Page 17 of 35
DR10.4 | Genital Ulcer Examination With Privacy and Chaperone — SDL Guide (Part 2)
Interpreting Ulcer Morphology and Lymph Node Findings
Provided image
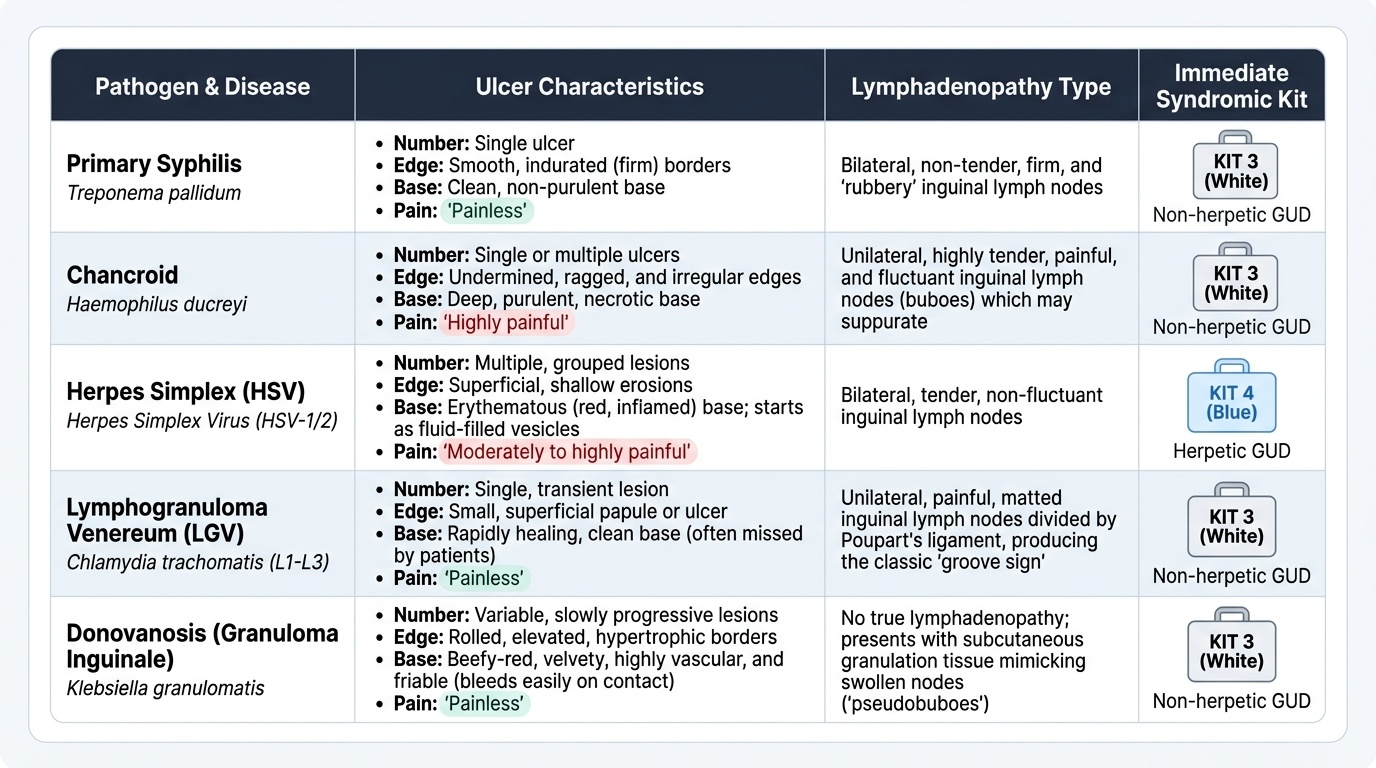
The reason morphology matters is that the physical characteristics of the ulcer and its draining nodes point reliably toward an aetiology and therefore toward the correct syndromic kit. A single, painless, indurated ulcer with a clean base and non-tender 'rubbery' inguinal nodes is the classic chancre of primary syphilis until proven otherwise. A painful, deep, purulent ulcer with an undermined ragged edge and tender, sometimes fluctuant inguinal nodes suggests chancroid (Haemophilus ducreyi). Multiple shallow, painful vesicles or erosions on an erythematous base indicate herpes simplex. A small, often-missed primary lesion followed by tender matted nodes with a groove sign points to lymphogranuloma venereum, while a beefy-red, friable ulcer with rolled edges suggests donovanosis. No single feature is pathognomonic, but the pattern of ulcer plus node guides syndromic triage and the decision between NACO Kit 3 (white, non-herpetic genital ulcer) and Kit 4 (blue, herpetic) — per current NACO guidance.
