Page 14 of 35
DR10.3 | Non-Syphilitic Genital Ulcer Differential Diagnosis — SDL Guide (Part 2)
Diagnostic Tests — Gram Stain, Tzanck Smear, PCR, and Serological Interpretation
Diagnostic Tests in Genital Ulcer Disease
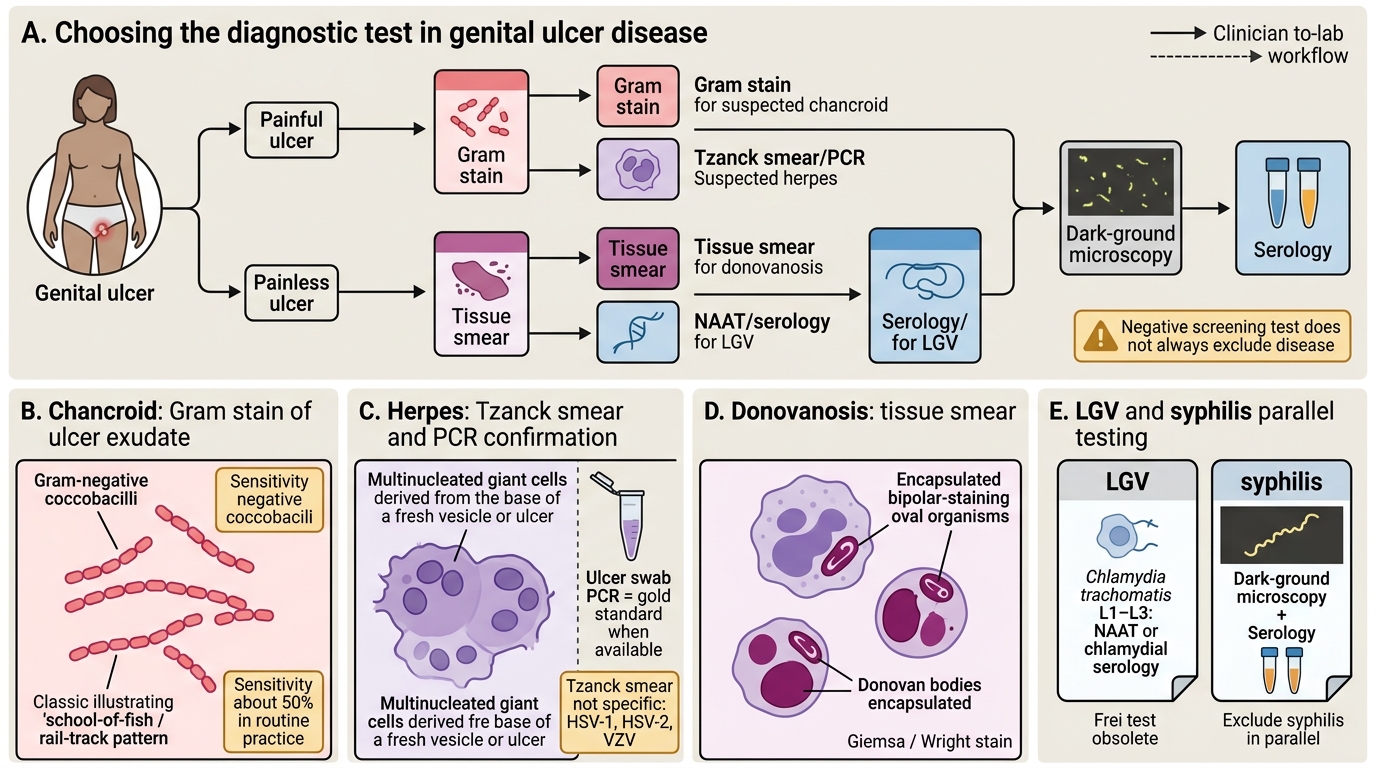
Confirming the cause means matching the right test to the suspected organism, while knowing the limits of each. For chancroid, a Gram stain of ulcer exudate may show Gram-negative coccobacilli arranged in parallel chains — the classic "school-of-fish" or "rail-track" pattern — but its sensitivity in routine clinical practice is only about 50%, so a negative Gram stain does not exclude chancroid, and definitive culture of H. ducreyi is technically demanding and rarely available. For herpes, a Tzanck smear from the base of a fresh lesion shows multinucleated giant cells; this is a useful, quick bedside test but it is not specific for HSV-2 — it is also positive in HSV-1 and varicella-zoster infection — so PCR of an ulcer swab is the gold standard when available, with viral culture and type-specific serology as alternatives. For donovanosis, a tissue smear or crush preparation stained with Giemsa or Wright stain reveals Donovan bodies — bipolar-staining, encapsulated organisms within the cytoplasm of large mononuclear cells. For LGV, the historical Frei intradermal test is obsolete and diagnosis now rests on chlamydial serology or nucleic acid testing. Throughout, syphilis must be excluded in parallel with dark-ground microscopy and serology, because co-infection occurs.
