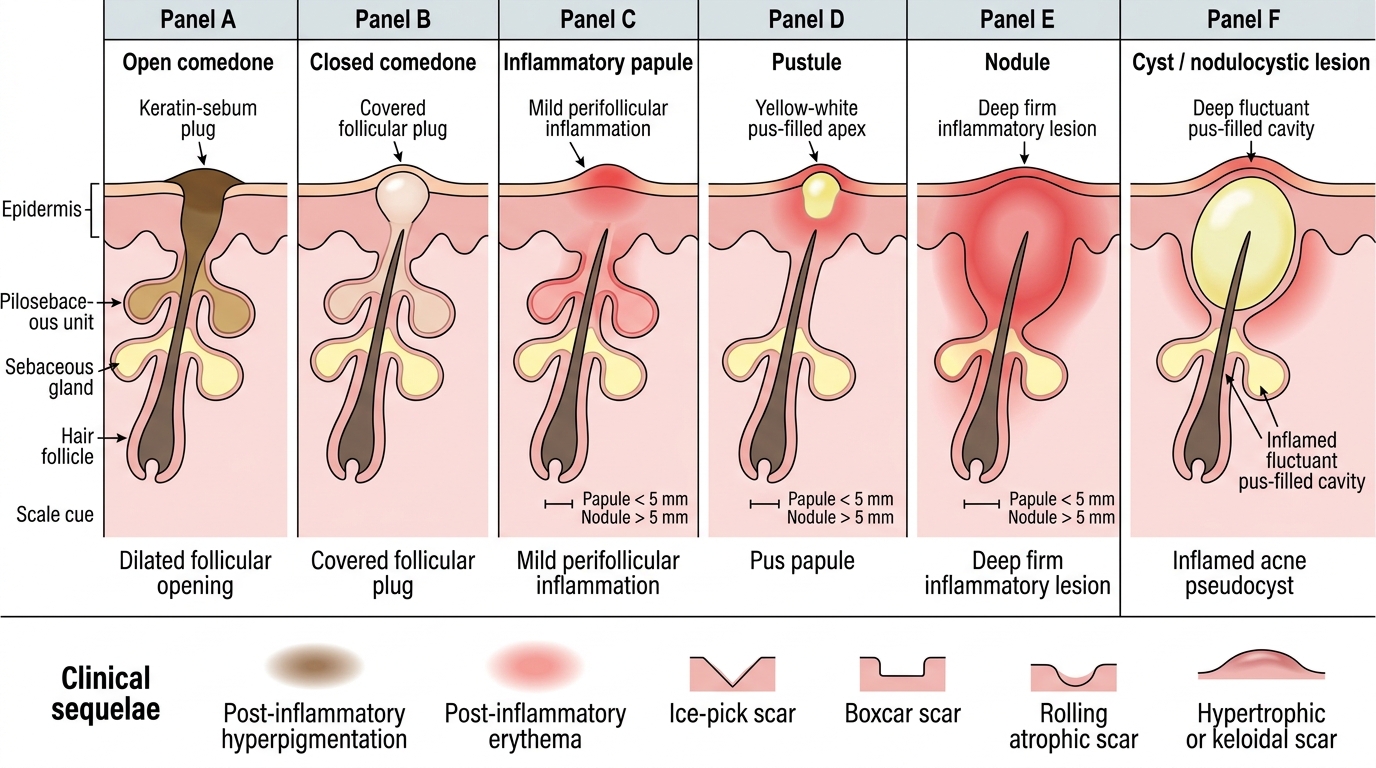
Acne Lesion Types and Sequelae
The inflammatory lesions form a graded series:
- Papule — a small (<5 mm) solid red raised lesion, tender, with no visible pus.
- Pustule — a papule whose apex contains visible yellow-white pus.
- Nodule — a larger (>5 mm), deep, firm, often very tender inflammatory lesion extending into the dermis; nodular acne is the type that scars.
