Page 4 of 11
DR11.2 | Dermatologic Reactions to ART Drugs — SDL Guide
Learning Objectives
- Recognise the spectrum of cutaneous reactions caused by common antiretroviral (ART) drugs, from mild rash to life-threatening Stevens-Johnson syndrome / toxic epidermal necrolysis
- Attribute characteristic reactions to specific drugs — nevirapine, abacavir, zidovudine, and efavirenz — and explain their underlying mechanisms
- Distinguish benign drug rash from severe cutaneous adverse reactions (SJS/TEN, DRESS) and from immune reconstitution inflammatory syndrome (IRIS) using clinical features and body-surface-area cut-offs
- Initiate appropriate primary management, including the decision to continue, stop permanently, or substitute the offending drug, and recognise when to refer
INSTRUCTIONS
Antiretroviral drugs are lifesaving, but several of them are also among the more frequent and occasionally dangerous causes of cutaneous adverse drug reactions a clinician will encounter. The skin is often the first organ to signal that an ART regimen is not being tolerated, and the range of reactions runs from a trivial self-limiting rash to Stevens-Johnson syndrome and toxic epidermal necrolysis, which carry significant mortality. For the intern and the physician managing people living with HIV, the critical skill is to recognise the reaction early, judge its severity, and make the correct decision — to reassure and continue, or to stop the drug and never rechallenge. This SDL builds that skill drug by drug, anchored in the body-surface-area thresholds and management principles you must carry to the bedside.
References
- Sacchidanand S, et al. (eds). IADVL Textbook of Dermatology, 4th ed. Ch: Cutaneous Adverse Drug Reactions (textbook)
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Drug Reactions (textbook)
- National AIDS Control Organisation (NACO). National Guidelines for HIV Care and Treatment / Antiretroviral Therapy Guidelines. Ministry of Health and Family Welfare, Government of India (policy)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 29-year-old woman started a nevirapine-based antiretroviral regimen ten days ago. She returns to the ART centre with fever, a spreading red rash over her face and trunk, and now painful erosions inside her mouth and on her lips. As you examine her you notice the rash is becoming dusky in places, and gentle lateral pressure on the skin makes the epidermis shear away. This is no longer a simple drug rash: she is developing a severe cutaneous adverse reaction on the Stevens-Johnson syndrome / toxic epidermal necrolysis spectrum, and the drug that is saving her from HIV is now threatening her life. The decisions made in the next hour — to stop the nevirapine immediately and never rechallenge it, to assess the body surface area involved, and to arrange urgent supportive care — will determine her outcome. The same drugs that suppress HIV can, in a minority of patients, produce some of the most feared reactions in all of medicine.
WHY THIS MATTERS
Recognising and managing the cutaneous reactions to antiretroviral drugs is a core competency for any clinician caring for people living with HIV, and in India that increasingly includes physicians, dermatologists, and interns at ART centres and general hospitals. A cutaneous drug reaction is one of the commonest reasons a patient stops or is switched off an ART regimen, and getting the decision right matters enormously: stopping a drug unnecessarily for a trivial rash interrupts viral suppression and breeds resistance, whereas continuing a drug through the early signs of Stevens-Johnson syndrome or a hypersensitivity reaction can be fatal. This is precisely competency DR11.2 — to recognise the common dermatological manifestations of ART drugs and to initiate primary management appropriately. The skill is not memorising every reaction but learning to grade severity quickly and to act decisively: reassure and continue, or stop and never rechallenge.
RECALL
Recall from your Pharmacology teaching the broad classes of antiretroviral drugs, because the reactions track the class. The non-nucleoside reverse transcriptase inhibitors (NNRTIs) — nevirapine and efavirenz — are the most important cutaneous offenders, with nevirapine notorious for rash and hypersensitivity and efavirenz causing a milder eruption. The nucleoside reverse transcriptase inhibitors (NRTIs) include abacavir, whose hypersensitivity reaction is pharmacogenetically determined, and zidovudine, which causes hyperpigmentation rather than an allergic rash. Recall also the general framework of cutaneous adverse drug reactions you have already met: the benign maculopapular (morbilliform) rash at one end, and the severe cutaneous adverse reactions — Stevens-Johnson syndrome, toxic epidermal necrolysis, and DRESS (drug reaction with eosinophilia and systemic symptoms) — at the other. Finally, recall the principle of pharmacogenomics: a specific HLA allele can predict the risk of a severe drug reaction, a concept that is central to the safe use of abacavir.
