Page 16 of 23
DR9.5 | Leprosy Management Under National Guidelines — SDL Guide
Learning Objectives
- State the rationale for multidrug therapy and the goal of preventing disability through early treatment
- Prescribe the correct WHO/NLEP multidrug-therapy regimens for paucibacillary and multibacillary leprosy, including adult and paediatric doses and durations
- Recognise the adverse effects of rifampicin, dapsone, and clofazimine and manage common drug problems including dapsone hypersensitivity
- Describe the NLEP framework for notification, release from treatment, relapse surveillance, and contact prophylaxis
INSTRUCTIONS
Leprosy is curable, and multidrug therapy (MDT) — provided free through the National Leprosy Eradication Programme — is one of the great public-health successes of modern medicine. But curing the patient and preventing their disability depend on choosing the correct regimen, giving it for the correct duration, recognising and managing drug toxicity, and following the patient through the programme's surveillance system. This module teaches you to manage a case of leprosy according to national and WHO guidelines: to select and prescribe the right MDT regimen for paucibacillary versus multibacillary disease, to adjust doses for children, to handle adverse drug reactions, and to operate within the NLEP framework of notification, release from treatment, and relapse surveillance. Getting the regimen exactly right — the right drugs, doses, and duration — is the core competency this module builds.
References
- Neena Khanna. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Leprosy — Treatment (textbook)
- National Leprosy Eradication Programme (NLEP) Operational Guidelines, Government of India; WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy 2018 (guideline)
- IADVL Textbook of Dermatology, 4th ed. Section: Leprosy — Multidrug Therapy and Programme Management (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old man is diagnosed with leprosy at your primary health centre: seven hypopigmented patches and a slit-skin smear positive at the ear lobe. His mother, terrified, asks the two questions that every leprosy family asks — 'Will he be cured?' and 'Will he be deformed?' The answers to both lie in the blister pack you are about to hand him. If you classify him correctly as multibacillary and give the right three drugs for the right twelve months, he will be cured and, if he started before nerve damage set in, spared deformity. If you mistakenly give him the shorter two-drug paucibacillary course because you counted only the patches and ignored the positive smear, you risk under-treatment and relapse. The same free medicines, supplied by the National Leprosy Eradication Programme, can either close this chapter of his life or leave it dangerously open — and which happens depends entirely on the prescribing decision you make in the next few minutes.
WHY THIS MATTERS
Knowing how to manage leprosy under national guidelines is a competency you will use directly, because MDT is delivered through general health services and a primary-care doctor is often the one who classifies the patient, hands over the blister pack, and follows them up. The stakes are concrete: the right regimen for the right duration cures the patient and, when started early, prevents the nerve damage that causes lifelong disability and stigma; the wrong regimen risks relapse, drug resistance, and continued transmission. You also need to recognise the adverse effects of the three MDT drugs so you do not stop treatment unnecessarily — or, conversely, so you act fast on a dangerous reaction like dapsone hypersensitivity. Finally, leprosy is a notifiable disease embedded in a national programme, so managing a case means working within NLEP's system of free drugs, surveillance, and contact prophylaxis.
RECALL
Before beginning, recall from the classification module the WHO operational dichotomy that drives the treatment choice: paucibacillary (PB) leprosy is 5 or fewer skin lesions AND a negative slit-skin smear, while multibacillary (MB) leprosy is more than 5 lesions OR a positive smear at any site — a positive smear always meaning MB. Recall from Pharmacology and Microbiology the three antileprosy drugs: rifampicin, a potent bactericidal agent that inhibits bacterial RNA polymerase and is also a strong hepatic enzyme inducer; dapsone, a folate-pathway antagonist (inhibits dihydropteroate synthase) that can cause haemolysis especially in G6PD deficiency; and clofazimine, a fat-soluble dye with bacteriostatic and anti-inflammatory actions that deposits in skin and causes reversible pigmentation. These mechanisms explain both why three drugs are combined and what adverse effects to watch for.
