Page 20 of 35
DR10.7 | Inguinal Bubo Syndromic Management — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Inguinal Bubo: Differential Diagnosis and Investigations
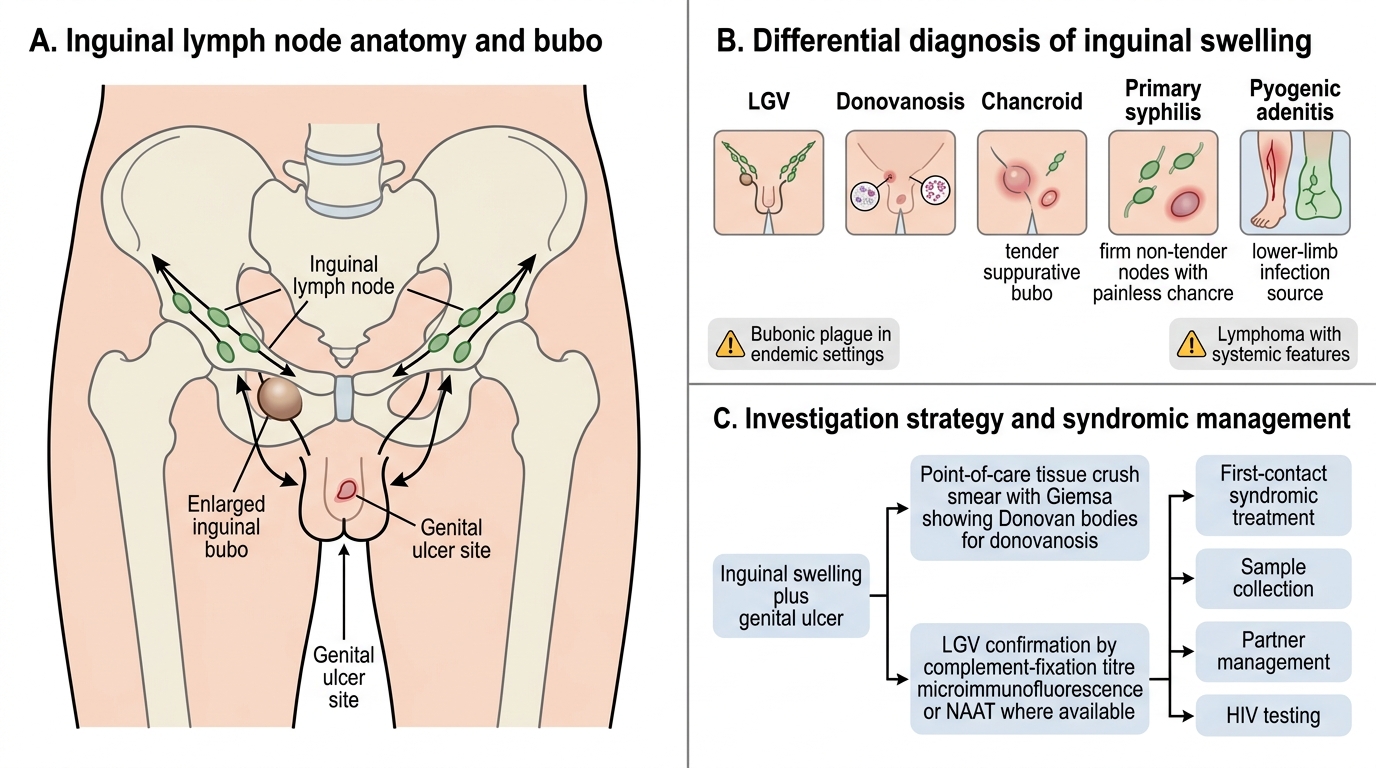
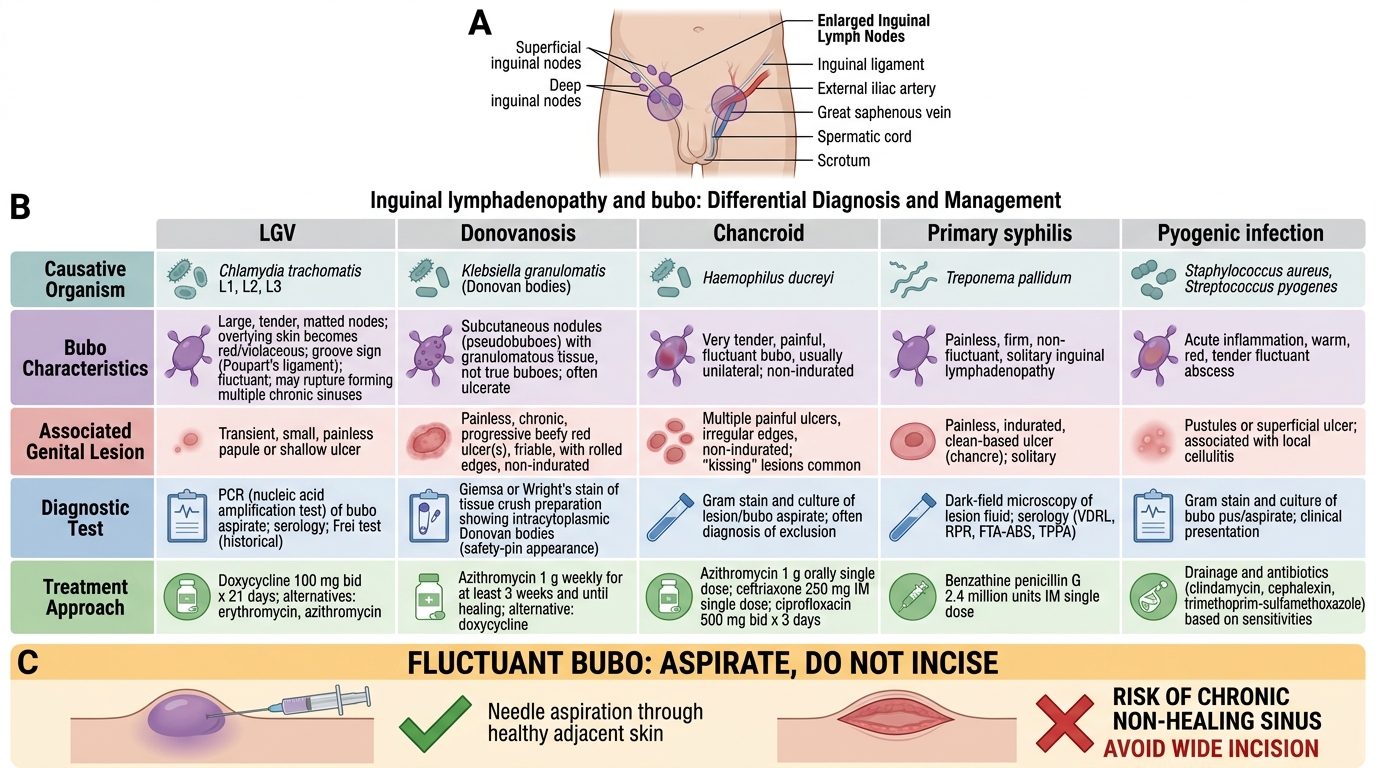
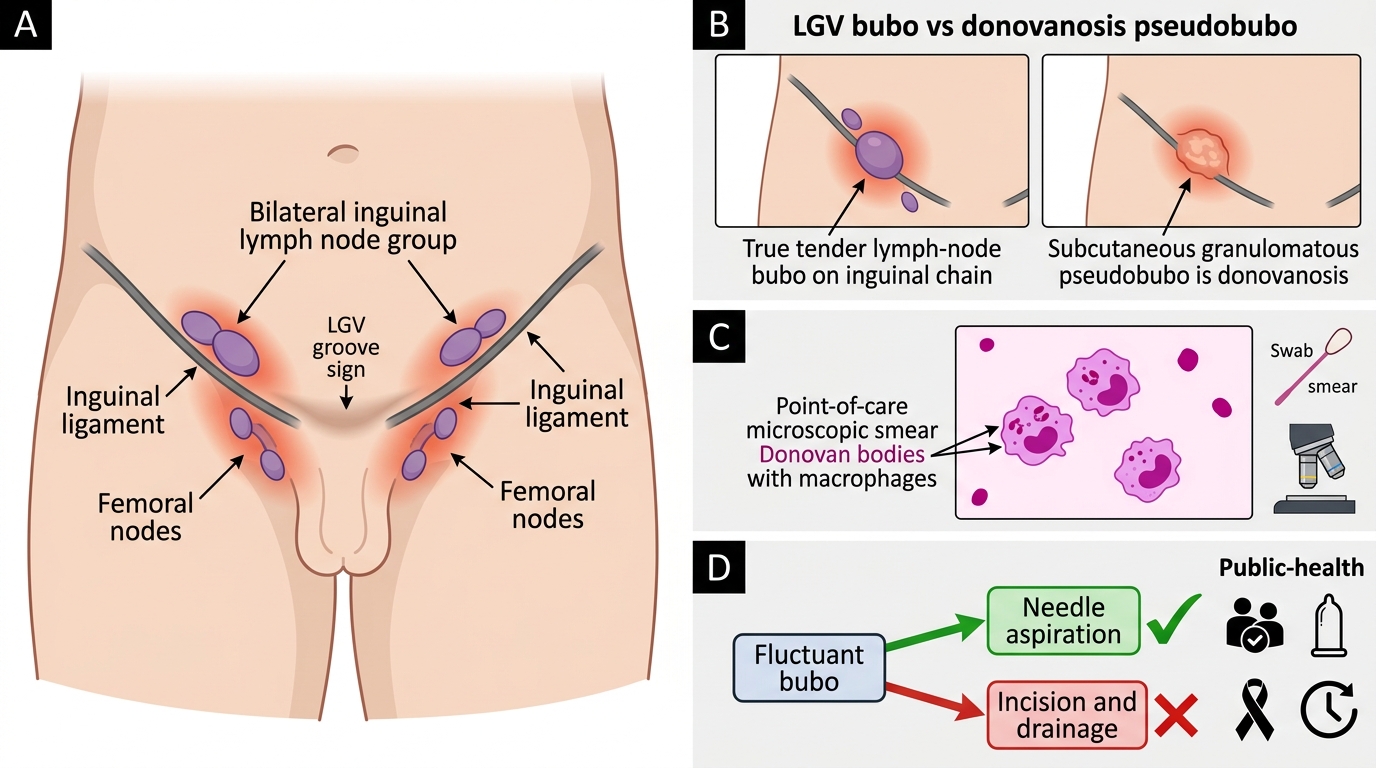
Because several conditions produce inguinal swelling, a disciplined differential prevents both over- and under-treatment. Beyond LGV and donovanosis, consider chancroid (painful suppurative bubo with a preceding painful ulcer), primary syphilis (firm non-tender nodes with a painless chancre), pyogenic adenitis from a lower-limb infection, bubonic plague in endemic settings, and lymphoma when systemic features are present. Investigation strategy is shaped by the resource setting: a tissue crush smear stained with Giemsa for Donovan bodies is the most accessible confirmatory test for donovanosis at the point of care. LGV is confirmed serologically (complement-fixation titre, classically high, or microimmunofluorescence) or by nucleic-acid amplification testing where available, but these are often unavailable in primary care. The operating principle of syndromic management is therefore to treat at first contact based on the clinical picture rather than waiting for confirmation, while sending available samples and offering HIV testing.
Inguinal Lymphadenopathy in Sexually Transmitted Diseases
Investigation pointers:
- Donovanosis: tissue crush smear (Giemsa) for Donovan bodies — point-of-care
- LGV: serology (complement fixation/microimmunofluorescence) or NAAT where available
- Syndromic principle: treat at first contact, do not await confirmation; offer HIV testing
SELF-CHECK
On examining a fluctuant inguinal bubo, what is the correct procedural step, and why?