ART Drugs and the Skin: Clinical Presentation Spectrum
ART-Related Skin Reactions: Clinical Severity Spectrum
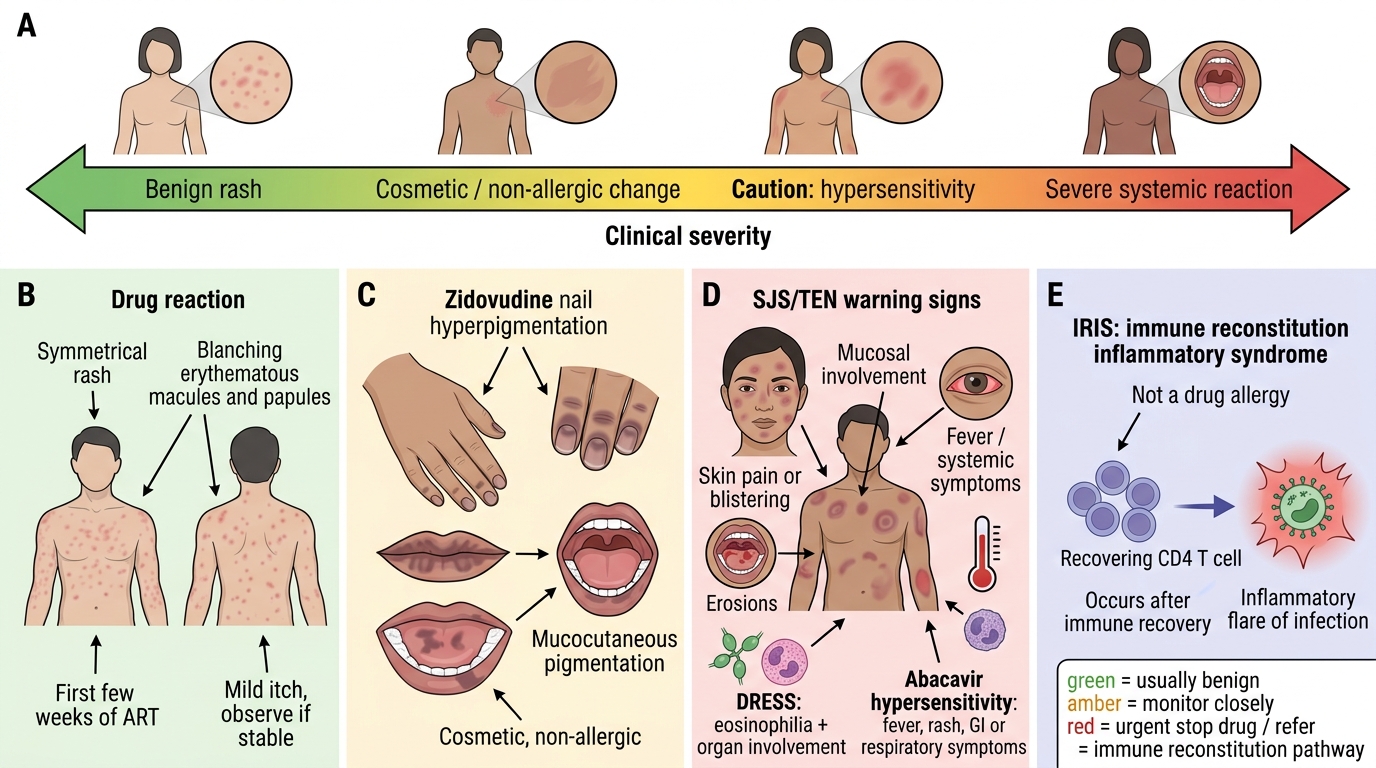
Cutaneous reactions to antiretroviral drugs occupy a wide spectrum of severity, and the clinician's first task is to place any given presentation along that spectrum. At the benign end lies the morbilliform (maculopapular) rash — a symmetrical, blanching, measles-like eruption that appears in the first few weeks of therapy, is often mildly itchy, and frequently settles even if the drug is continued under observation. In the middle lie reactions that demand caution: zidovudine-induced hyperpigmentation, which is cosmetically distressing but not dangerous, and the early phases of hypersensitivity reactions. At the severe end lie the reactions that can kill — Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN), abacavir hypersensitivity, and DRESS (drug reaction with eosinophilia and systemic symptoms). Separate from all of these is immune reconstitution inflammatory syndrome (IRIS), which is not a drug allergy at all but an inflammatory flare driven by the recovering immune system. Learning to scan a patient on ART for the warning features that separate a benign rash from a severe reaction is the organising skill of this module.