Why Early Treatment Matters — Preventing Disability Through MDT
Early MDT in Leprosy: Cure and Disability Prevention
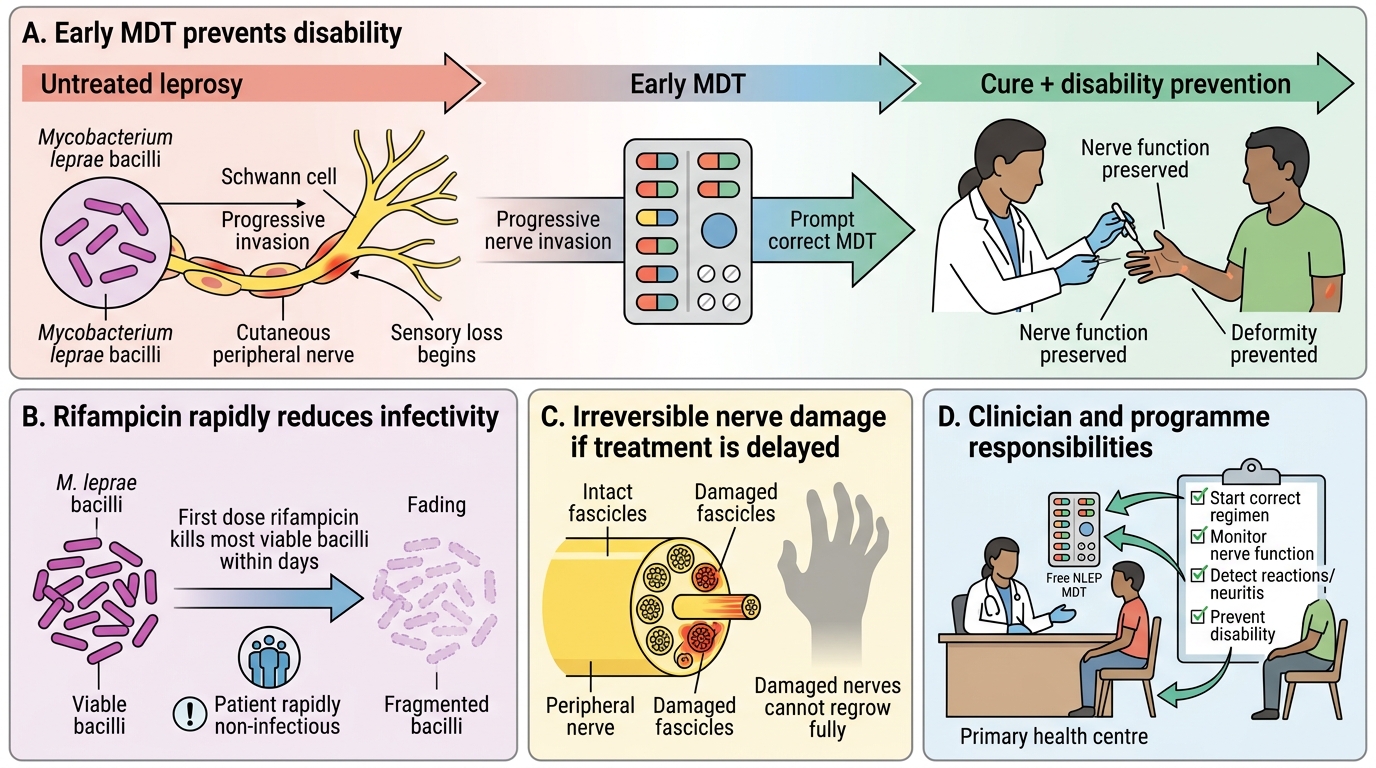
The clinical rationale for prompt, correct leprosy treatment is that multidrug therapy does two distinct jobs — it cures the infection and, when started early, it prevents the irreversible nerve damage that produces deformity, disability, and stigma. Killing M. leprae halts the progressive nerve invasion of lepromatous disease and renders the patient rapidly non-infectious; the first dose of rifampicin alone kills the great majority of viable bacilli within days, which is why a treated patient quickly ceases to be a public-health risk. But the nerves already damaged before treatment cannot be regrown, so the window for preventing disability is the time before — and during — therapy, which is exactly why early detection and early MDT are emphasised so heavily in the national programme.