- Cyst / nodulocystic lesion — a deep, fluctuant, pus-filled cavity; in acne these are usually inflamed pseudocysts rather than true epithelial-lined cysts.
Alongside the active lesions, always note the sequelae: post-inflammatory hyperpigmentation (the dark marks that distress patients with skin of colour), post-inflammatory erythema, and true scarring (ice-pick, boxcar, rolling atrophic scars, or hypertrophic/keloidal scars). Recognising scarring is itself a marker of severity and urgency.
The Four Pillars of Acne Pathogenesis
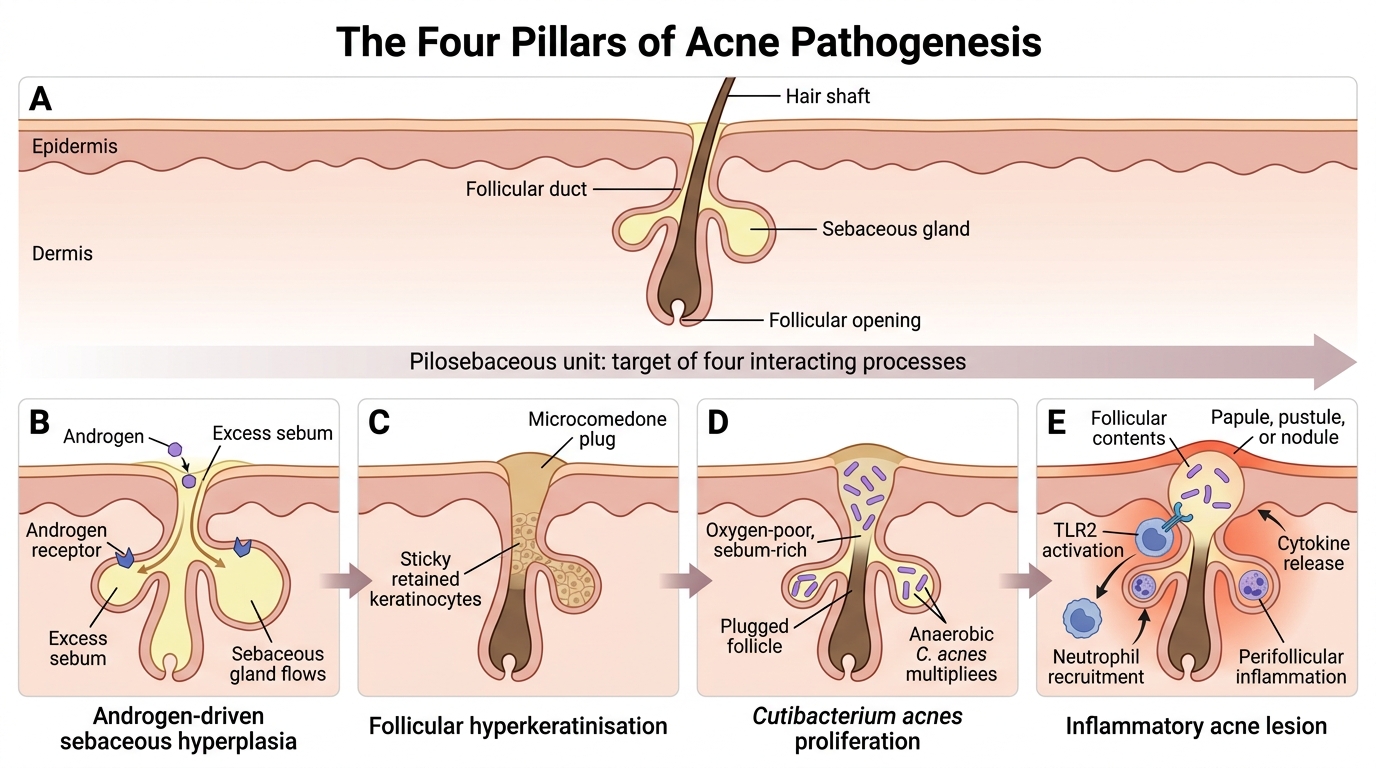
Four Pillars of Acne Pathogenesis
Acne is not caused by a single factor but by four interacting processes acting together on the pilosebaceous unit, and understanding them explains both why the lesions look as they do and why each treatment works. The four pillars are best learnt as a causal chain. First, under the influence of androgens, the sebaceous gland enlarges and produces excess sebum — this is why acne begins at puberty and why oily skin