In practice these tests refine a diagnosis that the painful-versus-painless framework has already roughed out, and they feed the NACO syndromic algorithm: a herpetic ulcer (grouped vesicles, recurrence, multinucleated giant cells on Tzanck) is treated with the antiviral Kit 4 (blue), while a non-herpetic ulcer (syphilis or chancroid) is treated with the antibacterial Kit 3 (white) — per current NACO guidance, since kit contents are periodically revised.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
Comparison of Genital Ulcer Disease Causes
- Chancroid: Gram stain (school-of-fish Gram-negative coccobacilli, sensitivity ~50%); culture difficult.
- Herpes: Tzanck smear (multinucleated giant cells — not HSV-specific); PCR is the gold standard.
- Donovanosis: Donovan bodies on Giemsa-stained tissue smear; LGV: chlamydial serology/NAAT (Frei test obsolete).
Principles of Treatment for Chancroid and Herpes Genitalis
Treatment Principles for Chancroid and Herpes Genitalis
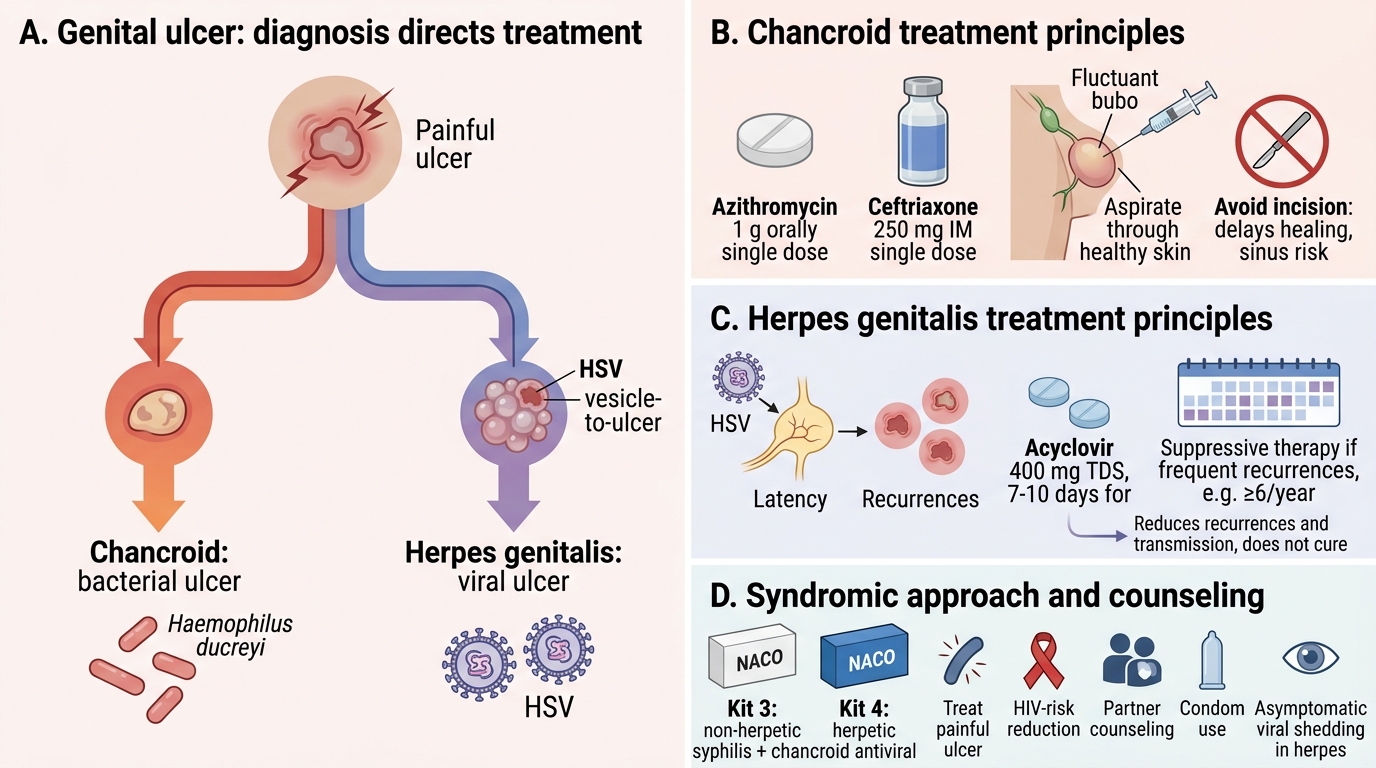
Treatment follows directly from the diagnosis, and the principles differ sharply between the bacterial and viral ulcers. Chancroid, being bacterial, responds to antibiotics: commonly a single dose of azithromycin 1 g orally or a single intramuscular dose of ceftriaxone 250 mg (other regimens such as ciprofloxacin or erythromycin are also used); a fluctuant bubo should be aspirated through adjacent healthy skin rather than incised, because incision delays healing and can create a sinus. Herpes genitalis, being viral, is not cured but controlled with antivirals: a primary episode is treated with acyclovir 400 mg three times daily for 7–10 days (or equivalent valacyclovir/famciclovir regimens), recurrences with shorter courses, and patients with frequent recurrences (often taken as around six or more episodes per year) may be offered suppressive therapy (for example daily acyclovir or valacyclovir) to reduce frequency and transmission. Always treat the painful ulcer for HIV-risk reduction and counsel on transmission, including asymptomatic viral shedding in herpes.