This 'cure plus disability prevention' framing is what makes leprosy management more than just handing over antibiotics. The clinician must start the right regimen promptly, monitor nerve function throughout (catching reactions and treating neuritis), and provide disability-prevention measures where damage has already occurred. The programme context reinforces this: MDT is supplied free of cost by the National Leprosy Eradication Programme in standard blister packs, removing the financial barrier that once delayed treatment, and is integrated into general health services so that any primary health centre can diagnose, treat, and follow up a case.
Key points:
- MDT both cures the infection and (if started early) prevents disability — nerve damage already present is not reversible.
- The first rifampicin dose makes the patient rapidly non-infectious.
- NLEP supplies MDT free in blister packs through general health services.
Mechanisms and Rationale for the Multi-Drug Regimen
Rationale for Multi-Drug Therapy in Leprosy
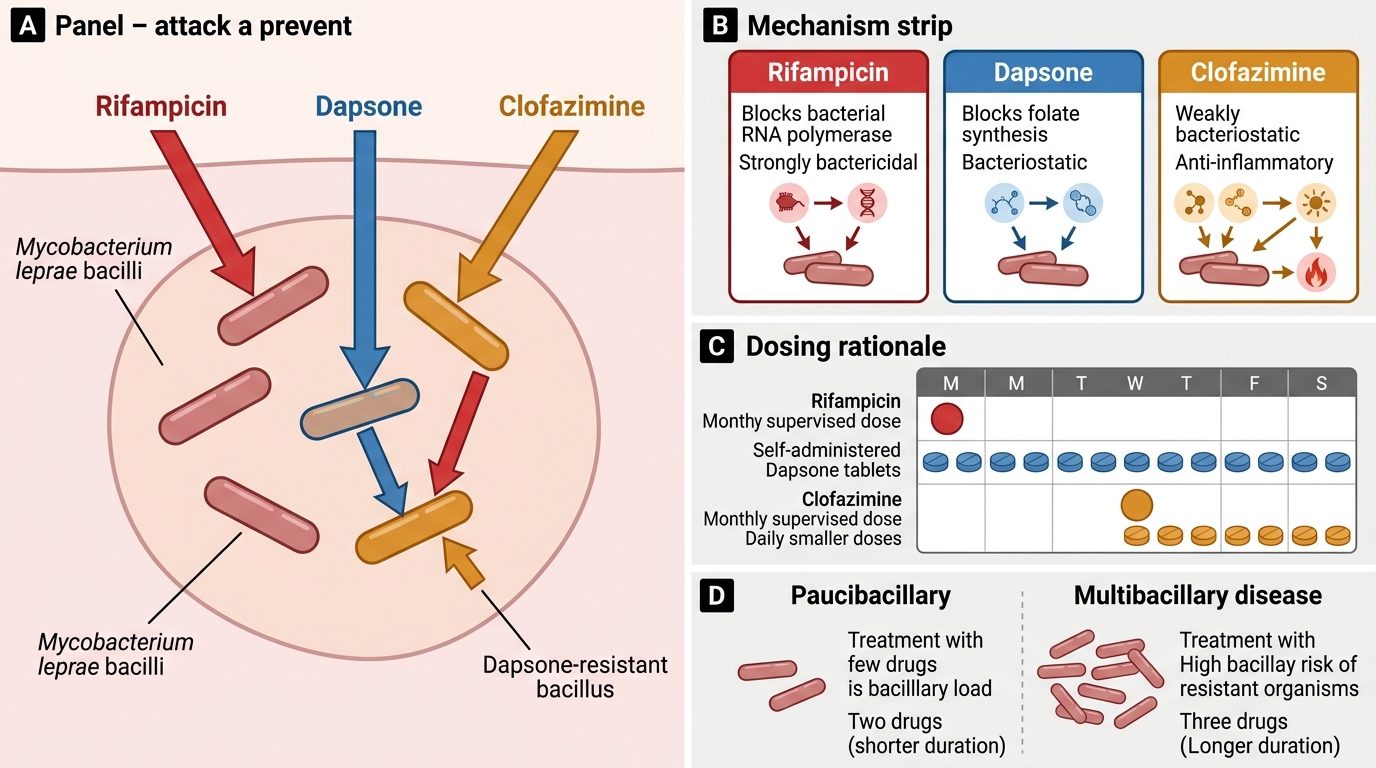
Leprosy is treated with several drugs together rather than one, and understanding why explains the structure of every regimen you will prescribe. The historical lesson is decisive: when dapsone was used alone for decades, M. leprae developed widespread resistance, and treatment failed. Combining drugs with different mechanisms of action prevents the emergence of resistance, because a bacillus resistant to one drug is still killed by the others. The three drugs also contribute complementary properties — a powerful bactericidal agent to kill rapidly, plus bacteriostatic agents to mop up the rest and (for clofazimine) to provide anti-inflammatory cover against reactions.