accompanies it. Second, the lining of the follicular duct undergoes follicular hyperkeratinisation: keratinocytes become abnormally sticky and fail to shed, so they pile up and plug the follicular opening, creating the microcomedone that is the silent precursor of every acne lesion. Third, the warm, sebum-rich, oxygen-poor plugged follicle is an ideal home for Cutibacterium acnes (the anaerobic diphtheroid formerly named Propionibacterium acnes), which proliferates and metabolises sebum. Fourth, C. acnes and the trapped contents trigger inflammation — the organism activates Toll-like receptor 2 on immune cells, releasing inflammatory cytokines that recruit neutrophils and convert a quiet comedone into a papule, pustule, or nodule.
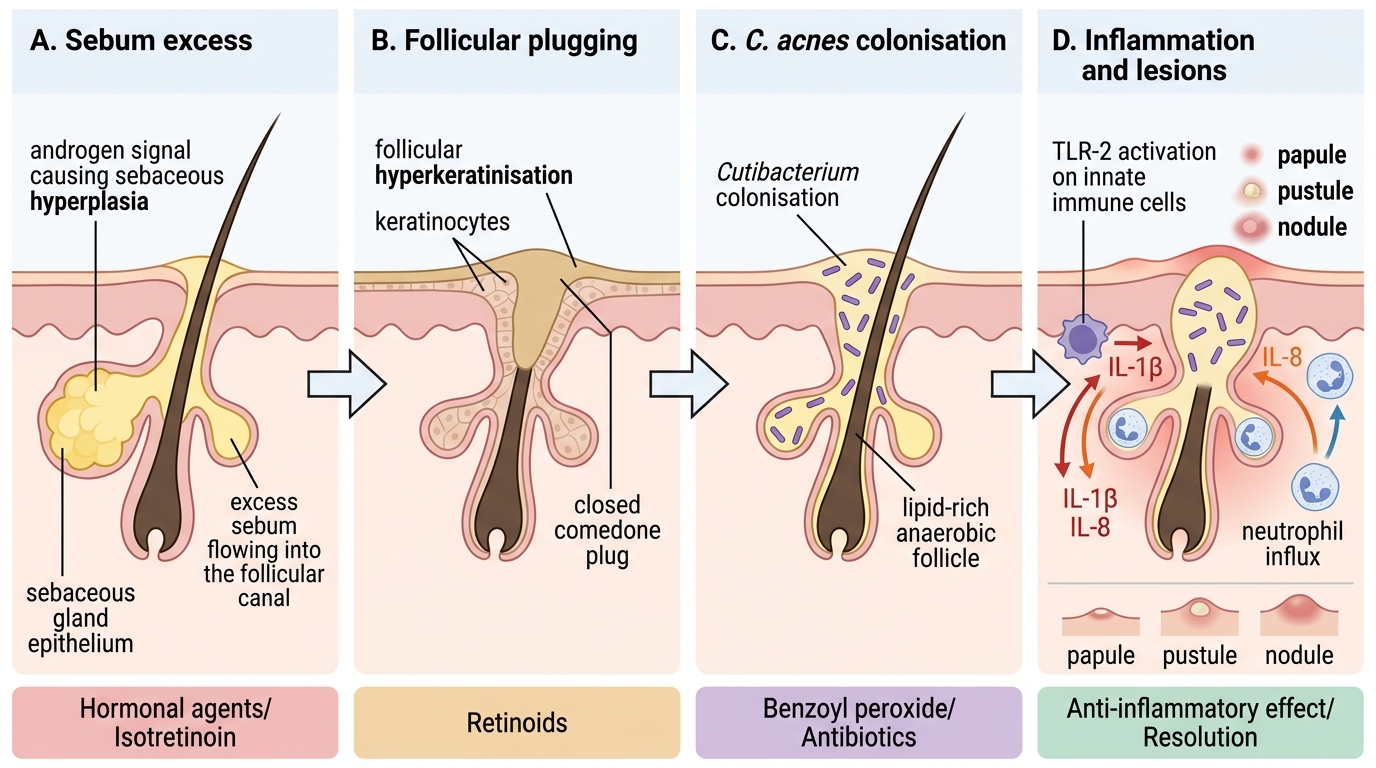
Four-Step Pathogenesis of Acne
The practical value of this framework is that every effective acne treatment targets one or more of these four pillars:
- Retinoids correct follicular hyperkeratinisation (and so prevent comedones at the source).
