Page 28 of 35
DR10.11 | Genital Wart Diagnosis Treatment and Education — SDL Guide
Learning Objectives
- Recognise the morphology and clinical presentation of genital warts (condylomata acuminata) and name the causative HPV types.
- Describe the etiopathogenesis of HPV infection, distinguishing low-risk (6, 11) from high-risk oncogenic (16, 18) types.
- Differentiate genital warts from condylomata lata, molluscum contagiosum, and pearly penile papules, and select appropriate investigations.
- Select an appropriate treatment for genital warts, note the pregnancy contraindication of podophyllotoxin, and provide patient education including HPV vaccination and cervical screening.
INSTRUCTIONS
Genital warts are common, distressing, and an opportunity for prevention that is too often missed. This module teaches you to diagnose condylomata acuminata, distinguish them from their important mimics — especially the condylomata lata of secondary syphilis — choose a safe and effective treatment, and use the consultation to educate the patient about HPV, vaccination, and cervical cancer screening (competency DR10.11). A single point of safety runs through it: podophyllotoxin is contraindicated in pregnancy, so you must always ask about pregnancy before prescribing patient-applied therapy.
References
- NACO National Guidelines on Prevention, Management and Control of STI/RTI (Genital Warts) (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, Genital Warts / HPV (textbook)
- IADVL Textbook of Dermatology, chapter on Human Papillomavirus Infections and Anogenital Warts (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old woman presents with several soft, fleshy, cauliflower-like growths around the vulva. She is frightened they are cancer. The reassuring truth is that these are condylomata acuminata caused by low-risk HPV types 6 and 11, which do not themselves cause cancer. But the consultation hides a second, easily missed question: are these warts really HPV warts, or could they be the flat, moist condylomata lata of secondary syphilis — a completely different disease needing a completely different treatment and a VDRL test? And there is a third opportunity: this visit is the moment to talk about HPV vaccination and cervical screening, because the same virus family that causes warts includes the high-risk types that cause cervical cancer. Diagnosis, differentiation, treatment, and education all live in this one encounter.
WHY THIS MATTERS
Genital warts are one of the most common viral STIs and a frequent reason patients attend dermatology and STI clinics, so you will diagnose and treat them often. Getting the diagnosis right matters because their most important mimic — condylomata lata — signals secondary syphilis, a serious systemic infection that demands different management. Treatment choice matters for both efficacy and safety, most acutely the contraindication of podophyllotoxin in pregnancy. And the consultation is a high-value prevention opportunity: counselling on HPV vaccination protects against the oncogenic types (16 and 18) responsible for most cervical cancers, and prompting cervical screening can save a life. Competency DR10.11 captures this whole package — diagnose, treat, and educate the patient with genital warts.
RECALL
Recall from Year-1 Microbiology that human papillomavirus is a small, non-enveloped, double-stranded DNA virus that infects basal keratinocytes through micro-abrasions, and that its oncogenic potential lies in the E6 and E7 proteins of high-risk types, which inactivate the tumour-suppressors p53 and Rb. Recall from Pathology the concept of koilocytes — the vacuolated epithelial cells characteristic of HPV infection. You will also draw on the genital examination skills and the consent-and-chaperone framework from DR10.4 before examining or treating any anogenital lesion.