The individual roles follow from their pharmacology. Rifampicin is the key bactericidal drug, inhibiting bacterial RNA polymerase and killing more than 99.9% of viable bacilli after only a few doses; because it is so potent, it is given as a single supervised dose once a month. Dapsone is bacteriostatic, a folate-pathway antagonist, taken daily and self-administered. Clofazimine is weakly bacteriostatic and additionally anti-inflammatory, taken in both a monthly supervised dose and a smaller daily dose. The reason multibacillary disease needs all three drugs for longer is its enormous bacillary load and higher risk of harbouring dapsone-resistant organisms, whereas paucibacillary disease, with few bacilli, can be cured by two drugs in half the time.
Mechanistic rationale:
- Multiple drugs prevent resistance (the failure of dapsone monotherapy is the historical proof).
- Rifampicin = bactericidal (RNA polymerase inhibitor), monthly supervised; dapsone = bacteriostatic (folate antagonist), daily; clofazimine = bacteriostatic + anti-inflammatory.
- MB disease (high bacillary load, resistance risk) needs all three for 12 months; PB disease needs two drugs for 6 months.
PB-MDT and MB-MDT Regimens — Drugs, Doses, Duration
PB-MDT and MB-MDT Regimens
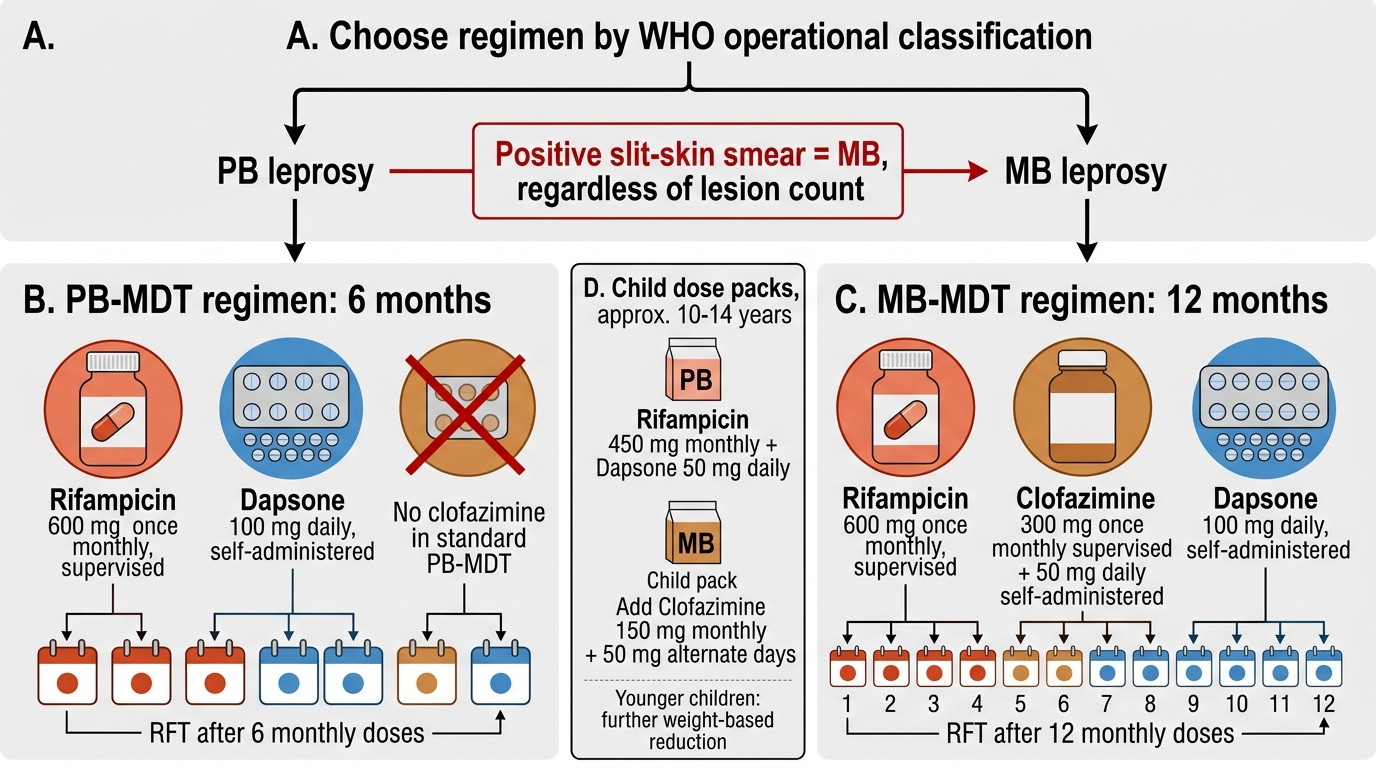
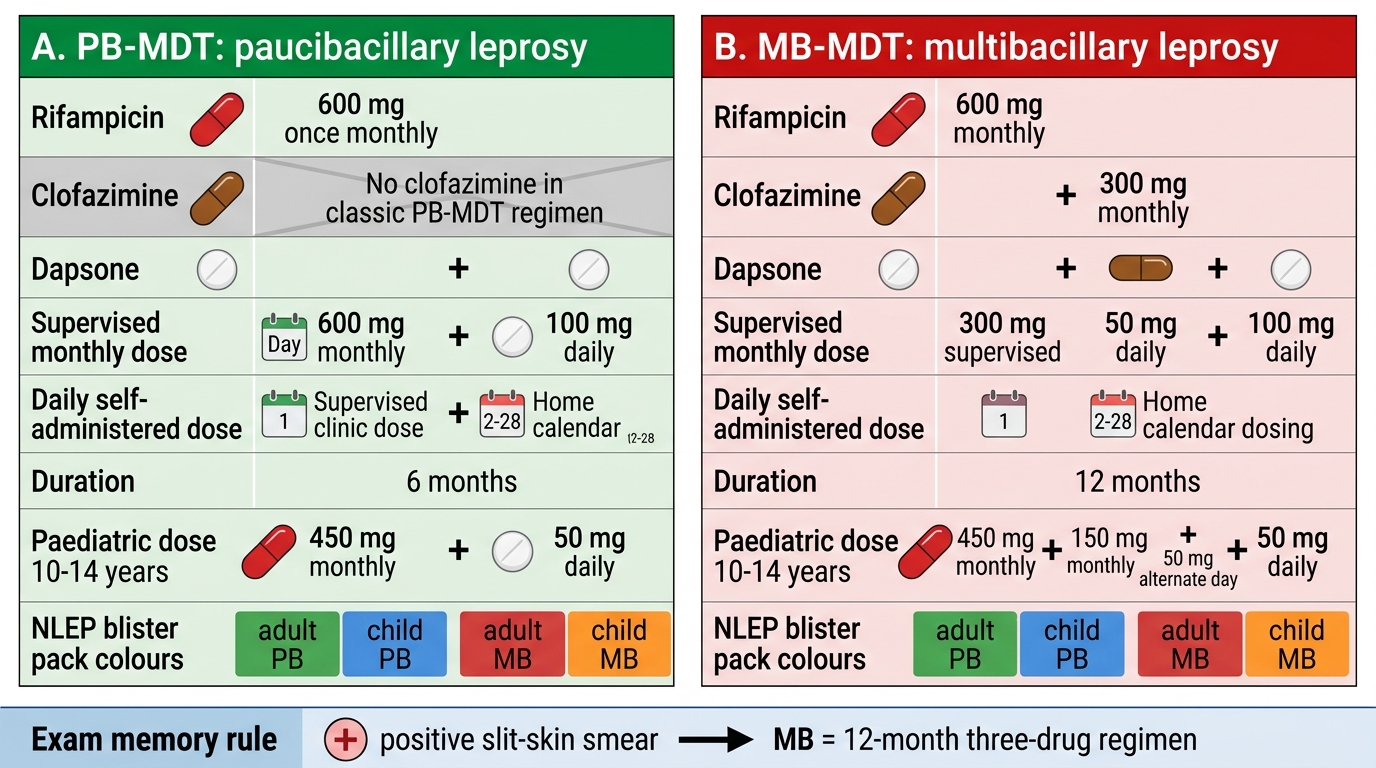
