Page 2 of 11
DR5.1 | Scabies Treatment Planning — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Scabies: Differential Diagnosis and Confirmatory Investigations
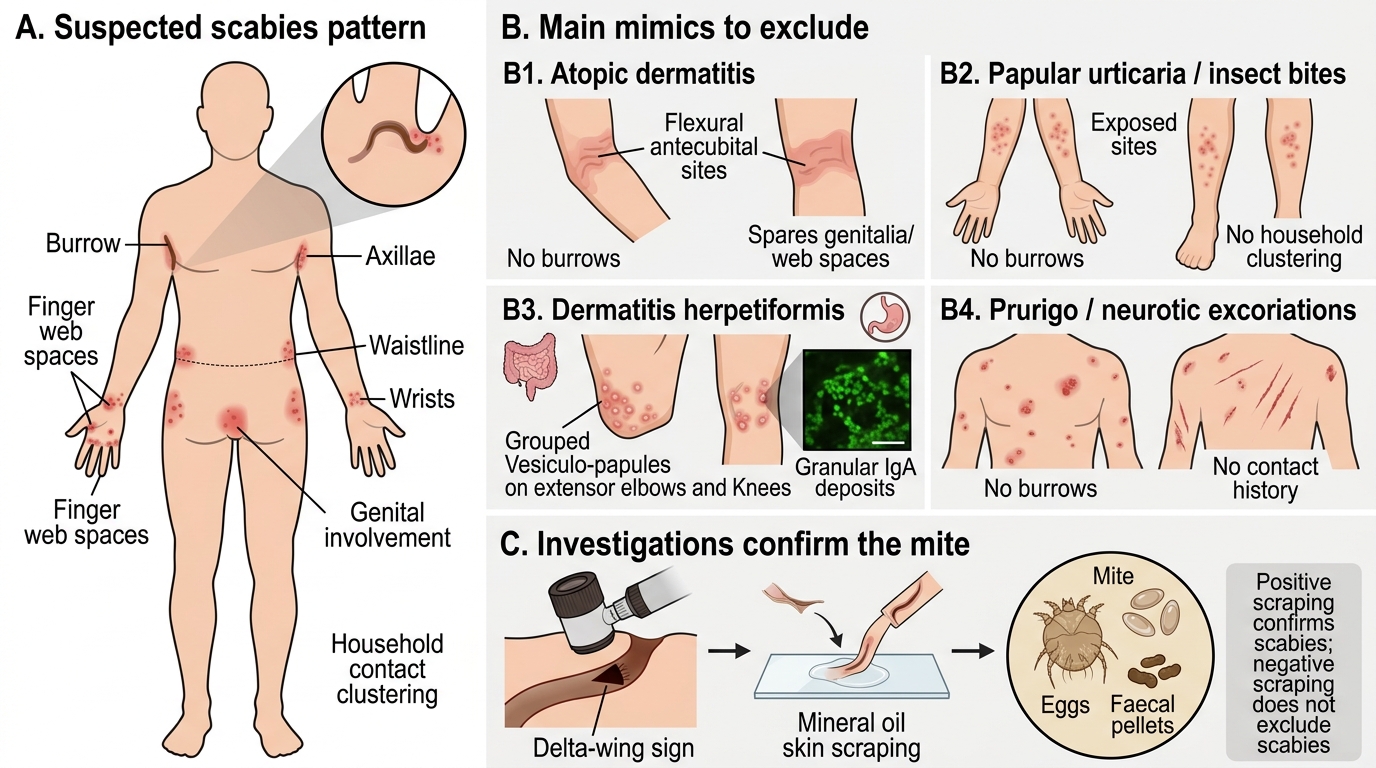
Because scabies is dominated by itch and excoriation, it is mimicked by several common dermatoses, and devising the right treatment plan first requires excluding these. Atopic dermatitis shares the intense pruritus but favours flexural sites (antecubital and popliteal fossae), spares the genitalia and web spaces, and lacks burrows and contact clustering. Papular urticaria and insect bites produce grouped itchy papules on exposed sites but again lack burrows and household spread. Dermatitis herpetiformis is intensely itchy and grouped over extensor surfaces but is associated with coeliac disease and shows IgA deposits on immunofluorescence. Prurigo and neurotic excoriations lack burrows and a contact history. The decisive investigations are therefore aimed at demonstrating the mite: dermoscopy of a suspected burrow, and microscopy of a skin scraping in mineral oil looking for the mite, eggs or faecal pellets. A positive scraping confirms the diagnosis, but a negative scraping does not exclude it because the mite burden is low — so treatment is often started on clinical grounds.