A. Incise and drain widely to evacuate all the pus, as for any abscess
B. Aspirate the pus through intact adjacent healthy skin, because incision risks chronic non-healing sinuses
C. Leave it strictly alone and never touch it under any circumstance
D. Apply a tight pressure bandage to force spontaneous resolution
Reveal Answer
Answer: B. Aspirate the pus through intact adjacent healthy skin, because incision risks chronic non-healing sinuses
A fluctuant bubo should be aspirated (through adjacent healthy skin), not incised. Incision and drainage of a bubo tends to produce chronic, non-healing sinuses and delays recovery. Aspiration relieves the collection while avoiding that complication. Definitive treatment is the appropriate antibiotic regimen alongside aspiration as needed.
Syndromic Management With NACO Kit 6
NACO Kit 6 for Inguinal Bubo
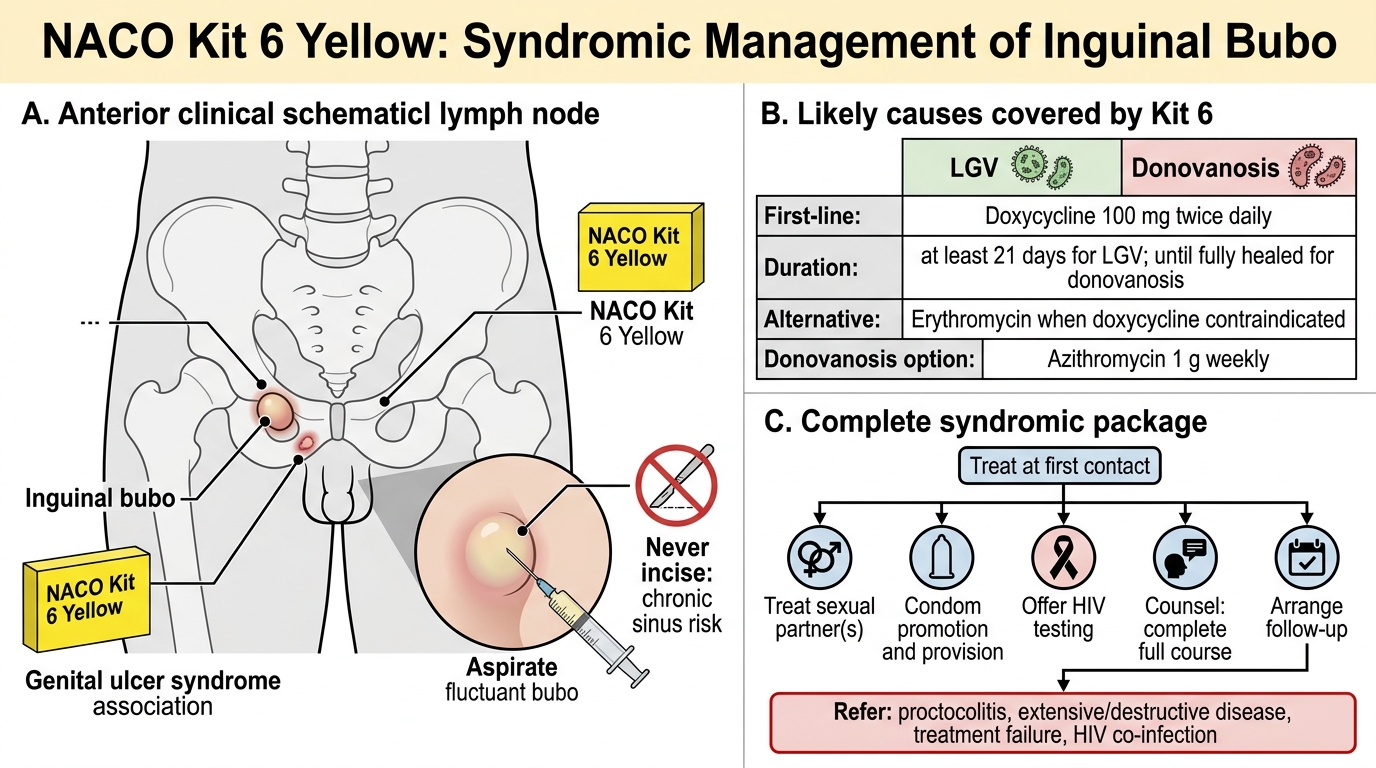
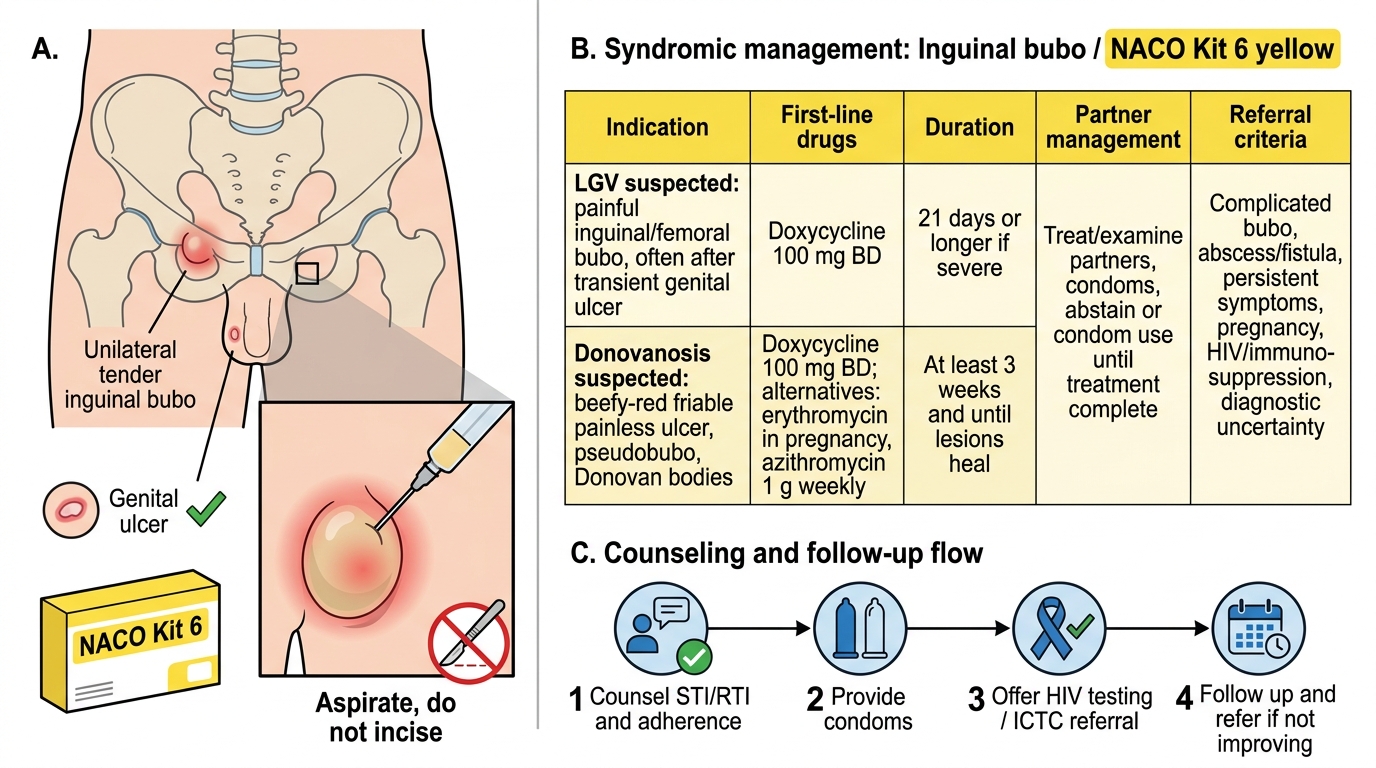
Syndromic management of the inguinal bubo means treating the syndrome reliably at first contact, and under the NACO programme this corresponds to Kit 6 (yellow) — per current NACO guidance, with the exact drugs and durations to be confirmed against the latest national protocol. The mainstay drug is doxycycline 100 mg twice daily, given for at least 21 days in LGV and continued for donovanosis until the lesions have fully healed (often three weeks or longer); erythromycin is the standard alternative where doxycycline is contraindicated (for example in pregnancy), and azithromycin (1 g weekly) is an accepted alternative specifically for donovanosis. A fluctuant bubo is aspirated, never incised, to avoid chronic sinus formation. Beyond drugs, syndromic management is incomplete without the public-health package: treat the sexual partner(s), promote and provide condoms, offer HIV testing, counsel on completing the full course, and arrange follow-up. Refer patients with proctocolitis, extensive or destructive disease, treatment failure, or HIV co-infection.
