Page 10 of 23
DR9.4 | Lepra Reaction Treatment — SDL Guide
Learning Objectives
- Recognise the clinical presentation of Type 1 (reversal) and Type 2 (erythema nodosum leprosum) lepra reactions
- Explain the distinct immunological mechanisms of Type 1 (T-cell-mediated) and Type 2 (immune-complex-mediated) reactions
- Distinguish Type 1 from Type 2 reactions clinically, including which part of the Ridley-Jopling spectrum each affects
- Effectively treat each reaction type with the correct drug regimen, recognise the thalidomide contraindication, and continue multidrug therapy throughout
INSTRUCTIONS
Lepra reactions are acute immunological episodes that interrupt the otherwise chronic course of leprosy, and they are the principal cause of the nerve damage and disability that follow the disease. They are medical emergencies because the nerve function lost during a reaction can be permanent if not treated promptly. This module teaches you to recognise the two distinct reaction types, to understand why they are immunologically different, to distinguish them at the bedside, and — most importantly — to treat each correctly. The two reactions are easy to confuse and have partly different treatments, so getting the type right and choosing the right drug is the high-stakes clinical skill this module builds. Throughout, one rule never changes: multidrug therapy is continued during a reaction, never stopped.
References
- Neena Khanna. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Leprosy — Lepra Reactions (textbook)
- IADVL Textbook of Dermatology, 4th ed. Section: Leprosy — Reactions and Their Management (textbook)
- National Leprosy Eradication Programme (NLEP) Guidelines on Management of Reactions; WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy 2018 (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Two patients with leprosy arrive at your clinic in the same week, both 'flaring', and the temptation is to treat them the same. The first is a man with borderline-tuberculoid disease whose existing skin patches have suddenly turned red, raised, and swollen, and whose ulnar nerve is now tender — he is two months into multidrug therapy and his hand is starting to weaken. The second is a woman with lepromatous disease who has erupted in crops of fresh, exquisitely tender red nodules all over her arms and legs, with fever, malaise, and red painful eyes. Treat the first with corticosteroids and you rescue his nerve; treat the second the same way and you have helped, but you may also need clofazimine or thalidomide to control her recurring nodules — and if she is a young woman, thalidomide is absolutely forbidden. Same disease, two completely different immunological storms, two partly different treatments. Telling them apart, fast, is the skill that saves nerves and prevents catastrophe.
WHY THIS MATTERS
Lepra reactions are where leprosy does its lasting damage, so recognising and treating them correctly is among the most consequential skills in leprosy care. The acute neuritis of a reaction can destroy nerve function within days, and the difference between a hand that recovers and a hand that claws permanently is often whether corticosteroids were started in time. You will need to distinguish the two reaction types because, although both can need corticosteroids, their mechanisms, the patients who get them, and the additional drugs they require differ — and one of those drugs, thalidomide, is an absolute teratogen that must never reach a woman who could become pregnant. Getting the reaction type and its treatment right, while never stopping multidrug therapy, directly determines whether your patient keeps the use of their hands, feet, and eyes.
RECALL
Before beginning, recall from Immunology the two hypersensitivity mechanisms that underlie the reactions. Type IV (delayed-type, cell-mediated) hypersensitivity is driven by sensitised T cells releasing cytokines that activate macrophages and produce granulomatous inflammation over days — this is the basis of the Type 1 reversal reaction. Type III (immune-complex) hypersensitivity results from antigen-antibody complexes depositing in tissues, activating complement and recruiting neutrophils — this is the basis of the Type 2 reaction (erythema nodosum leprosum). Recall also from the classification module that borderline patients (BT, BB, BL) sit in the immunologically unstable middle of the Ridley-Jopling spectrum, while lepromatous patients (BL, LL) carry a very high bacillary load — these positions on the spectrum predict which reaction a patient is liable to develop.