Quick morphological pointers:
- Single, painless, indurated ulcer → primary syphilis (refer VDRL/TPHA)
- Painful, deep, undermined, purulent ulcer → chancroid
- Multiple painful vesicles/erosions → herpes simplex
- Groove sign, matted tender nodes → LGV
- Beefy-red friable ulcer → donovanosis
SELF-CHECK
A male patient has a single, painless, firm (indurated) genital ulcer with a clean base and non-tender, rubbery bilateral inguinal nodes. What does this morphology most strongly suggest, and what is the appropriate next step?
A. Chancroid — incise and drain the nodes immediately
B. Herpes simplex — start acyclovir and reassure it is self-limiting
C. Primary syphilis — treat syndromically for non-herpetic genital ulcer and refer for VDRL/TPHA
D. A normal anatomical variant — no action needed
Reveal Answer
Answer: C. Primary syphilis — treat syndromically for non-herpetic genital ulcer and refer for VDRL/TPHA
A single, painless, indurated ulcer with a clean base and non-tender nodes is the classic chancre of primary syphilis until proven otherwise. The correct action is syndromic management for a non-herpetic genital ulcer (NACO Kit 3, white — per current NACO guidance) together with referral for serological confirmation (VDRL/TPHA). Chancroid is painful with undermined edges; herpes is multiple painful vesicles.
Applied Practice: Putting the Examination Together
Putting Together the STI Examination: Primary Syphilis Pattern
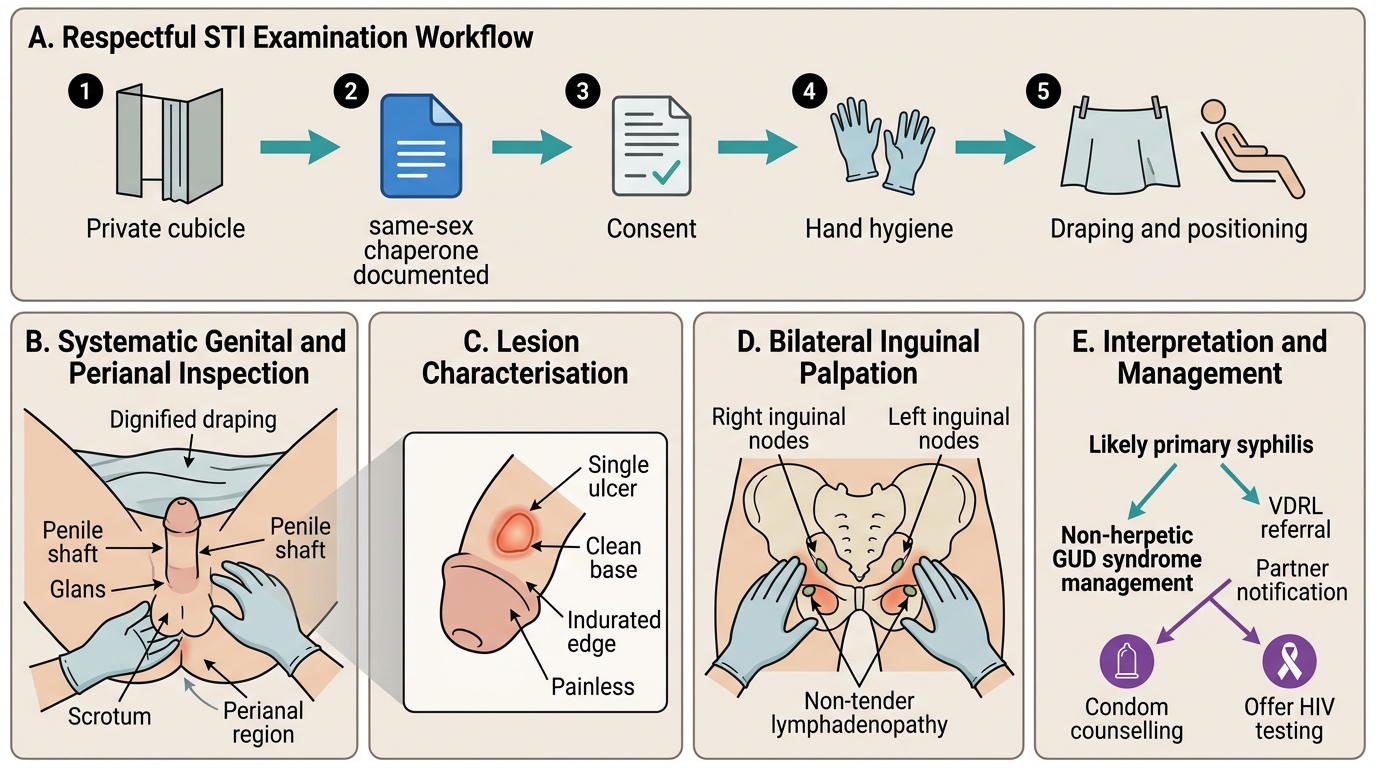
Now bring every element together in a realistic encounter, because in practice the rights framework, the technique, and the interpretation happen in one continuous flow. Imagine a 26-year-old man with a single painless penile ulcer and non-tender inguinal lymphadenopathy. You begin by securing a private cubicle and calling a same-sex chaperone, whose name you document. You explain what you need to examine and obtain consent. You don gloves, perform hand hygiene, position and drape the patient, and inspect the whole genital and perianal region, characterising the ulcer as single, painless, indurated, with a clean base — then palpate both inguinal node groups, finding them non-tender. You document the findings, recognise the pattern as likely primary syphilis, initiate syndromic management for a non-herpetic genital ulcer, refer for VDRL, and counsel the patient on partner notification, condom use, and HIV testing. The examination and the management are inseparable: a respectful, systematic examination is what makes the rest possible.
