Page 3 of 21
DR3.1 | Psoriasis Recognition and Differential Diagnosis — SDL Guide (Part 3)
Self-Assessment and Applied Differential Framework
Scaly Red Lesion Differential Framework
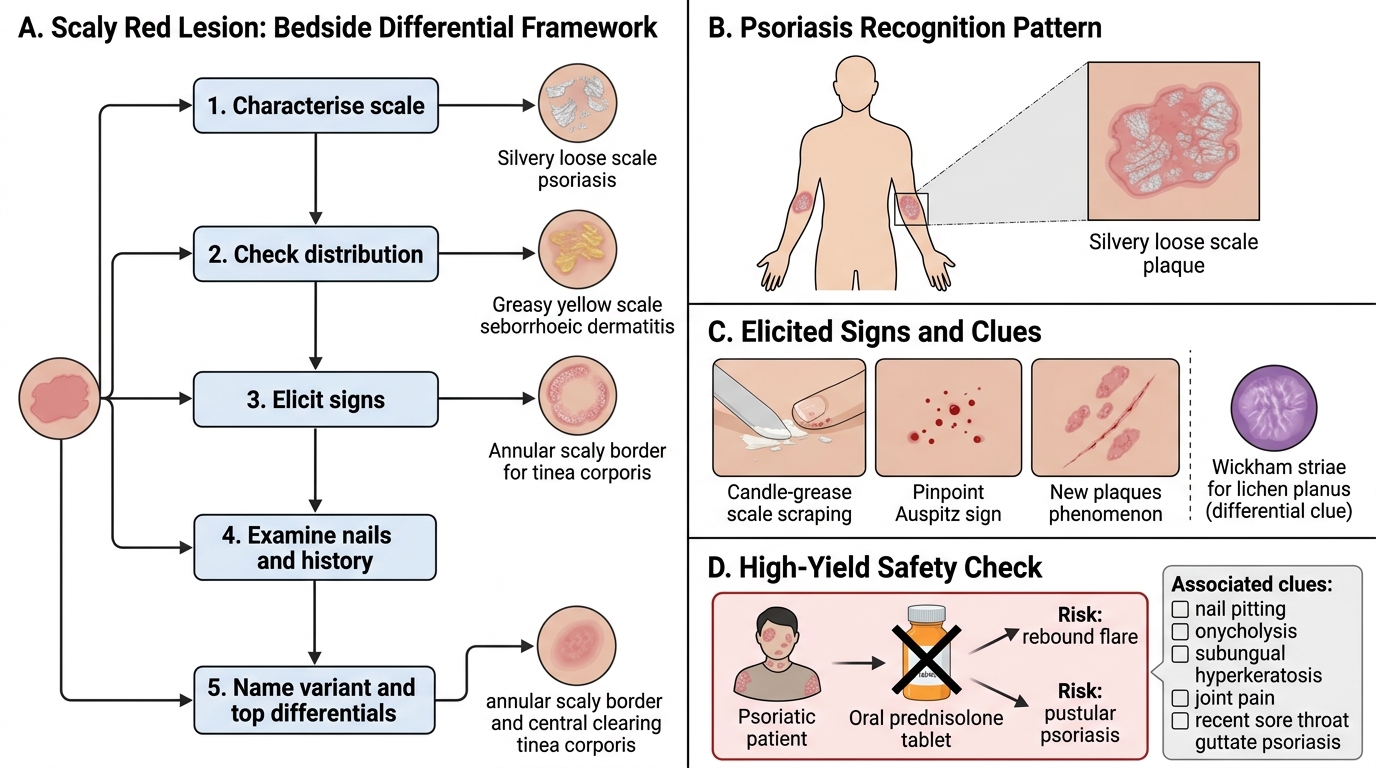
Consolidate your learning by working through the recognition reasoning yourself rather than simply recalling facts. The practised dermatologist does not memorise a list of diseases; they read a lesion's morphology, distribution, and elicited signs and then run a rapid mental differential, asking at each step "what would make this NOT psoriasis?" Use the following framework on every scaly red lesion you meet: first characterise the scale (silvery and loose, or greasy and yellow?); second, check the distribution (extensor and symmetrical, or seborrhoeic, or annular with central clearing?); third, elicit the signs (candle-grease and Auspitz present?); fourth, look at the nails and ask about joints and sore throat; and finally, name the most likely variant and its top two differentials before deciding anything else. Practising this disciplined sequence is what turns isolated facts into reliable bedside judgement.
Self-check prompts to test yourself:
- Which sign — Auspitz, Koebner, or Wickham striae — belongs to which condition, and which is shared?
- What trigger precedes guttate psoriasis, and over what time-frame?
- Name three nail changes of psoriasis.
- Why must a systemic steroid never be the answer in a psoriatic patient?
SELF-CHECK
A known plaque-psoriasis patient is admitted under medicine and a colleague suggests a short course of oral prednisolone to 'clear the skin quickly'. What is the correct advice, and why?
A. Agree — a short steroid course safely clears psoriasis with no rebound risk
B. Advise against systemic steroids — their withdrawal can precipitate a rebound generalised pustular or erythrodermic flare
C. Agree, but only if the patient also receives a topical antifungal
D. Advise against, because steroids are ineffective and have no effect on psoriasis at all
Reveal Answer
Answer: B. Advise against systemic steroids — their withdrawal can precipitate a rebound generalised pustular or erythrodermic flare
Systemic corticosteroids are contraindicated in psoriasis. Although they may transiently improve the skin, withdrawal can trigger a rebound flare into generalised pustular (Von Zumbusch) or erythrodermic psoriasis, which is potentially life-threatening. The correct advice is to avoid systemic steroids and manage psoriasis through the appropriate topical, phototherapy, or non-steroid systemic pathway. Steroids are not ineffective on the skin — the danger is specifically the rebound on withdrawal.
CLINICAL PEARL
If a 'fungal' rash on the elbows or knees fails to respond to antifungals — or worsens — stop and re-examine for psoriasis. Lift a flake of scale (candle-grease sign), scrape gently for pinpoint bleeding (Auspitz sign), and inspect the nails for pitting. A KOH mount that is negative, together with these signs, reclassifies the diagnosis. And remember the cardinal safety rule that distinguishes psoriasis from almost every other itchy red rash: never reach for a systemic steroid, because its withdrawal can flip stable plaque disease into a pustular or erythrodermic emergency.