Recognising a Lepra Reaction — Clinical Presentation and Urgency
Recognising Lepra Reactions: Clinical Presentation and Urgency
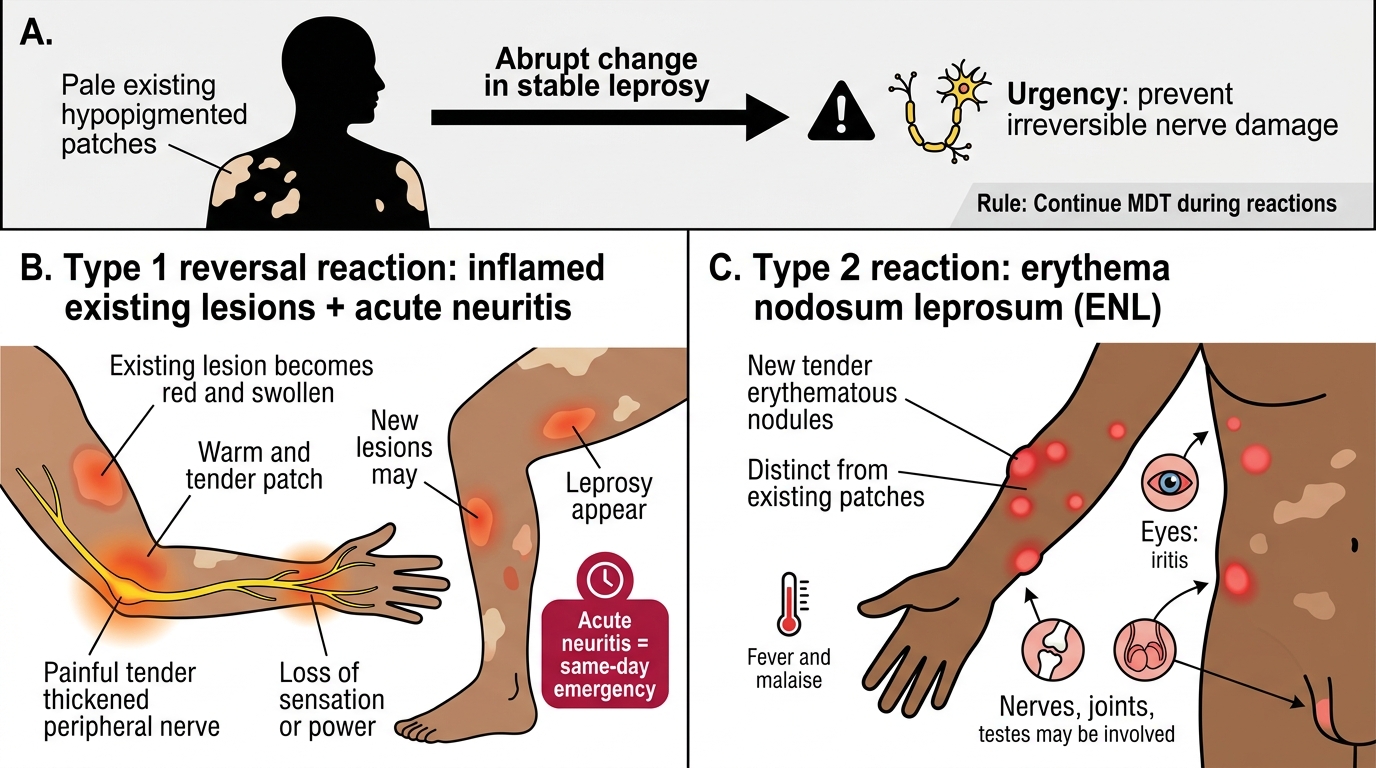
A lepra reaction announces itself as an abrupt change in a patient whose leprosy was previously stable, and recognising it quickly is what makes the difference between recovery and permanent disability. The two types present differently. A Type 1 (reversal) reaction presents with the patient's EXISTING skin lesions becoming acutely red, swollen, warm, and tender, often with new lesions appearing, and — most dangerously — with acute neuritis: a peripheral nerve becomes suddenly painful, tender, and thickened, and nerve function (sensation or power) begins to fail. A Type 2 reaction (erythema nodosum leprosum, ENL) presents with crops of NEW, tender, erythematous subcutaneous nodules distinct from the existing patches, accompanied by systemic upset — fever, malaise — and often involvement of other organs such as the eyes (iritis), nerves, joints, and testes.
What unites both reactions is urgency, because both can cause rapid, irreversible nerve damage. Acute neuritis in a Type 1 reaction is a same-day emergency: the nerve is losing function that corticosteroids can still recover, but only if treatment starts promptly. ENL, too, can be severe and recurrent, threatening the eyes and nerves and causing genuine systemic illness. The single most important rule across both is that multidrug therapy (MDT) is continued throughout the reaction — the reaction is an immunological event, not a sign of treatment failure, and stopping MDT does not help and may harm.