Worked sequence in this case:
1. Privacy secured, chaperone called and documented, consent taken
2. Gloves, hand hygiene, dignified positioning and draping
3. Systematic inspection → single painless indurated ulcer, clean base
4. Bilateral inguinal palpation → non-tender nodes
5. Document, triage to non-herpetic GUD syndrome, refer VDRL, counsel and offer HIV testing
SELF-CHECK
Which infection-control practice is mandatory both before and after every genital examination?
A. Sterilising the examination couch with autoclave-grade equipment
B. Hand hygiene (WHO five moments), with soiled gloves and swabs disposed into biohazard waste
C. Wearing a full surgical gown and face shield for every patient
D. Sending the patient for a shower before examination
Reveal Answer
Answer: B. Hand hygiene (WHO five moments), with soiled gloves and swabs disposed into biohazard waste
Hand hygiene before donning gloves and again after the examination — consistent with the WHO 'five moments' — is mandatory, and all soiled gloves and swabs must be disposed of in the correct biohazard waste stream. Full gowns and face shields are not routinely required for a standard genital examination, and autoclaving the couch is not the relevant control.
Self-Assessment: Genital Ulcer Examination Skills
Genital Ulcer Examination Self-Assessment Checklist
Consolidate your learning by self-assessing against the competency before you next examine a real patient, because a skill you cannot self-audit is a skill you cannot reliably reproduce. Use the structured checklist below to rehearse the full sequence mentally and to mark where you are confident and where you still need supervised practice. Honest self-assessment of consent, chaperone documentation, systematic technique, and morphological interpretation is what converts a memorised list into a dependable clinical reflex, and it is exactly what an OSPE examiner will score you on. Work through each item slowly the first few times rather than rushing, since the discipline of completing every step in order is what prevents you from skipping consent under time pressure or forgetting to palpate the second inguinal node group. Revisit any item you cannot perform smoothly with a faculty member before you are signed off, and treat any gap as a prompt for deliberate practice rather than a reason for discouragement.