Genital Wart Morphology and Clinical Presentation
Genital Wart Morphology and Clinical Presentation
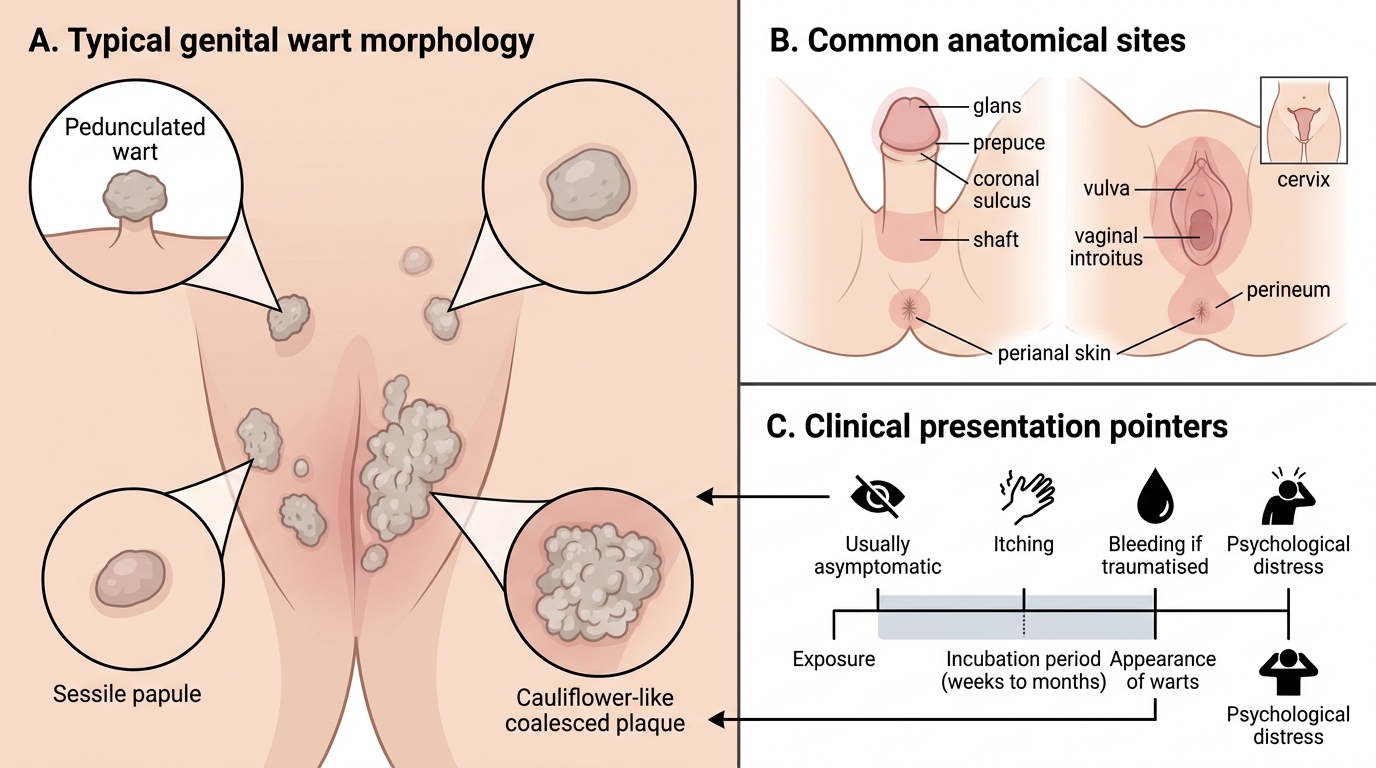
The clinical recognition of genital warts begins with their characteristic morphology, which is usually distinctive enough to suggest the diagnosis at a glance. Condylomata acuminata are soft, flesh-coloured to greyish, pedunculated or sessile, often cauliflower-like growths that may be single or multiple and can coalesce into larger plaques in warm moist areas. In men they favour the glans, prepuce, coronal sulcus, shaft, and the perianal region; in women they appear on the vulva, vaginal introitus, perineum, perianal skin, and sometimes the cervix. In moist sites they may look flatter or more papular. The incubation period is variable — typically weeks to several months after exposure — so patients often cannot pinpoint the contact. Most warts are asymptomatic, though they may itch, bleed if traumatised, or cause distress out of proportion to their size. Recognising this morphology is the first step before differentiating warts from their mimics.