Red flags demanding immediate action:
- Sudden inflammation of existing lesions + a tender, thickened nerve with new weakness → Type 1 reaction with neuritis → urgent corticosteroids.
- Crops of new tender nodules + fever + red painful eye → Type 2 (ENL) → urgent treatment, assess for eye/nerve involvement.
- In every reaction: continue MDT; never stop it.
Immunological Mechanisms — Type IV vs Type III Hypersensitivity
Type IV versus Type III Hypersensitivity in Lepra Reactions
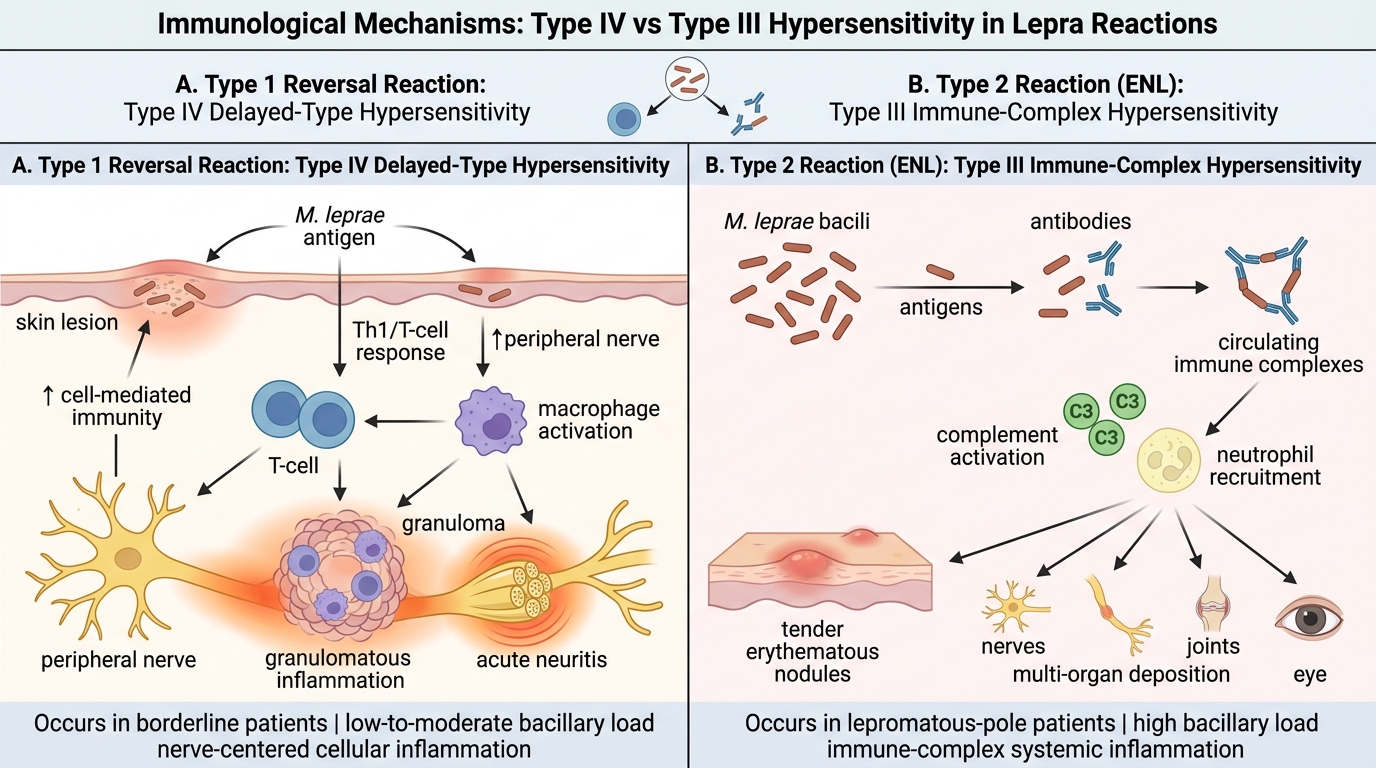
The two lepra reactions look different at the bedside because they are driven by two fundamentally different immunological mechanisms, and understanding the mechanism is the key to predicting who gets which reaction and why their treatments differ. A Type 1 (reversal) reaction is a Type IV, T-cell-mediated, delayed-type hypersensitivity event: a sudden upswing in cell-mediated immunity against M. leprae antigens (a shift toward the tuberculoid pole, hence 'reversal') causes brisk granulomatous inflammation within skin lesions and, critically, within nerves. Because it is driven by the cellular immune response attacking antigen in the nerves, its hallmark is acute neuritis, and it occurs in patients who have enough residual cell-mediated immunity to mount such a response — the immunologically unstable borderline patients.