Self-check items:
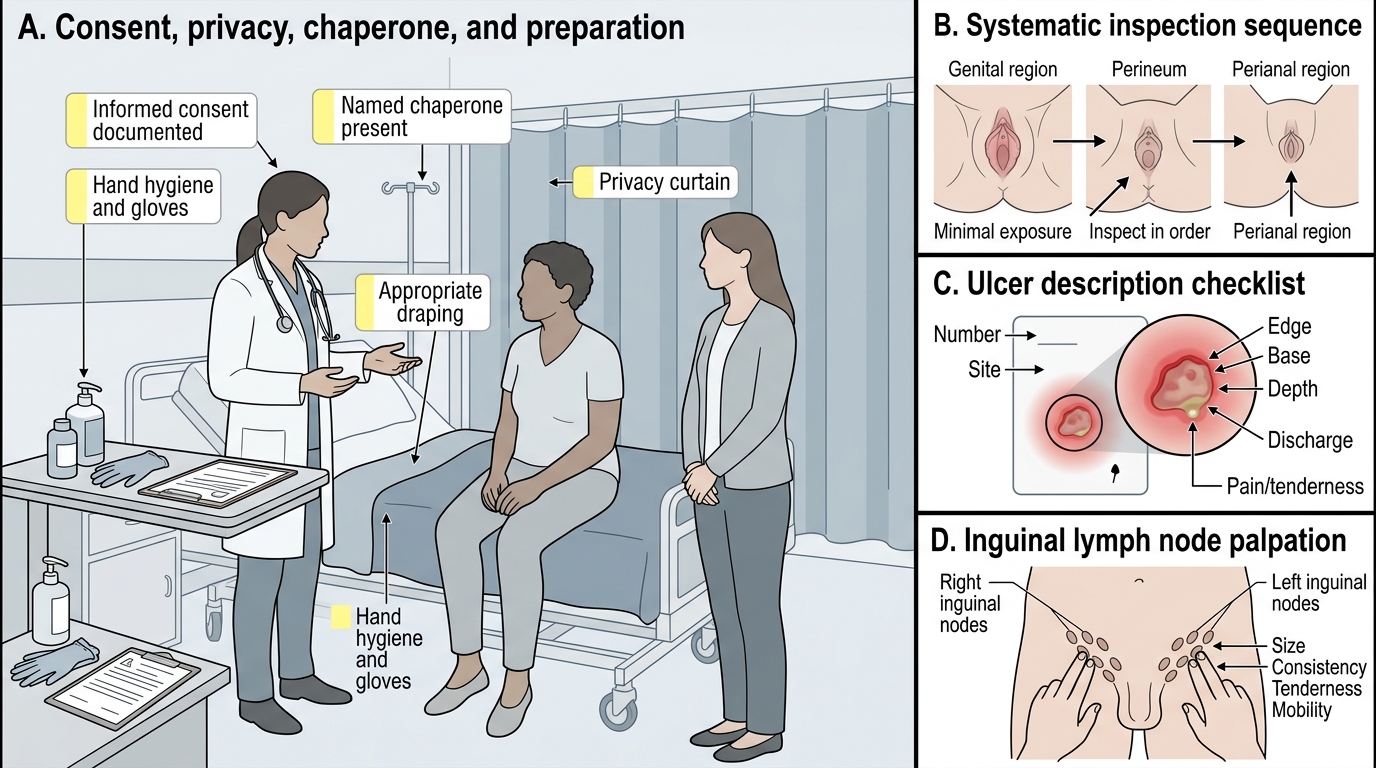
- Did I obtain and document informed consent before examining?
- Was a chaperone present and named in the record?
- Did I secure privacy and use appropriate draping with minimal exposure?
- Did I inspect the whole genital, perineal, and perianal region systematically?
- For each ulcer, did I record number, site, edge, base, depth, discharge, and pain?
- Did I palpate both inguinal node groups for size, consistency, tenderness, matting, and fluctuance?
- Did I triage to the correct NACO syndromic category and arrange counselling, partner notification, and HIV testing?
CLINICAL PEARL
If a male patient has a genital ulcer you cannot retract the prepuce over, do not force it — phimosis can hide a sub-preputial chancre or chancroid, and forcing causes pain and paraphimosis. Examine what you can, document the limitation, treat syndromically, and arrange review. And remember: a painless ulcer is more sinister than a painful one — patients often delay presenting precisely because it does not hurt, while primary syphilis silently transmits. 'Painless' should raise, not lower, your index of suspicion.