In the syndromic setting these specifics are delivered through the NACO kits: a herpetic ulcer is treated with the antiviral Kit 4 (blue), and a non-herpetic ulcer (covering both syphilis and chancroid) with the antibacterial Kit 3 (white) — the same syndromic logic that lets you treat effectively at the first visit, per current NACO guidance. Where laboratory confirmation is available it refines therapy and enables partner tracing and HIV testing, which accompany every genital ulcer consultation.
- Chancroid: single-dose azithromycin 1 g or ceftriaxone 250 mg IM; aspirate (do not incise) a fluctuant bubo.
- Herpes: acyclovir 400 mg TDS × 7–10 days for primary episodes; suppressive therapy for frequent recurrences.
- Syndromically: herpetic → Kit 4 (blue, antiviral); non-herpetic → Kit 3 (white, antibacterial), per current NACO guidance.
SELF-CHECK
A Tzanck smear taken from the base of a fresh genital ulcer shows multinucleated giant cells. What is the correct interpretation?
A. This is diagnostic of and specific for HSV-2 infection only
B. It indicates a herpesvirus infection (consistent with HSV-1, HSV-2, or varicella-zoster) — supportive but NOT specific for HSV-2; PCR is the gold standard for confirmation and typing
C. It is diagnostic of chancroid
D. It indicates donovanosis because the cells contain Donovan bodies
Reveal Answer
Answer: B. It indicates a herpesvirus infection (consistent with HSV-1, HSV-2, or varicella-zoster) — supportive but NOT specific for HSV-2; PCR is the gold standard for confirmation and typing
Multinucleated giant cells on a Tzanck smear indicate a herpesvirus infection but are not specific for HSV-2 — HSV-1 and varicella-zoster give the same finding. The Tzanck smear is a useful rapid bedside test, but PCR of an ulcer swab is the gold standard for confirmation and HSV typing. Donovan bodies (donovanosis) are a different finding seen on Giemsa-stained tissue smears.
Self-Assessment — GUD Differential Diagnosis Cases
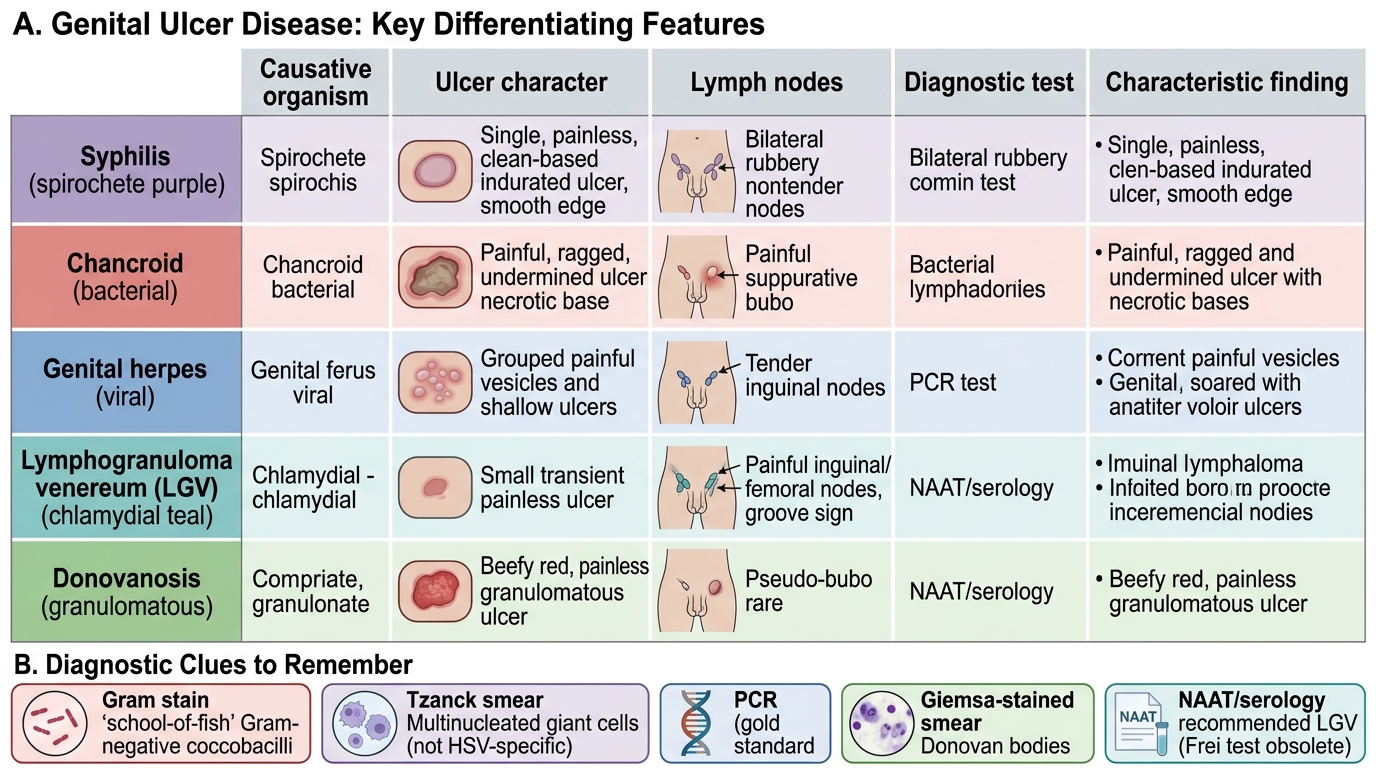
Consolidate the differential by working scenarios and, in each, stating the discriminating feature and the confirmatory test. First, anchor everything on the painful-versus-painless triage: a painful, soft, ragged ulcer with a tender suppurative bubo is chancroid; painful grouped vesicles that recur are herpes; a painless indurated clean-based ulcer is the syphilitic chancre; a painless, beefy-red, friable ulcer without true nodes is donovanosis; and a transient painless ulcer followed by matted