Page 6 of 12
DR15.3 | Pyoderma Surgical Referral Decisions — SDL Guide (Part 2)
Differential Diagnosis: Distinguishing Surgical from Medical Pyoderma
Surgical vs Medical Pyoderma Triage
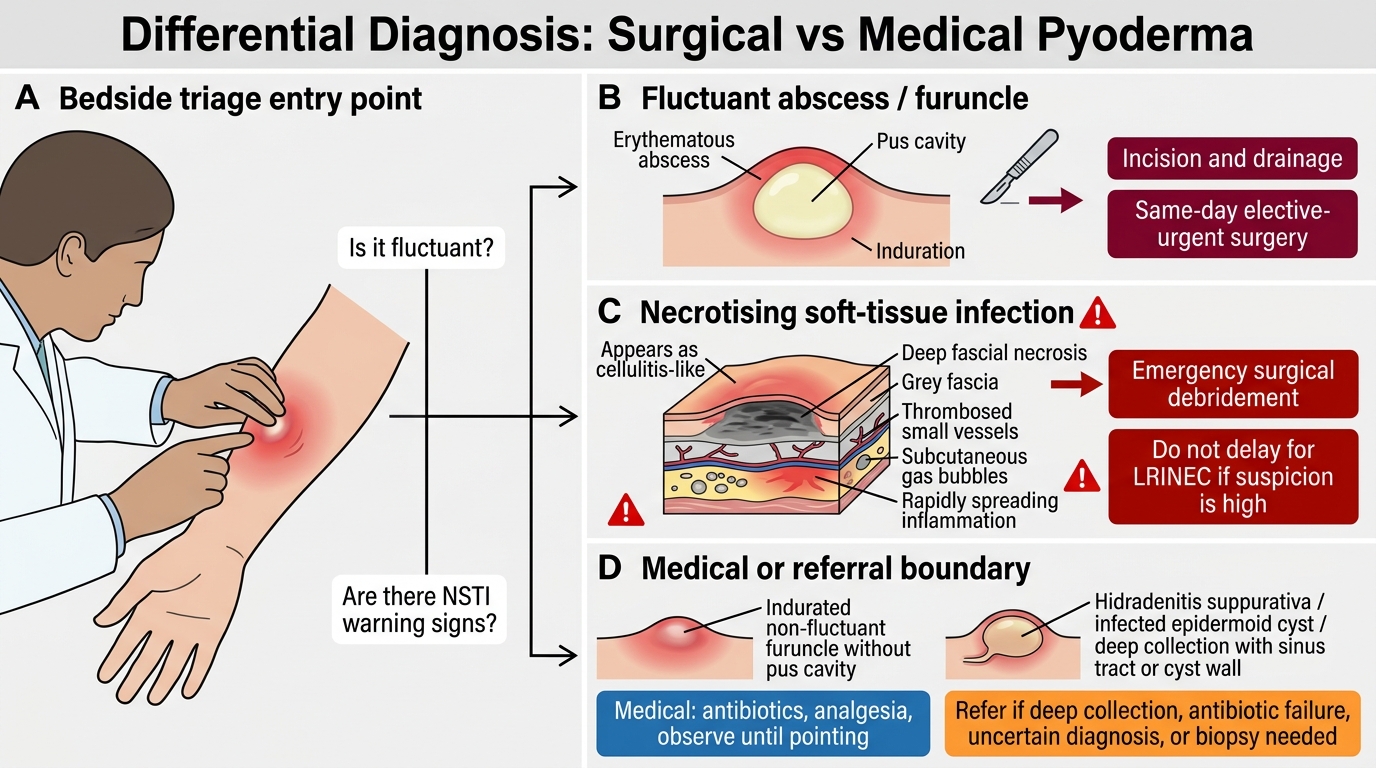
The crux of this competency is reliably separating the pyoderma that needs surgery from the one that needs only antibiotics, and doing so before harm accrues. Two distinctions carry almost all the clinical weight: a furuncle that is merely indurated (manage medically and let it 'point') versus one that has become fluctuant (drain it); and an ordinary cellulitis (manage medically) versus an early necrotising soft-tissue infection masquerading as cellulitis (a surgical emergency). Several other conditions, such as hidradenitis suppurativa and infected epidermoid cysts, sit at the boundary and may need drainage when they collect. A simple bedside scoring aid, the LRINEC score (Laboratory Risk Indicator for Necrotising Fasciitis), can raise or lower suspicion of necrotising infection, but it is an adjunct to clinical judgement and must never override a strong clinical suspicion — a high index of suspicion trumps a reassuring score.