- Atopic dermatitis: flexural, no burrows, spares genitalia/web spaces
- Papular urticaria / insect bites: exposed sites, no burrows, no clustering
- Dermatitis herpetiformis: extensor, coeliac link, IgA on immunofluorescence
- Prurigo / neurotic excoriations: no burrows, no contact history
- Investigations: dermoscopy (delta-wing sign); skin scraping microscopy (mite/eggs/scybala) — negative result does NOT exclude scabies
Treatment Plan for Scabies: Scabicides, ADRs, and Contact Management
Provided image
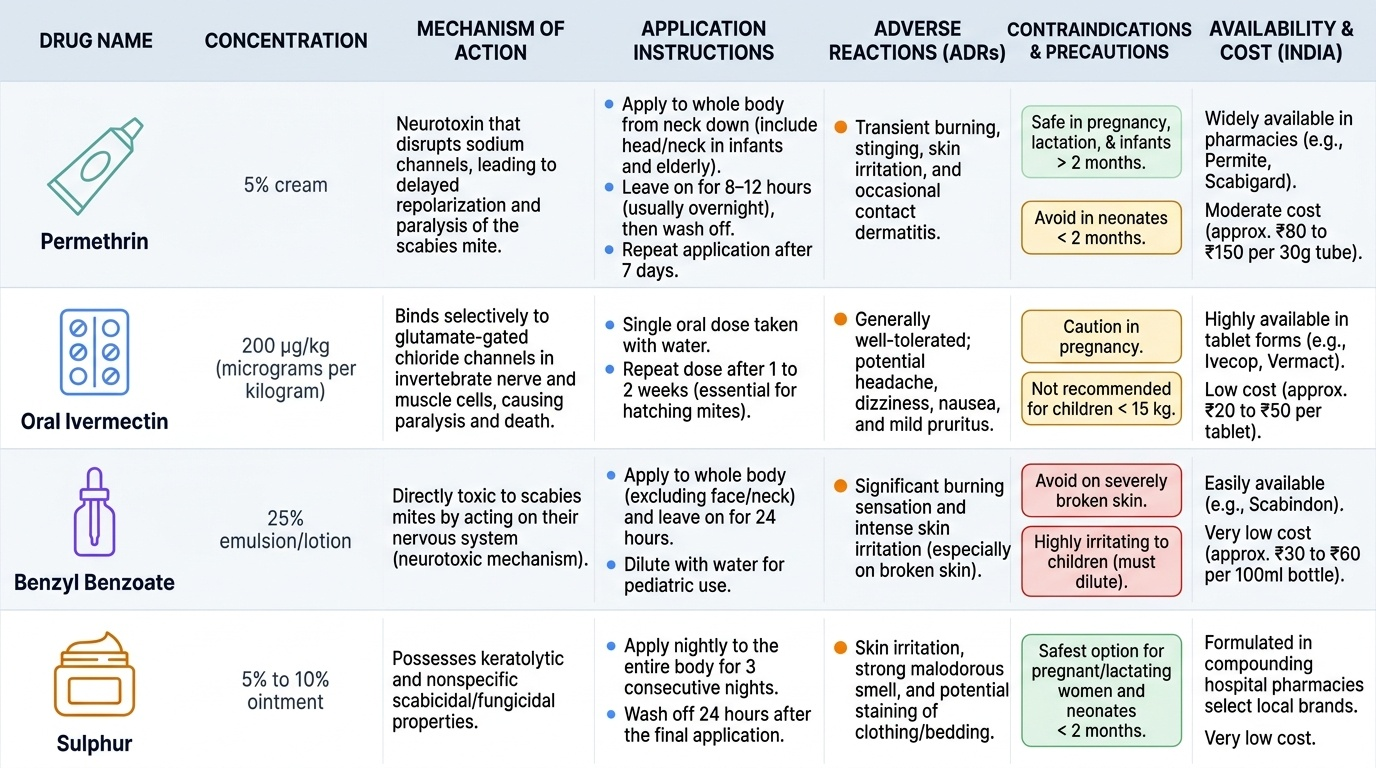
Devising the treatment plan is the core of this competency, and a good plan has four parts: the right scabicide applied correctly, simultaneous treatment of all close contacts, environmental decontamination, and counselling about post-scabetic itch. The first-line scabicide for ordinary scabies is permethrin 5% cream, applied to the whole body from the neck downwards (including the head and neck in infants and the elderly), left on for 8 to 12 hours (usually overnight) and washed off, then repeated after 7 days to kill mites that hatch from surviving eggs; it is safe in pregnancy, lactation and infants over two months and is the preferred topical agent. The principal alternative is oral ivermectin at 200 micrograms per kilogram as a single dose repeated after 1 to 2 weeks — invaluable for outbreaks, institutional control, patients who cannot apply creams reliably, and crusted scabies. Older topical agents