groove-sign nodes is LGV. Second, match the test to the suspicion: a Gram stain showing school-of-fish Gram-negative coccobacilli supports chancroid (but is only ~50% sensitive); multinucleated giant cells on a Tzanck smear support herpes (but are not HSV-specific — PCR confirms); Donovan bodies on a Giemsa tissue smear confirm donovanosis. Third, link to treatment and the syndromic kits: bacterial ulcers (chancroid, syphilis) to antibacterial therapy / Kit 3, herpes to antivirals / Kit 4 — always with HIV testing and partner management.
For each self-check question, reason from the framework rather than memorising answers: if you can name the discriminating clinical feature, the confirmatory test and its limitation, and the correct treatment, you have mastered the genital ulcer differential.
- Triage by pain, then morphology, nodes, and recurrence.
- Match test to suspicion and know each test's limitation (Gram stain ~50%; Tzanck not HSV-specific).
- Treat by mechanism (antibacterial vs antiviral) and deliver syndromically (Kit 3 vs Kit 4) with HIV testing and partner care.
SELF-CHECK
A patient has a slowly enlarging, painless, beefy-red, friable genital ulcer that bleeds easily on contact, with no significant inguinal lymphadenopathy. A tissue smear stained with Giemsa shows bipolar-staining intracytoplasmic organisms. What is the diagnosis?
A. Chancroid
B. Donovanosis (granuloma inguinale)
C. Primary syphilis
D. Herpes genitalis
Reveal Answer
Answer: B. Donovanosis (granuloma inguinale)
A painless, beefy-red, friable ulcer that bleeds easily, without true lymphadenopathy, plus Donovan bodies (bipolar-staining, encapsulated intracytoplasmic organisms) on a Giemsa-stained tissue smear, is diagnostic of donovanosis (granuloma inguinale), caused by Klebsiella granulomatis. The painlessness and absence of true nodes distinguish it from chancroid; Donovan bodies are the confirmatory finding.
CLINICAL PEARL
When a genital ulcer hurts, think herpes and chancroid; when it does not, think syphilis (and donovanosis and LGV). Then let the texture decide between the painful pair: chancroid is soft and ragged, herpes is vesicular and grouped — and recurrence clinches herpes. Remember the two test traps that examiners love: the chancroid Gram stain is only about 50% sensitive, so a negative result does not exclude it; and the herpes Tzanck smear shows multinucleated giant cells that are not specific for HSV-2 (HSV-1 and varicella give them too), so PCR is the gold standard for confirmation and typing.