The key contrasts:
Surgical Triage Pathways in Pyoderma
- Indurated (non-fluctuant) furuncle → antibiotics ± warm compresses; surgery not yet indicated.
- Fluctuant furuncle / carbuncle → incision and drainage (same-day, urgent).
- Cellulitis → systemic antibiotics; no surgery.
- Early necrotising soft-tissue infection → emergency surgical referral despite unimpressive skin.
- Late necrotising infection / Fournier gangrene → emergency debridement, do not delay.
When the two columns are hard to separate at the bedside, treat upward: a suspected necrotising infection is a surgical emergency until a surgeon proves otherwise.
SELF-CHECK
A diabetic patient has a 36-hour history of rapidly spreading leg erythema with severe pain that is markedly out of proportion to the visible skin changes, early crepitus, and a temperature of 39°C with tachycardia. The LRINEC score is calculated as 4. What is the most appropriate action?
A. Reassure and continue oral antibiotics, because the LRINEC score is below 6
B. Refer immediately for emergency surgical assessment, because the clinical picture strongly suggests a necrotising soft-tissue infection and clinical suspicion overrides a non-high LRINEC score
C. Admit for observation and recalculate the LRINEC score in 24 hours
D. Switch to a topical antibiotic and review in clinic next week
Reveal Answer
Answer: B. Refer immediately for emergency surgical assessment, because the clinical picture strongly suggests a necrotising soft-tissue infection and clinical suspicion overrides a non-high LRINEC score