include benzyl benzoate 25% (effective but irritant, diluted for children) and sulphur 5-10% ointment (messy and malodorous but the safest option in neonates and pregnancy). Crucially, all close and household contacts must be treated on the same day even if asymptomatic, and bedding, towels and clothing used in the preceding 3-4 days should be machine-washed hot and dried or sealed in a plastic bag for 72 hours. Patients must be warned that itch can persist for 2-4 weeks after successful treatment (post-scabetic itch), managed with emollients, antihistamines and a short course of topical steroid — and that this is NOT treatment failure. Crusted scabies needs combined repeated oral ivermectin plus topical permethrin and a keratolytic, with isolation. The adverse drug reactions the competency demands you state are: permethrin — transient burning, stinging and irritation, occasional contact dermatitis; ivermectin — generally well tolerated but may cause headache, dizziness, nausea and pruritus, with caution in pregnancy and in children weighing under 15 kg where safety is not established; benzyl benzoate — significant burning and irritation, especially on broken skin and in children; sulphur — irritation, staining and odour.
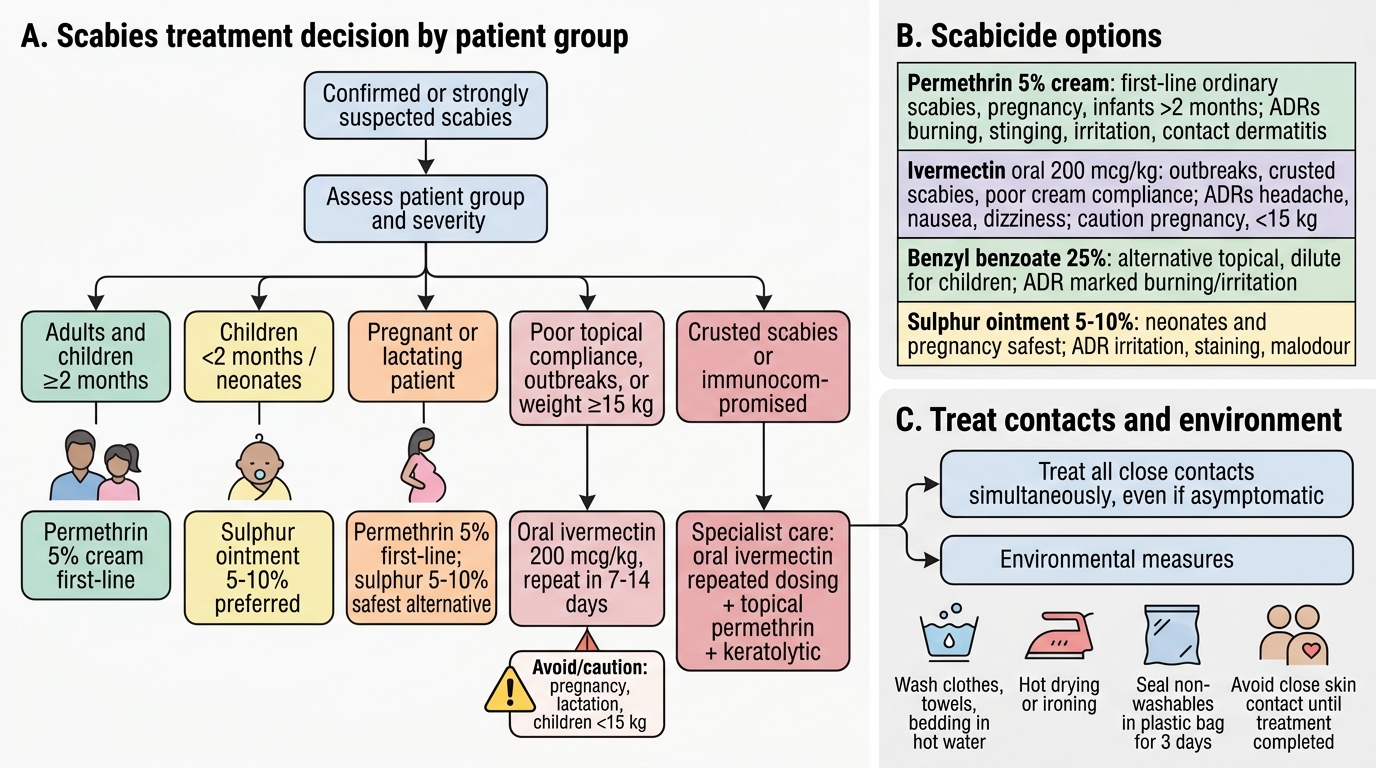
Scabies Treatment Decision Flowchart
| Scabicide | Strength | First-line for | Key ADRs / cautions |
|---|---|---|---|
| Permethrin cream | 5% | Ordinary scabies (incl. pregnancy, infants >2 mo) | Burning, stinging, irritation, contact dermatitis |