A Type 2 reaction (ENL) is a Type III, immune-complex-mediated event. In lepromatous-pole patients carrying a huge bacillary load, the death of bacilli (often as treatment begins to work) releases abundant antigen which, with circulating antibody, forms immune complexes that deposit in skin, nerves, joints, eyes, and other tissues, activate complement, and recruit neutrophils — producing the tender nodules and multi-organ systemic features. Because it depends on a high antigen load, ENL occurs in patients at the lepromatous end of the spectrum (BL and LL). This mechanistic split also explains the treatments: corticosteroids damp down both inflammatory cascades, while clofazimine and thalidomide have specific anti-inflammatory roles in the immune-complex-driven ENL.

Leprosy Reactions: Type 1 Reversal vs Type 2 ENL
Mechanistic anchors:
- Type 1 = Type IV (T-cell/delayed) hypersensitivity → acute neuritis → in borderline (BT, BB, BL) patients.
- Type 2 (ENL) = Type III (immune-complex) hypersensitivity → tender nodules + systemic/multi-organ features → in lepromatous (BL, LL) patients.
SELF-CHECK
A patient with borderline-tuberculoid leprosy develops acute inflammation of existing skin lesions and a tender, thickened ulnar nerve with new finger weakness. Which reaction is this, what is its mechanism, and what is the first-line treatment?
A. Type 2 (ENL); immune-complex (Type III) hypersensitivity; treat with thalidomide
B. Type 1 (reversal reaction); T-cell-mediated (Type IV) hypersensitivity; treat with corticosteroids
C. Type 1 (reversal reaction); immune-complex (Type III) hypersensitivity; treat with clofazimine alone
D. Type 2 (ENL); T-cell-mediated (Type IV) hypersensitivity; treat with corticosteroids and stop MDT
Reveal Answer
Answer: B. Type 1 (reversal reaction); T-cell-mediated (Type IV) hypersensitivity; treat with corticosteroids
Acute inflammation of EXISTING lesions plus acute neuritis (tender, thickened nerve with new motor loss) in a BORDERLINE patient is a Type 1 (reversal) reaction. Its mechanism is T-cell-mediated, delayed-type (Type IV) hypersensitivity — a surge of cell-mediated immunity attacking antigen in skin and nerves. The first-line treatment is corticosteroids (e.g., prednisolone), started urgently to rescue nerve function. Thalidomide and clofazimine are for Type 2 ENL, not Type 1. And multidrug therapy is always CONTINUED during a reaction, never stopped.
Differential Diagnosis and Clinical Distinction Between Type 1 and Type 2