Morphological pointers:
- Soft, flesh-coloured, cauliflower-like, pedunculated or sessile growths
- Men: glans, prepuce, coronal sulcus, shaft, perianal; Women: vulva, introitus, perineum, perianal, cervix
- Incubation weeks to months; usually asymptomatic, may itch or bleed
HPV Biology: Low-Risk vs High-Risk Types and Transmission
HPV Biology: Low-Risk Warts vs High-Risk Cancer
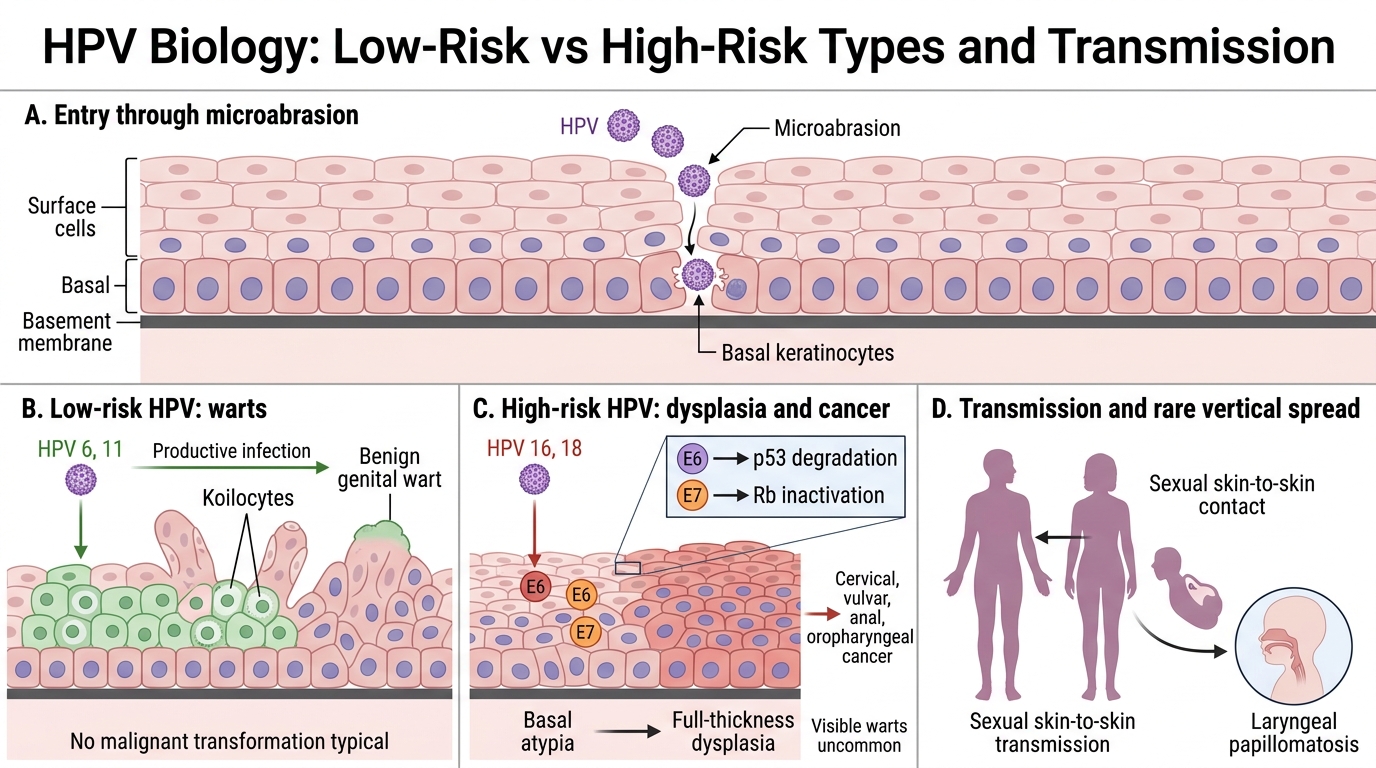
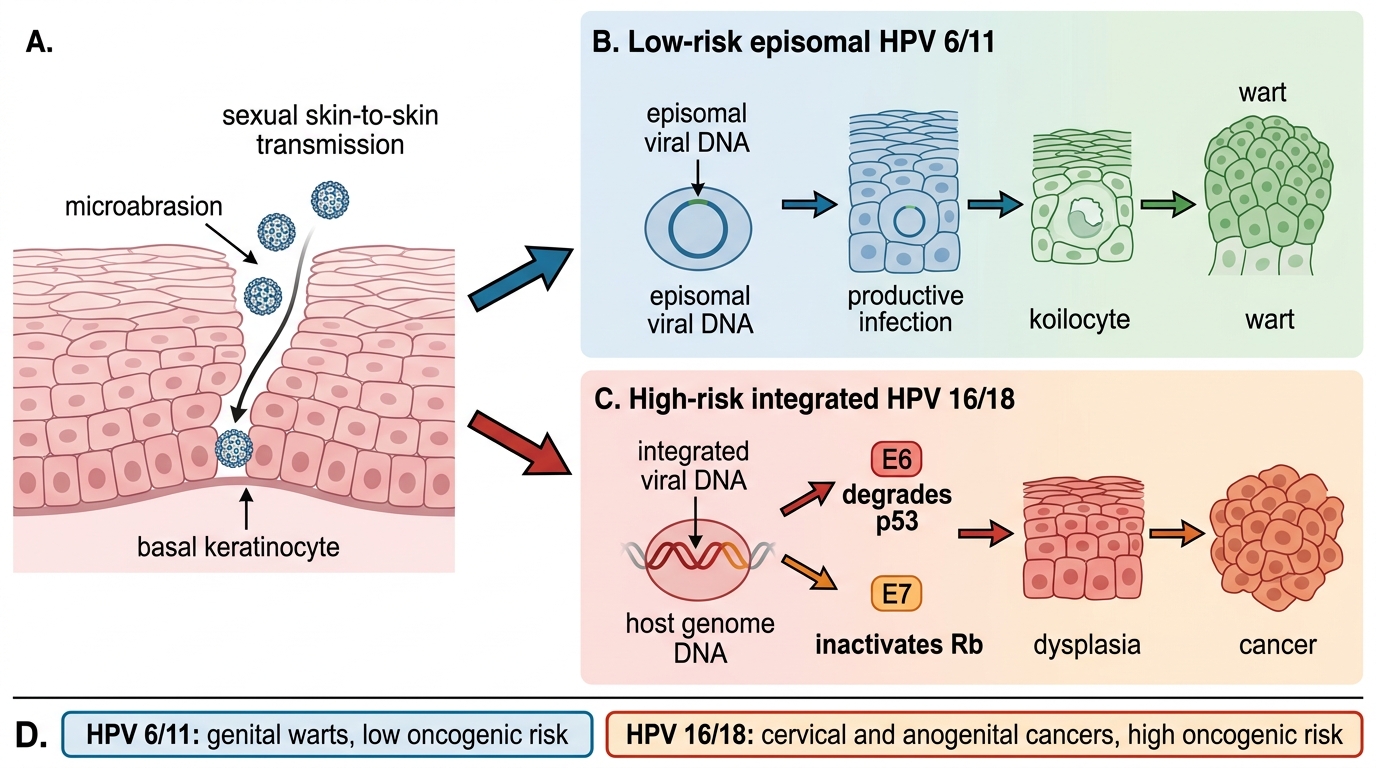
The etiopathogenesis of genital warts explains both why they form and why HPV matters far beyond the warts themselves. HPV infects basal keratinocytes exposed by micro-abrasions during skin-to-skin sexual contact. Low-risk types 6 and 11 cause the overwhelming majority of genital warts: they drive a productive infection that produces koilocytes and benign warty proliferation but do not transform cells malignantly. High-risk types — chiefly 16 and 18 (with others such as 31, 33, 45, 52, 58) — behave very differently: their E6 and E7 oncoproteins degrade p53 and inactivate Rb, driving the dysplasia that can progress to cervical, vulvar, anal, and oropharyngeal cancer; these types do not usually cause typical visible warts. Transmission is by sexual skin-to-skin contact, and vertical transmission during delivery can rarely cause laryngeal papillomatosis in the neonate. This dual personality of HPV — benign warts from low-risk types, cancer from high-risk types — is the conceptual heart of patient education later.