Prescribing leprosy treatment correctly comes down to two standard WHO/NLEP regimens, chosen strictly by the WHO operational classification, and you must be able to state each precisely because errors in drug, dose, or duration directly cause treatment failure. For paucibacillary (PB) leprosy, the regimen is rifampicin 600 mg once a month (supervised) plus dapsone 100 mg daily (self-administered), for 6 months — note there is no clofazimine in the standard PB regimen. For multibacillary (MB) leprosy, the regimen is rifampicin 600 mg once a month (supervised) plus clofazimine 300 mg once a month (supervised) and 50 mg daily (self-administered) plus dapsone 100 mg daily (self-administered), for 12 months. The single most important rule is that a positive smear means MB, and therefore the longer three-drug course, no matter how few lesions there are.
Doses are adjusted for children, and the standard NLEP child packs (for ages roughly 10-14 years) use rifampicin 450 mg monthly and dapsone 50 mg daily for PB, and for MB add clofazimine 150 mg monthly with 50 mg on alternate days, with further weight-based reduction for younger children. Release from treatment (RFT) occurs on completion of the course — 6 monthly doses for PB (taken within a permitted window) and 12 monthly doses for MB. These two regimens — PB = rifampicin + dapsone for 6 months, and MB = rifampicin + dapsone + clofazimine for 12 months — are the standard WHO and NLEP regimens supplied in the NLEP blister packs and are what you must know at the MBBS level; always follow current NLEP operational guidance for any local updates.