Clinical Distinction Between Type 1 and Type 2 Leprosy Reactions
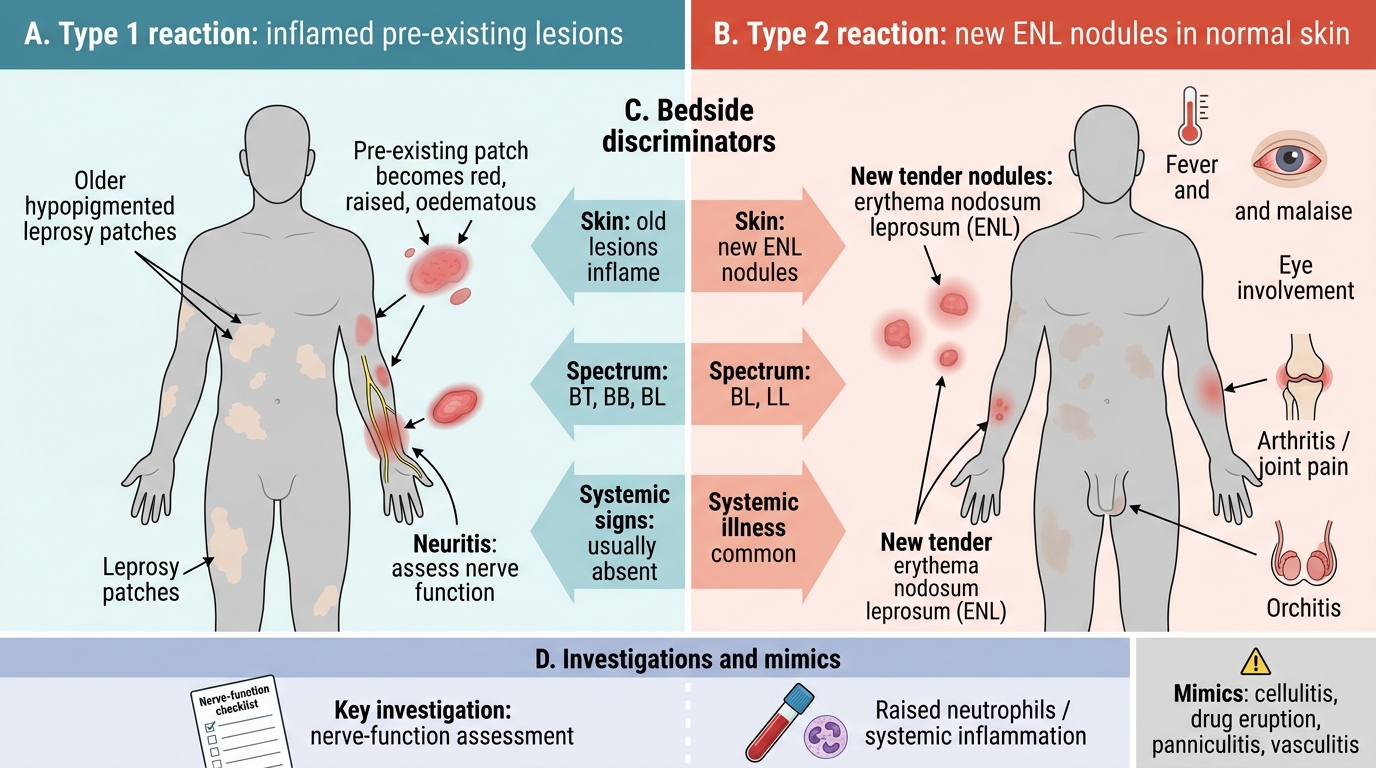
Distinguishing Type 1 from Type 2 reactions is the central clinical skill of this module, because although both may require corticosteroids, the additional drugs and the prognosis differ, and the distinction rests on a handful of reliable features. The cleanest discriminator is what the skin is doing: in a Type 1 reaction the patient's PRE-EXISTING lesions become inflamed (red, raised, oedematous), whereas in a Type 2 reaction crops of entirely NEW tender nodules (erythema nodosum leprosum) appear in apparently normal skin, separate from the old patches. The second discriminator is where on the spectrum the patient sits: Type 1 occurs in borderline disease (BT, BB, BL), Type 2 in lepromatous-end disease (BL, LL). The third is systemic involvement: Type 1 is largely confined to skin and nerves, while Type 2 is a systemic illness with fever, malaise, and frequent eye, joint, and testicular involvement.
Investigations and mimics support the bedside distinction. A Type 2 reaction often shows a raised neutrophil count and other markers of systemic inflammation, reflecting its immune-complex, neutrophil-driven mechanism; a Type 1 reaction's key 'investigation' is careful nerve-function assessment to quantify the neuritis. Both reactions can be mistaken for other conditions — cellulitis, an allergic drug eruption, or other panniculitides and vasculitides — so the context of known leprosy and the pattern of lesions guides you. The practical reason the distinction matters is therapeutic: it tells you whether you are reaching only for corticosteroids (Type 1) or whether you must add clofazimine or thalidomide for a Type 2 reaction.
| Feature | Type 1 (Reversal Reaction) | Type 2 (ENL) |
|---|---|---|
| Mechanism | T-cell-mediated, Type IV (delayed) | Immune-complex, Type III |
| Spectrum affected | Borderline (BT, BB, BL) | Lepromatous (BL, LL) |
| Skin | Existing lesions inflamed | Crops of NEW tender nodules |
| Nerve | Acute neuritis prominent | Neuritis can occur |
| Systemic features | Usually absent | Fever, malaise, iritis, arthritis, orchitis |
| Typical labs | — | Neutrophilia, raised inflammatory markers |
| Core treatment | Corticosteroids | Corticosteroids + clofazimine / thalidomide |
Key distinctions:
- Existing lesions inflamed → Type 1; new crops of nodules → Type 2.
- Borderline patient → Type 1; lepromatous patient with systemic features → Type 2.