HPV Infection Pathway: Low-Risk Warts vs High-Risk Cancer
HPV biology summary:
- Low-risk HPV 6 and 11 → genital warts (benign, non-oncogenic)
- High-risk HPV 16 and 18 → E6/E7 inactivate p53/Rb → cervical and anogenital cancers
- Transmission: sexual skin-to-skin contact; rarely vertical (laryngeal papillomatosis)
SELF-CHECK
Which HPV types cause the majority of genital warts, and how do they relate to cancer risk?
A. Types 16 and 18, which directly cause the visible warts and most cervical cancers
B. Types 6 and 11 (low-risk), which cause most genital warts but are NOT the main oncogenic types; types 16 and 18 are the main high-risk oncogenic types
C. Types 6 and 11, which are the main cause of cervical cancer
D. All HPV types are equally oncogenic
Reveal Answer
Answer: B. Types 6 and 11 (low-risk), which cause most genital warts but are NOT the main oncogenic types; types 16 and 18 are the main high-risk oncogenic types
Low-risk HPV types 6 and 11 cause about 90% of genital warts and are non-oncogenic. The high-risk oncogenic types — chiefly 16 and 18 — cause most cervical and other anogenital cancers but do not typically cause visible warts. Distinguishing low-risk from high-risk types is central to patient counselling.