- Hormonal agents and isotretinoin reduce sebum production.
- Benzoyl peroxide and antibiotics suppress C. acnes.
- Several agents (and the resolution of the above) reduce inflammation.
Keeping the four pillars in mind turns acne treatment from a list to be memorised into a logical, mechanism-based plan.
SELF-CHECK
A patient has numerous skin-coloured, dome-shaped 1–2 mm papules with no surrounding redness and a barely visible central opening over the forehead. Which lesion type are these, and which pathogenetic step do they primarily represent?
A. Pustules — representing Cutibacterium acnes infection
B. Closed comedones (whiteheads) — representing follicular hyperkeratinisation with plugging
C. Nodules — representing deep dermal inflammation
D. Open comedones (blackheads) — representing oxidised keratin exposed to air
Reveal Answer
Answer: B. Closed comedones (whiteheads) — representing follicular hyperkeratinisation with plugging
Skin-coloured, non-inflamed papules with a covered (barely visible) opening are closed comedones, or whiteheads. Because the follicular opening is narrow and covered, the keratin–sebum plug is not exposed to air and does not oxidise, so the lesion stays pale rather than turning black. Comedones are the primary, defining lesions of acne and they represent the follicular hyperkeratinisation pillar — abnormally cohesive keratinocytes plug the follicular duct. They are non-inflammatory: there is no redness, pus, or tenderness, which distinguishes them from papules and pustules.
Risk Factors, Triggers, and Who Gets Acne
Risk Factors and Triggers for Acne
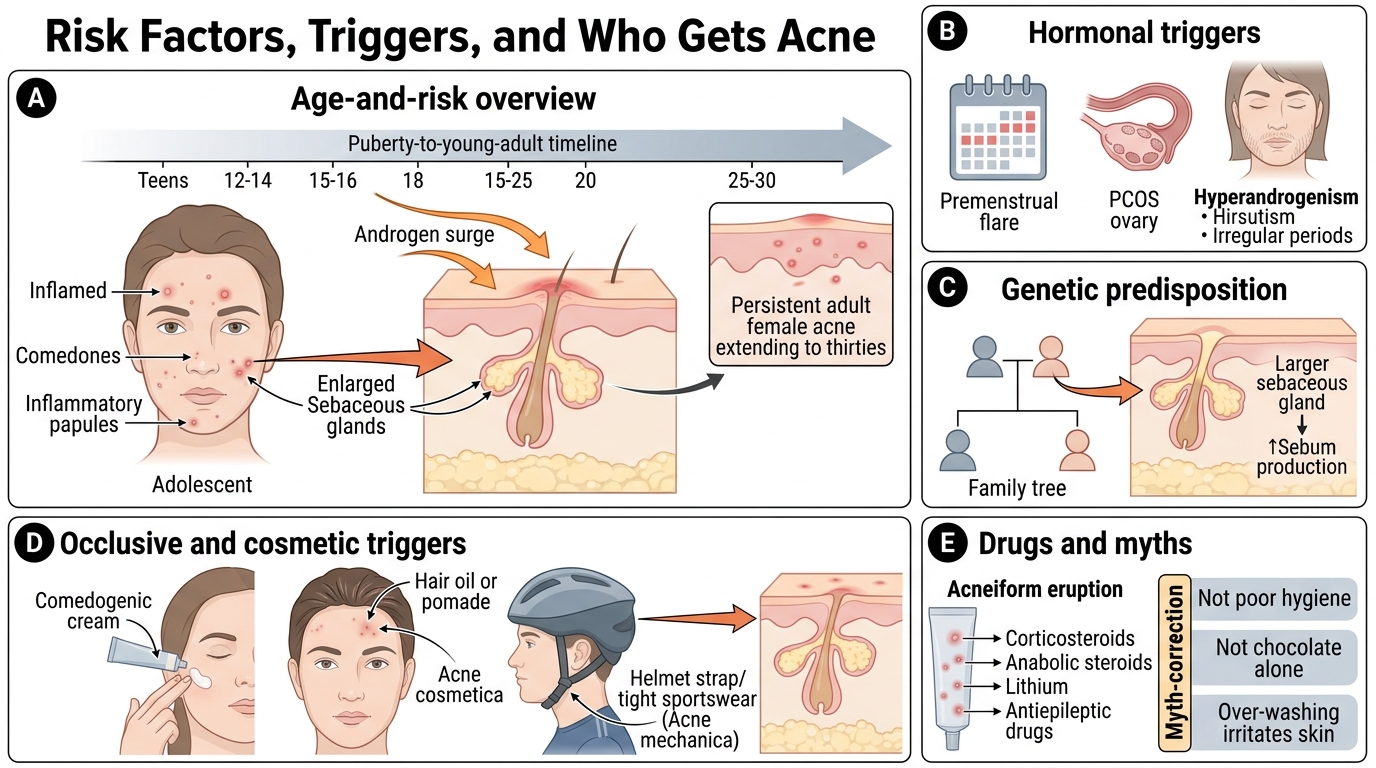