NACO Kit 6 Yellow: Syndromic Management of Inguinal Bubo
Management essentials:
- NACO Kit 6 (yellow); first-line doxycycline 100 mg BD (LGV ≥21 days; donovanosis until healed)
- Erythromycin alternative (e.g. pregnancy); azithromycin 1 g weekly an alternative for donovanosis
- Aspirate — do not incise — a fluctuant bubo
- Treat partner(s), provide condoms, offer HIV testing, counsel, follow up, refer when complicated
SELF-CHECK
A 30-year-old man has a beefy-red, friable genital ulcer that bleeds on touch and is painless, with a subcutaneous groin swelling. A tissue crush smear shows intracellular organisms within macrophages. What is the diagnosis and a key management principle?
A. LGV — give a single dose of azithromycin and discharge
B. Donovanosis — Donovan bodies confirm it; treat with prolonged doxycycline until lesions heal, treat the partner, and offer HIV testing
C. Chancroid — incise the pseudobubo immediately
D. Primary syphilis — a single dose of benzathine penicillin is curative and no follow-up is needed
Reveal Answer
Answer: B. Donovanosis — Donovan bodies confirm it; treat with prolonged doxycycline until lesions heal, treat the partner, and offer HIV testing
A beefy-red friable ulcer with a pseudobubo and intracellular Donovan bodies on tissue smear is donovanosis (Klebsiella granulomatis). Treatment is prolonged doxycycline (continued until lesions heal; azithromycin weekly is an alternative), with partner treatment and HIV testing as part of syndromic care. A pseudobubo is not incised.
Self-Assessment: Inguinal Bubo Recognition and Management
Inguinal Bubo Recognition and Management
Test your own grasp of this syndrome before moving on, because the value of recognising an inguinal bubo lies entirely in pairing the right diagnosis with the right action. Work through the questions below as if a patient were in front of you, articulating not just the answer but the reasoning — which organism, which sign, which kit, and which procedural rule. Pay particular attention to the two traps that catch learners most often: confusing the LGV groove sign with the donovanosis pseudobubo, and reflexively incising a fluctuant bubo that should be aspirated. If any item feels uncertain, return to the relevant section and rehearse the distinction until it is automatic, because under clinical pressure you will default to whatever you have practised most thoroughly. Treat each gap as a cue for focused revision rather than a verdict on your ability.
Self-check questions:
- What is the groove sign, and which condition does it indicate?
- How do the bubo of LGV and the pseudobubo of donovanosis differ?
- What confirms donovanosis at the point of care?
- What is the first-line Kit 6 drug, and how long is it given in LGV versus donovanosis?
- Why is a fluctuant bubo aspirated rather than incised?
- What public-health steps complete syndromic management (partner, condoms, HIV testing, follow-up)?
CLINICAL PEARL
The groove sign is memorable but not universal — it appears in only a minority of LGV cases, so its absence never rules LGV out. Conversely, the 'bubo' of donovanosis is usually a pseudobubo (subcutaneous granuloma), not a true lymph node, which is why a tissue smear for Donovan bodies — not a node biopsy — is your point-of-care confirmatory test. And whichever you treat, remember the deceptively simple rule that distinguishes good from harmful care: aspirate a fluctuant bubo, never incise it, because incision converts a treatable swelling into a chronic discharging sinus.