| Ivermectin (oral) | 200 mcg/kg, repeat 1-2 wk | Outbreaks, crusted scabies, poor cream compliance | Headache, nausea, dizziness; caution in pregnancy, <15 kg |
| Benzyl benzoate | 25% (dilute for children) | Alternative topical | Marked burning/irritation, esp. broken skin/children |
| Sulphur ointment | 5-10% | Neonates, pregnancy (safest) | Irritation, staining, malodour |
SELF-CHECK
A 28-year-old woman in her first trimester of pregnancy presents with classic scabies; her husband has similar itching. Which treatment plan is most appropriate?
A. Oral ivermectin 200 mcg/kg single dose for her only
B. Permethrin 5% cream for her, applied overnight and repeated after 7 days, AND simultaneous treatment of her husband, with bedding/clothing decontamination
C. Lindane 1% lotion for the whole household
D. A potent topical corticosteroid until the itch settles
Reveal Answer
Answer: B. Permethrin 5% cream for her, applied overnight and repeated after 7 days, AND simultaneous treatment of her husband, with bedding/clothing decontamination
Permethrin 5% is the first-line scabicide and is safe in pregnancy and lactation; ivermectin is best avoided in pregnancy. Treating the index patient alone would fail — all close contacts (here the husband) must be treated on the same day, with environmental decontamination. Steroids treat itch, not the mite, and lindane is avoided due to neurotoxicity.