Pain out of proportion to visible signs, rapid progression, crepitus, and systemic toxicity together describe a necrotising soft-tissue infection — a surgical emergency. The LRINEC score is only an adjunct: a score below 6 does NOT exclude the diagnosis, and a strong clinical picture must override it. The correct action is immediate referral for emergency surgical assessment and debridement, with systemic broad-spectrum (MRSA-covering) antibiotics as a bridge, not a substitute.
Surgical Referral Decisions: When, Why, and How Urgently
Surgical Referral Tiers in Pyoderma
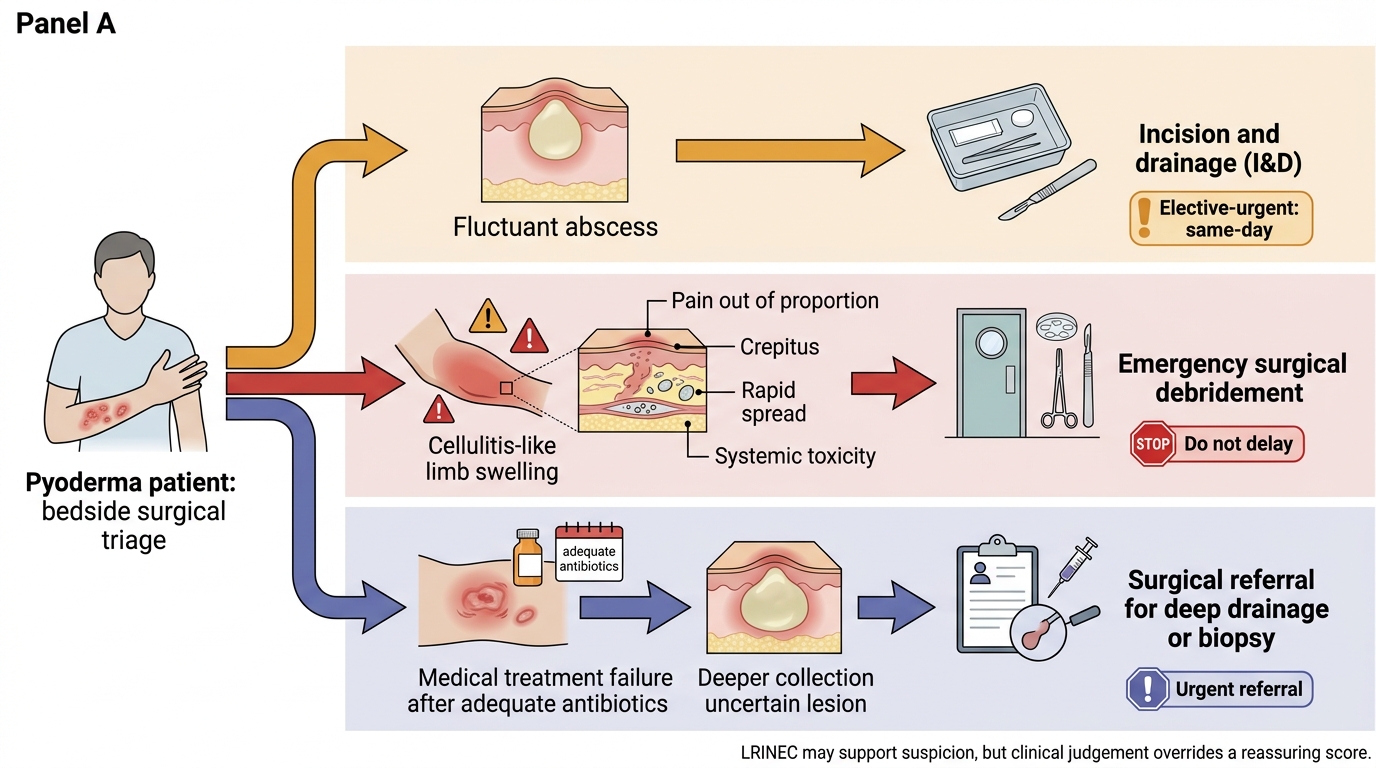
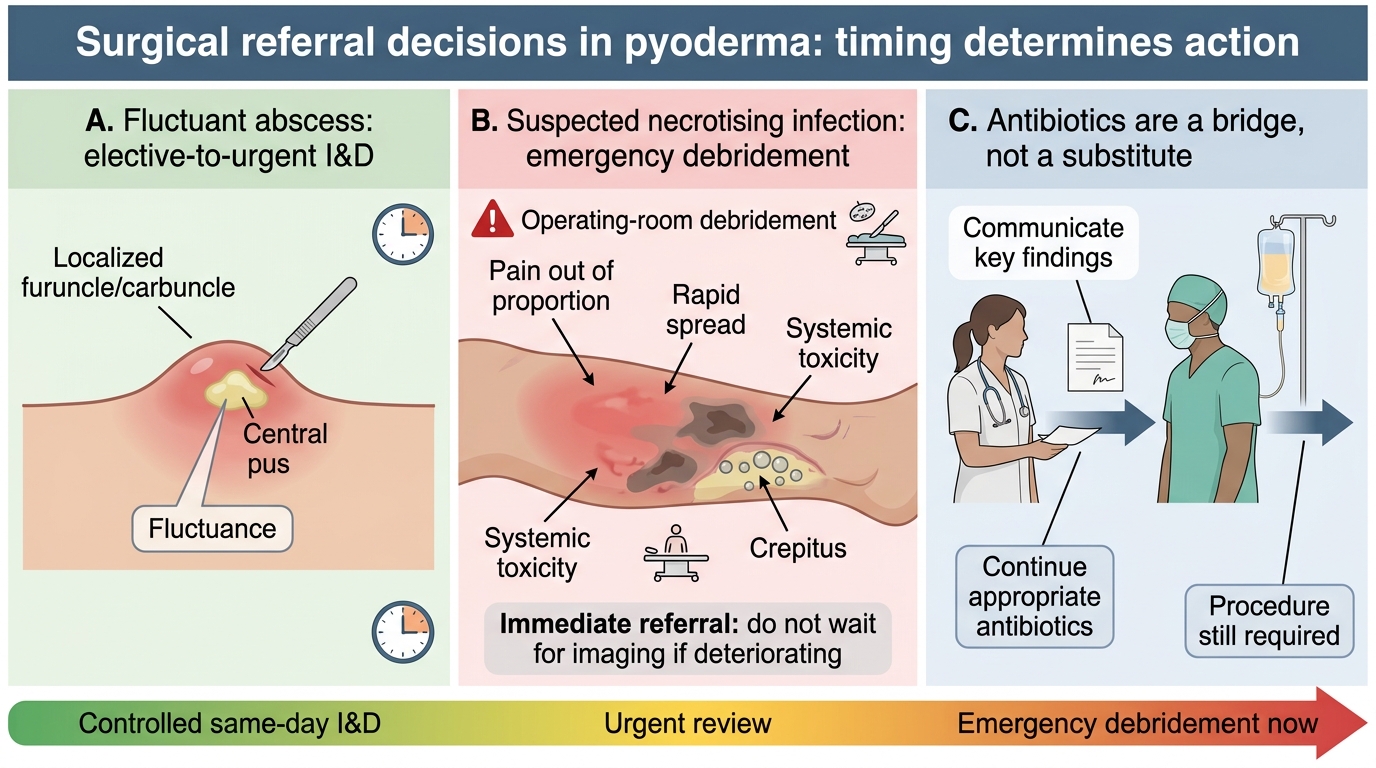
The final step is to convert recognition into a concrete, appropriately urgent referral, because in surgical pyoderma the management decision is as much about timing as about diagnosis. Surgical referral in pyoderma falls into three categories, each with a different urgency tier and a different message to the surgeon. The clinician's job is to place the patient in the right category, communicate the key clinical findings clearly, and continue the appropriate antibiotic as a bridge — never as a substitute — until the surgical procedure happens. For the necrotising infection in particular, time-to-surgery is itself a determinant of survival, so the referral must convey genuine urgency and must not be softened by an instinct to 'try antibiotics a little longer'. Getting the category and the urgency right is the whole competency in action.
The three referral categories:
- Elective-to-urgent: incision and drainage of a fluctuant abscess. Indicated for a fluctuant furuncle or carbuncle; usually a same-day, controlled procedure; continue anti-staphylococcal antibiotics around it.