The spectrum, from milder to most severe:
- Benign: morbilliform (maculopapular) rash, efavirenz rash
- Cosmetic / non-allergic: zidovudine nail and mucocutaneous hyperpigmentation
- Severe / systemic: abacavir hypersensitivity, DRESS, Stevens-Johnson syndrome, toxic epidermal necrolysis
- Inflammatory (not allergic): IRIS-related cutaneous flares after starting ART
Mechanisms of ART-Induced Cutaneous Reactions
Mechanisms of ART-Induced Cutaneous Reactions
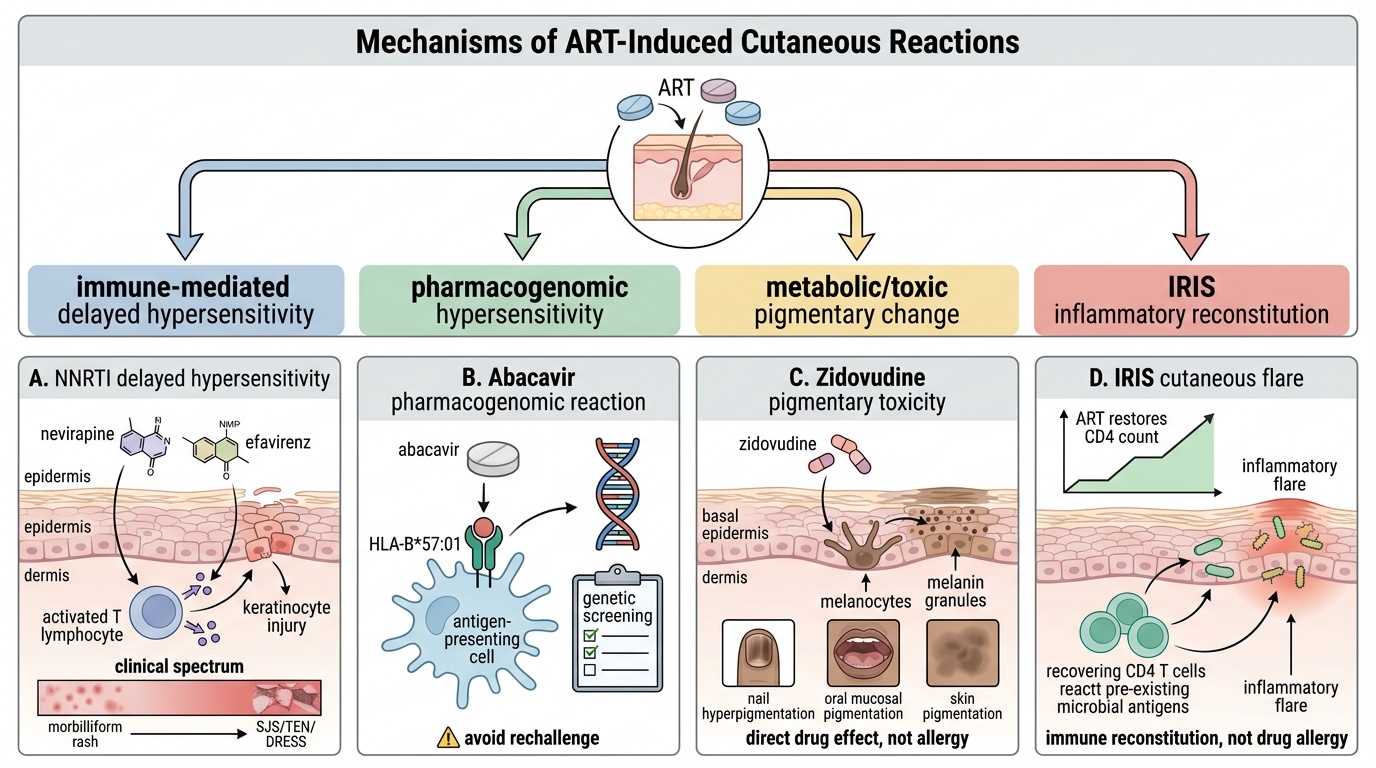
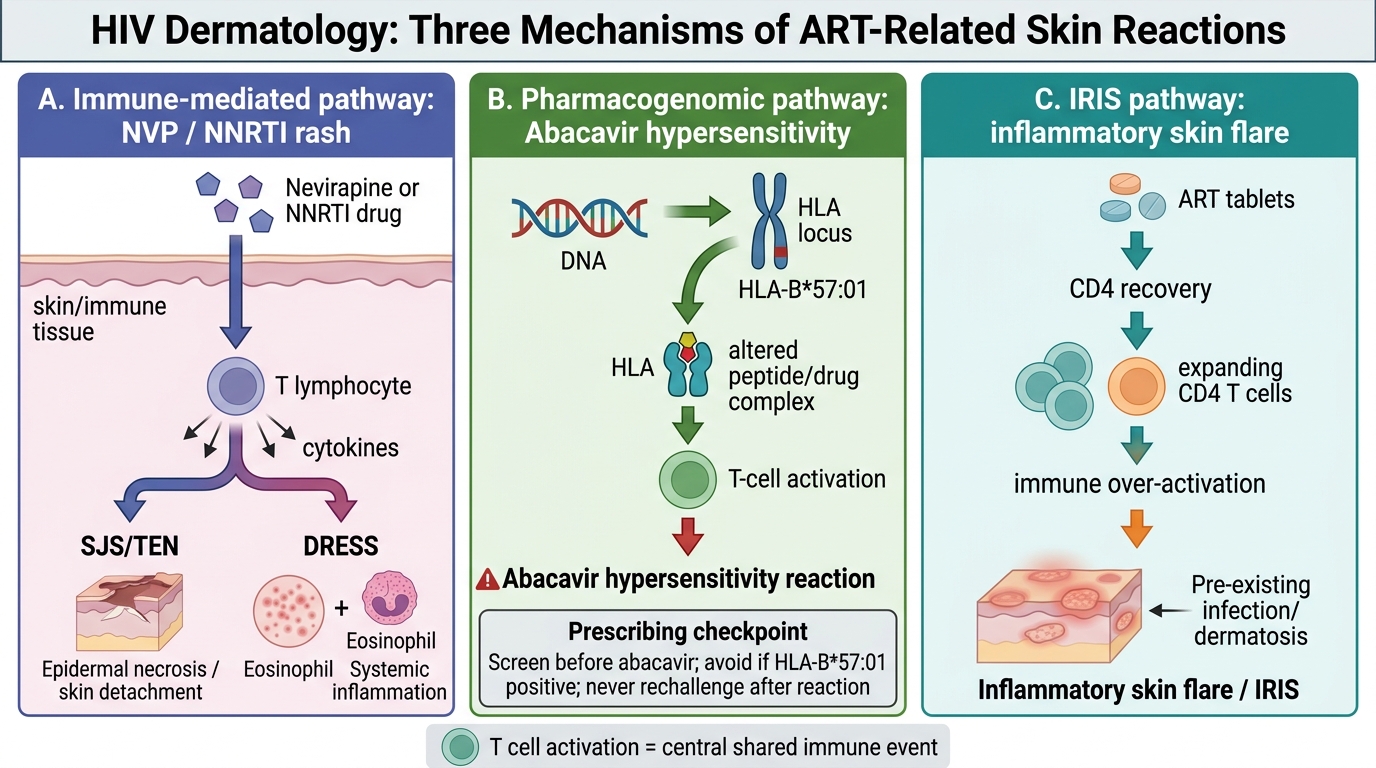
The cutaneous reactions to antiretroviral drugs arise through several distinct mechanisms, and understanding them clarifies why some reactions can be watched while others demand immediate, permanent drug withdrawal. Immune-mediated (delayed hypersensitivity) reactions account for the NNRTI-associated rashes: nevirapine and, more mildly, efavirenz provoke a T-cell-driven response that ranges from a benign morbilliform rash to Stevens-Johnson syndrome, toxic epidermal necrolysis, and DRESS. A