Diagnosis: Clinical Features and Differential Diagnosis
Genital Papules and Plaques: Key Differentials
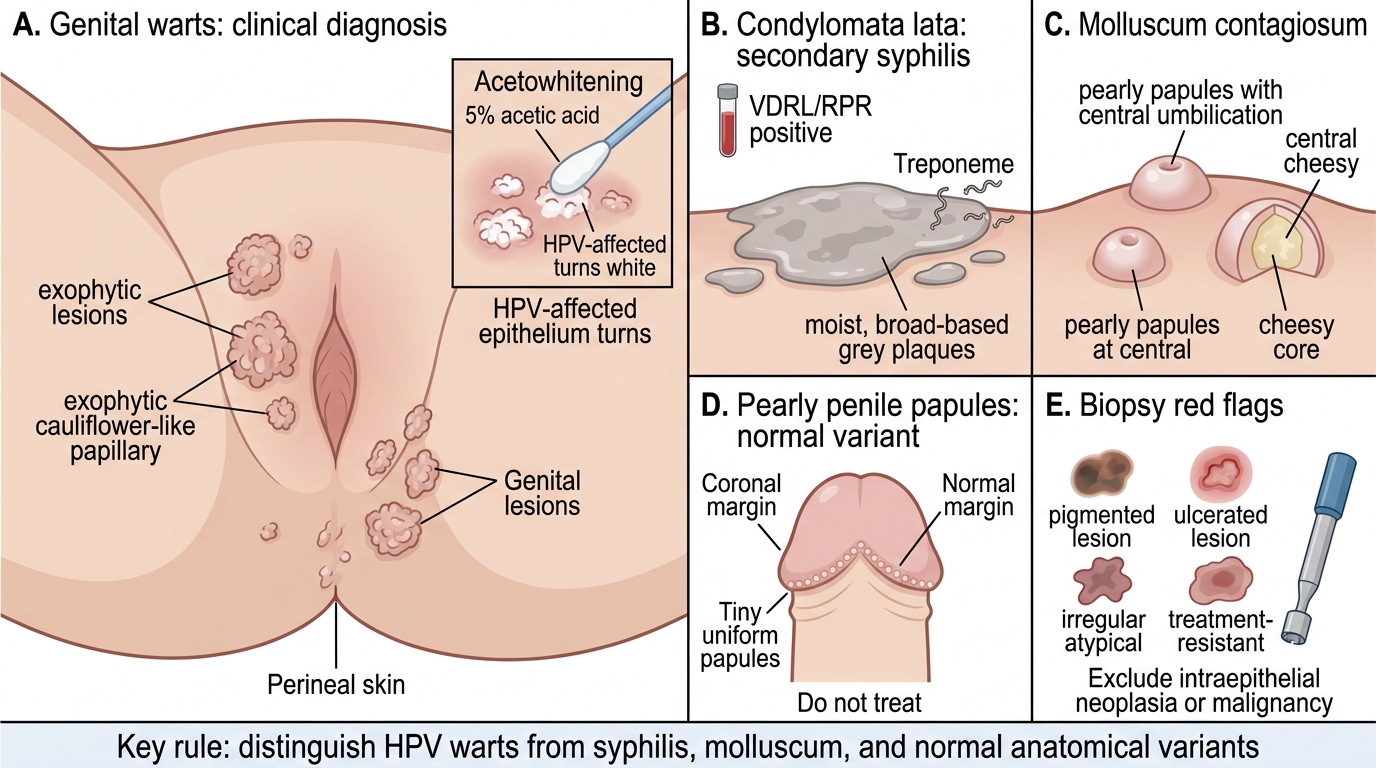
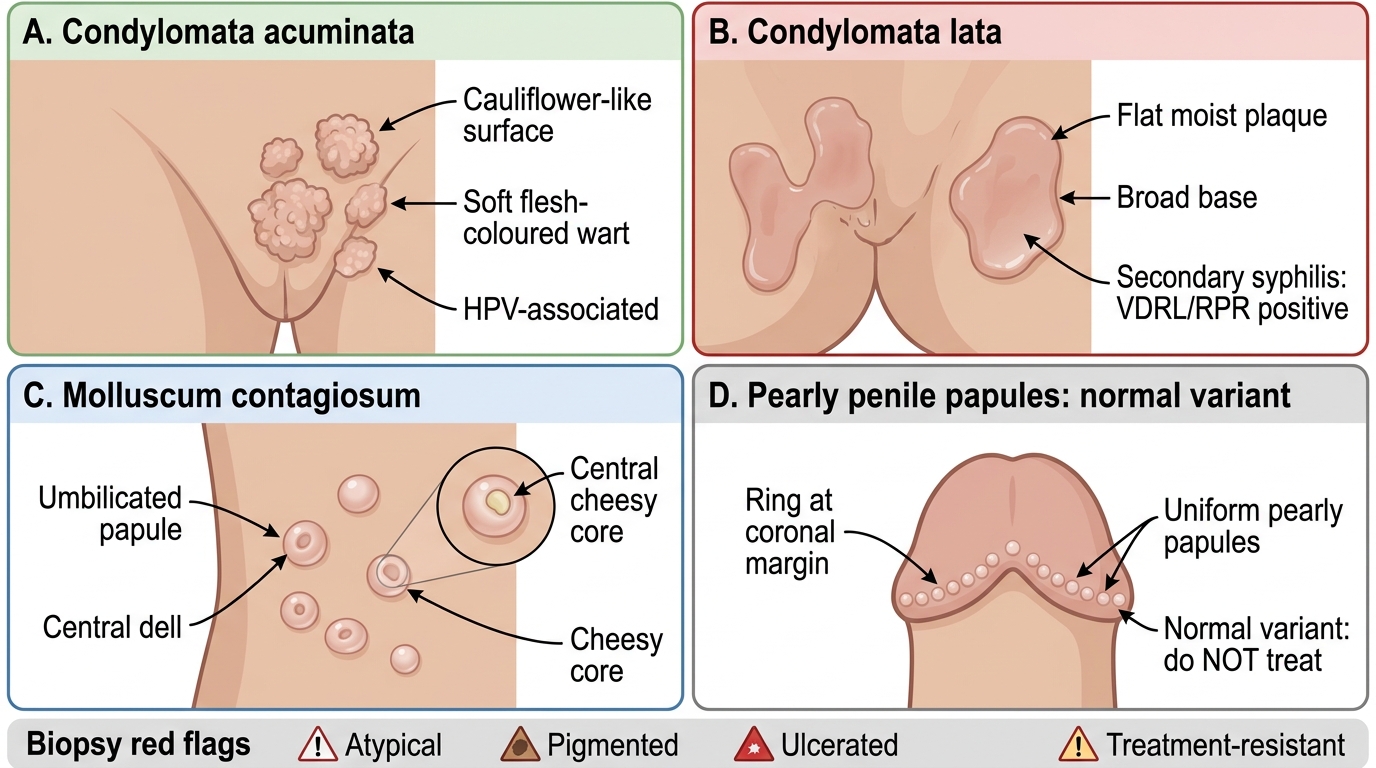
Diagnosis is usually clinical, but the differential diagnosis is where careful clinicians earn their keep. Genital warts are typically diagnosed on their cauliflower-like morphology; an acetowhitening test (applying 5% acetic acid, which turns HPV-affected epithelium white) can help reveal subclinical lesions. The crucial differentials are: condylomata lata of secondary syphilis — flat, moist, broad-based, grey lesions that are teeming with treponemes and accompanied by a positive VDRL/RPR — which must not be mistaken for HPV warts; molluscum contagiosum — dome-shaped, umbilicated papules with a central cheesy core; and pearly penile papules — a normal anatomical variant forming a ring of tiny uniform papules at the coronal margin, which must not be treated. Biopsy is indicated for atypical, pigmented, ulcerated, or treatment-resistant lesions to exclude intraepithelial neoplasia or malignancy. Getting this differential right prevents both the under-diagnosis of syphilis and the needless treatment of a normal variant.
Genital Papules and Plaques: Key Differentials
Differential pointers:
- Condylomata lata (secondary syphilis): flat, moist, broad-based; VDRL/RPR positive
- Molluscum contagiosum: umbilicated papules with cheesy core
- Pearly penile papules: normal variant, ring at coronal margin, do NOT treat
- Biopsy if atypical, pigmented, ulcerated, or treatment-resistant