PB-MDT vs MB-MDT in Leprosy
Regimens to commit to memory:
- PB-MDT (6 months): rifampicin 600 mg monthly (supervised) + dapsone 100 mg daily. No clofazimine.
- MB-MDT (12 months): rifampicin 600 mg monthly + clofazimine 300 mg monthly (both supervised) + clofazimine 50 mg daily + dapsone 100 mg daily.
- A positive smear = MB = the 12-month three-drug regimen, regardless of lesion count.
SELF-CHECK
What is the correct standard WHO/NLEP regimen for an adult with MULTIBACILLARY leprosy?
A. Rifampicin + dapsone for 6 months
B. Rifampicin + dapsone + clofazimine for 12 months
C. Rifampicin + clofazimine for 6 months
D. Dapsone alone for 12 months
Reveal Answer
Answer: B. Rifampicin + dapsone + clofazimine for 12 months
Multibacillary (MB) leprosy is treated with three drugs — rifampicin (600 mg monthly, supervised), dapsone (100 mg daily), and clofazimine (300 mg monthly supervised plus 50 mg daily) — for 12 months. Option 1 is the paucibacillary (PB) regimen (rifampicin + dapsone for 6 months), which omits clofazimine and uses half the duration — giving it to an MB patient is under-treatment. Dapsone monotherapy (option 4) is never used because it breeds resistance. The defining errors to avoid are dropping clofazimine from MB or shortening the 12-month course.