Self-Assessment: Scabies Treatment Scenarios
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Scabies Treatment Scenarios: Applying the Four Pillars
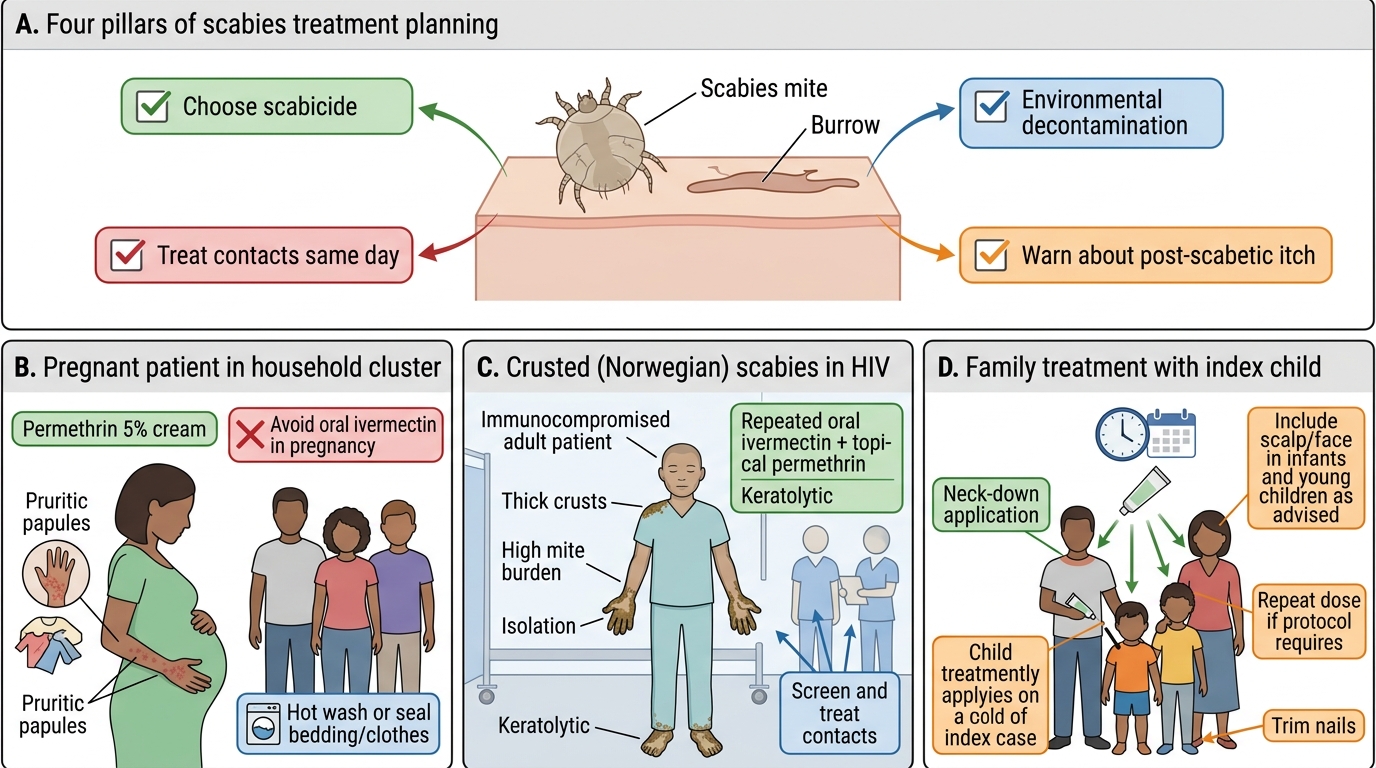
Use these scenarios to test whether you can convert the principles above into a concrete, defensible treatment plan for the patient in front of you, choosing the scabicide, planning contact treatment, and stating the adverse effects you would warn about. Work through each before reading any model answer, and for every case ask yourself the same four questions: which scabicide and why, which contacts must be treated, what environmental measures apply, and what will I tell the patient to expect afterwards. These mirror the four pillars of the treatment plan and are exactly what an examiner expects you to articulate. Pay particular attention to the patient-group modifiers — pregnancy, very young children, immunocompromise — because these are where the wrong default choice causes harm or treatment failure.
- Scenario 1 — A pregnant woman in a household cluster: choose permethrin 5% (avoid ivermectin), treat all contacts the same day, decontaminate bedding, warn of post-scabetic itch.
- Scenario 2 — An HIV-positive man with thick hyperkeratotic crusts and little itch: recognise crusted (Norwegian) scabies, isolate, give combined repeated oral ivermectin + topical permethrin + keratolytic, screen/treat all ward contacts and staff.
- Scenario 3 — A family of four with an index child: treat all four simultaneously, give clear neck-down application instructions (head-and-neck in the youngest), repeat at 7 days, decontaminate the shared bedroom's linen.
CLINICAL PEARL
The two most common reasons scabies 'fails' to clear are entirely avoidable: not treating asymptomatic contacts, and the patient (or a junior doctor) mistaking normal post-scabetic itch — which can last 2-4 weeks after the mite is dead — for treatment failure and escalating to ever-stronger steroids. Always write the plan as a household prescription, not an individual one, and counsel up front that the itch outlasts the mite. If a genuinely treated patient is still infested at review, suspect re-infestation from an untreated contact or undiagnosed crusted scabies in the household.