- Emergency: surgical debridement of a necrotising soft-tissue infection. Indicated the moment the diagnosis is suspected (pain out of proportion, crepitus, rapid spread, systemic toxicity); refer immediately, resuscitate, and start broad-spectrum MRSA-covering antibiotics as a bridge — do not delay for imaging if the patient is deteriorating.
- Referral for inadequate medical response. Indicated when appropriate antibiotics have failed to control disease, or when deep or recurrent collections need drainage, biopsy, or definitive surgical management (for example, recurrent carbuncle or hidradenitis suppurativa).
The rule that ties it together: drain what is fluctuant, debride what is necrotising without delay, and refer what fails adequate medical therapy.
Self-Assessment: Surgical Referral Judgment in Pyoderma Cases
Pyoderma Surgical Referral Triage
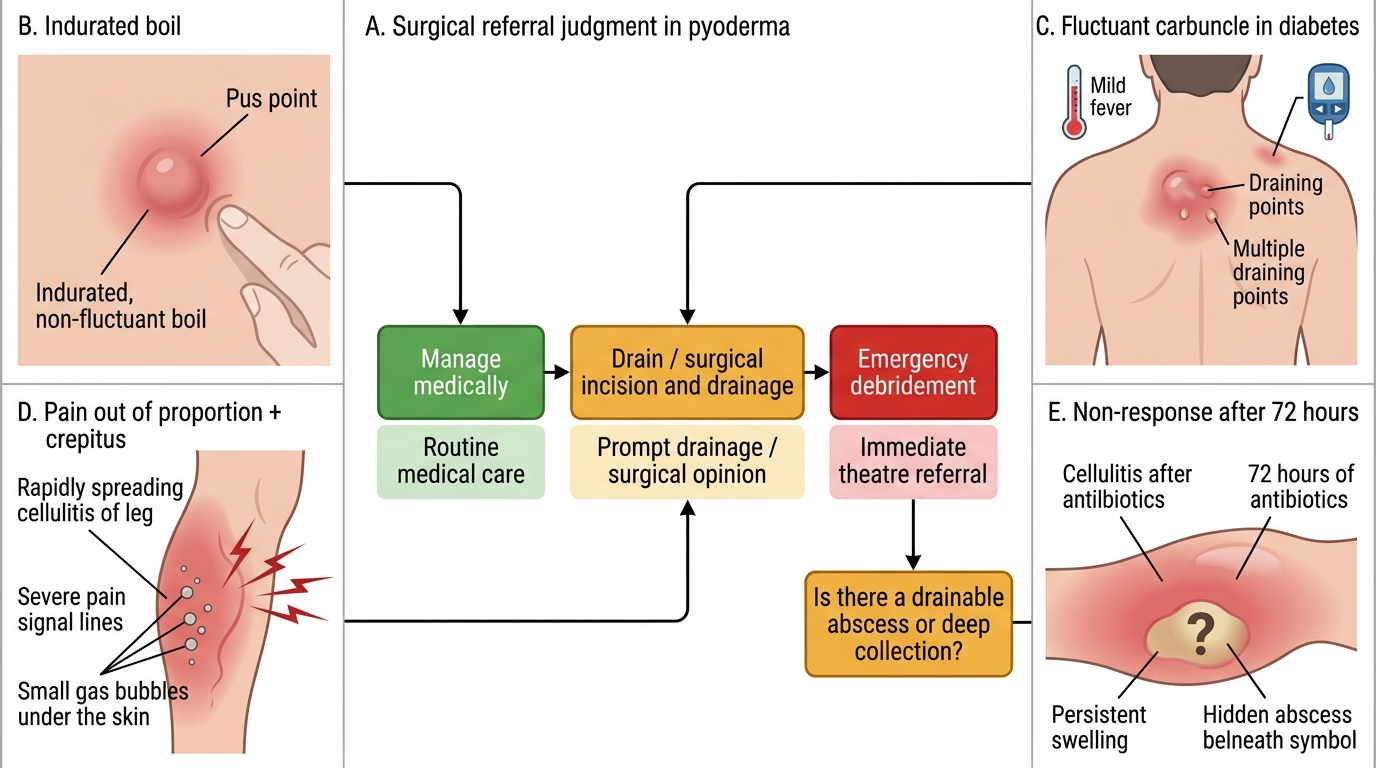
Consolidate this competency by rehearsing the referral judgement on realistic cases, because the skill being assessed is decision-making under time pressure, not the recall of isolated facts. The competency is precise: to recognise the need for surgical referral in pyoderma. Meeting it means reliably sorting patients into 'manage medically', 'drain', and 'emergency debridement', and knowing how urgently to act in each. Work through the prompts below as if you were the first doctor to see each patient, deciding in each case whether antibiotics suffice, whether the lesion needs draining, or whether you are looking at a surgical emergency that must go to theatre without delay. The ability to make that call quickly and to justify it — naming the triggering feature and the urgency tier — is exactly what this module has prepared you to do, and what real practice will demand.
Use these self-check prompts:
- An indurated but non-fluctuant boil: do you drain it now, and why or why not?
- A fluctuant carbuncle in a diabetic with mild fever: what is the management and how urgent?
- A spreading 'cellulitis' with pain out of proportion and early crepitus: what is your single most important next action?
- A cellulitis that has not responded to 72 hours of appropriate antibiotics: what surgical question do you now ask?
If you can answer all four, naming the triggering feature and the correct urgency, you have met the objective of recognising when pyoderma needs a surgeon.
CLINICAL PEARL
Pain out of proportion to the visible skin signs is the most important early warning of necrotising soft-tissue infection — act on it before the skin turns dusky. The classic late signs (crepitus, haemorrhagic bullae, skin necrosis, frank sepsis) confirm the diagnosis but appear too late to save tissue; survival depends on referring at the early, deceptively mild stage. A useful bedside rule: if a 'cellulitis' hurts far more than it looks, is spreading by the hour, or is making the patient systemically unwell, treat it as a surgical emergency until a surgeon says otherwise. The LRINEC score may support you, but a reassuring score never overrides a strong clinical suspicion. Time-to-surgery is a survival determinant — when in doubt, refer up and refer now.