Recognising acne is easier and more accurate when you know who tends to get it and what makes it worse, because the risk-factor profile is part of the clinical picture you build at the bedside. Acne is overwhelmingly a disease of adolescence and young adulthood, beginning as the androgen surge of puberty drives sebaceous activity; it usually peaks in the mid-to-late teens and resolves by the mid-twenties, though a substantial minority — especially women — have persistent or late-onset acne into their thirties. A strong family history is common, reflecting genetic influence on sebaceous gland size and activity. Beyond age and genetics, several host and external factors modulate severity, and asking about them sharpens both recognition and patient counselling. It is equally important to know what does NOT cause acne, so you can correct the guilt and myths patients carry — acne is not caused by poor hygiene or by chocolate alone, and over-washing actually irritates the skin.
The clinically useful risk factors and triggers are:
- Hormonal: puberty, the premenstrual flare, polycystic ovary syndrome (PCOS) and other hyperandrogenic states — suspect these in a woman with acne plus irregular periods, hirsutism, or sudden severe acne.
- Cosmetic / occlusive (acne cosmetica): comedogenic creams, hair oils applied to the forehead (pomade acne), and occlusive sportswear or helmets (acne mechanica).
- Drugs (acneiform eruptions): corticosteroids, anabolic steroids, androgens, lithium, isoniazid, phenytoin, and some others — these produce a monomorphic papular eruption rather than true polymorphic acne.
- Dietary association: high-glycaemic-index diets and possibly skimmed milk show a modest association in studies; chocolate alone is not proven causal.
A red flag worth memorising: sudden-onset severe acne, acne with virilising features, or acne unresponsive to standard treatment in a woman should prompt evaluation for an underlying endocrine cause.