second mechanism is pharmacogenomic: abacavir hypersensitivity occurs almost exclusively in patients carrying the HLA-B*57:01 allele, which is why genetic screening before starting abacavir can virtually eliminate the reaction. A third, quite different mechanism is metabolic / toxic pigmentary change: zidovudine stimulates melanocytes to produce hyperpigmentation of the nails, oral mucosa, and skin, which is a direct drug effect rather than an allergy. Finally, IRIS is an inflammatory reconstitution phenomenon — as ART restores CD4 counts, the recovering immune system reacts vigorously against existing antigens and infections, producing cutaneous flares that are immunological but not allergic. Sorting any reaction into the correct mechanistic bucket guides the management decision.
Mechanisms of ART-Related Cutaneous Reactions in HIV
SELF-CHECK
Abacavir hypersensitivity reaction is most strongly predicted by the presence of which factor, and what does this imply for prescribing?
A. A low CD4 count; therefore abacavir is avoided below CD4 200
B. The HLA-B*57:01 allele; therefore genetic screening before starting abacavir markedly reduces the reaction
C. Female sex; therefore abacavir is contraindicated in women
D. Concurrent nevirapine use; therefore the two are never combined
Reveal Answer
Answer: B. The HLA-B*57:01 allele; therefore genetic screening before starting abacavir markedly reduces the reaction
Abacavir hypersensitivity is pharmacogenomically linked to the HLA-B*57:01 allele. Screening patients for this allele before prescribing abacavir, and withholding the drug in carriers, virtually eliminates the immunologically confirmed hypersensitivity reaction. If hypersensitivity occurs, abacavir must be stopped permanently and never rechallenged.
Drug-Specific Cutaneous Manifestations
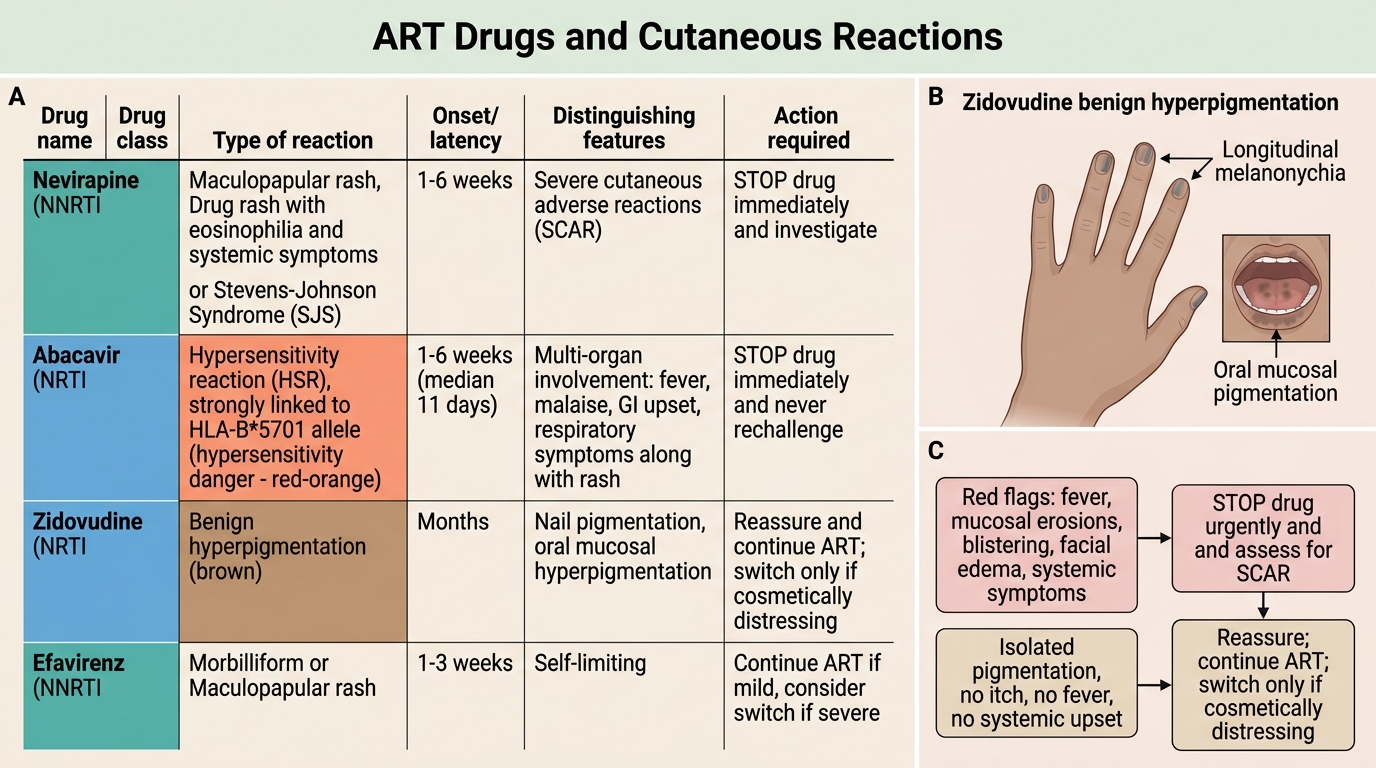
ART Drugs and Cutaneous Reactions
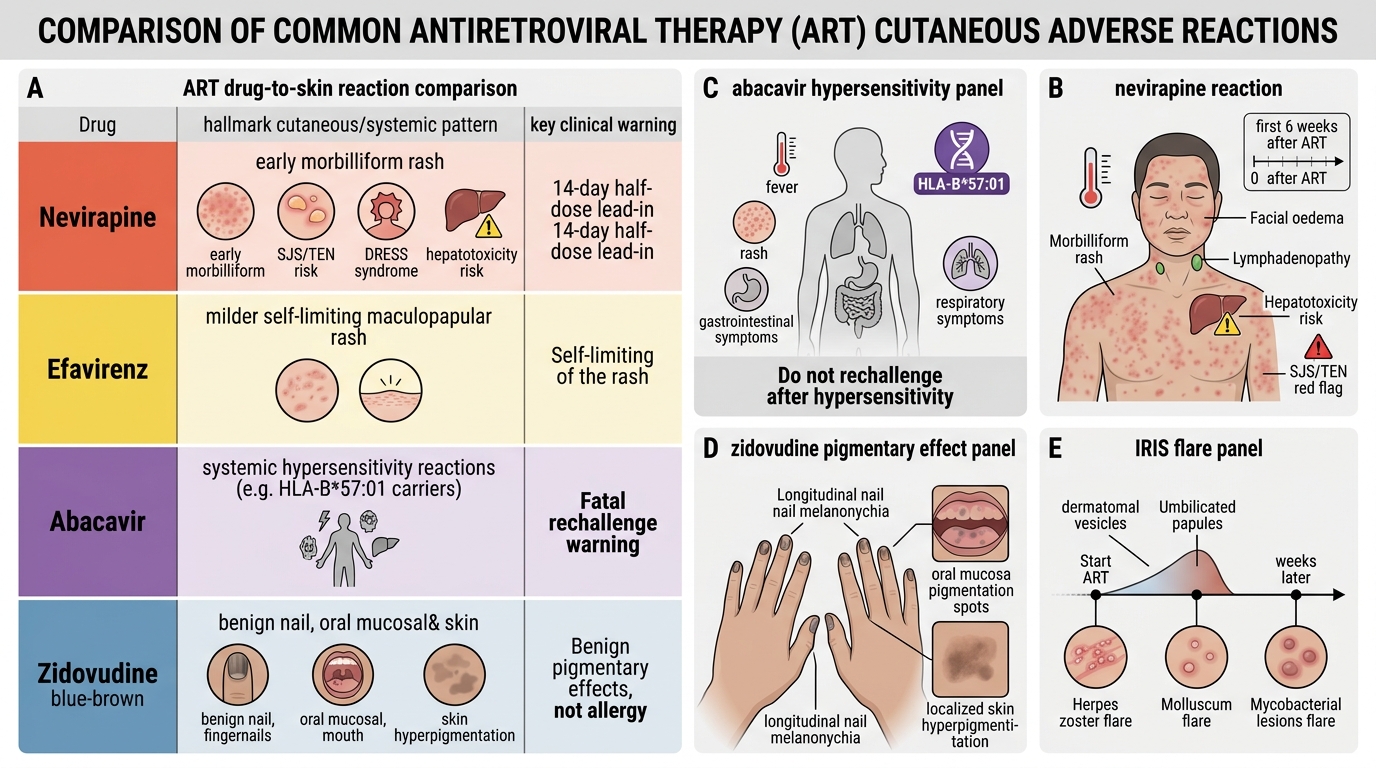
Each major antiretroviral offender produces a characteristic pattern, and recognising the drug-reaction pairing speeds diagnosis. Nevirapine is the most important: it commonly causes a morbilliform rash in the first six weeks, but it is also the ART drug most associated with progression to Stevens-Johnson syndrome and toxic epidermal necrolysis, with DRESS (rash with fever, facial oedema, lymphadenopathy, eosinophilia, and organ involvement), and with hepatotoxicity that may accompany the skin reaction. A 14-day half-dose lead-in is used to reduce the incidence of nevirapine rash. Efavirenz also causes a maculopapular rash, but it is typically milder and more often self-limiting. Abacavir produces a systemic hypersensitivity reaction — fever, rash, gastrointestinal and respiratory symptoms — in HLA-B*57:01 carriers, and rechallenge after a hypersensitivity reaction can be fatal. Zidovudine causes a distinctive blue-brown hyperpigmentation of the nails (longitudinal melanonychia), oral mucosa, and skin, which is a benign pigmentary effect rather than an allergy. Layered on these is IRIS, where pre-existing infections (herpes zoster, molluscum, mycobacterial lesions) flare within weeks of starting ART. Recognising which drug produces which pattern is the heart of competency DR11.2.
ART Drugs and Cutaneous Reactions
SELF-CHECK
A patient on ART develops blue-brown discolouration of the nails and oral mucosa, without itch, fever, or systemic upset. Which drug is the most likely cause, and how is it managed?
A. Nevirapine; stop immediately as this heralds SJS/TEN
B. Abacavir; stop permanently as this is hypersensitivity
C. Zidovudine; this is benign hyperpigmentation — reassure, and switch only if the patient is distressed
D. Efavirenz; this indicates DRESS and needs systemic steroids
Reveal Answer
Answer: C. Zidovudine; this is benign hyperpigmentation — reassure, and switch only if the patient is distressed
Zidovudine causes benign hyperpigmentation of the nails (longitudinal melanonychia), oral mucosa, and skin through a direct effect on melanocytes. It is not an allergic reaction and is not dangerous; the patient should be reassured, and the drug switched only if the cosmetic change is distressing.