Page 5 of 35
DR10.5 | Sexual History Safe Behaviour Counselling and HIV Pretest Counselling — SDL Guide (Part 2)
Interpreting Risk Level and Tailoring Risk-Reduction Advice
Risk Stratification and Tailored STI Counselling
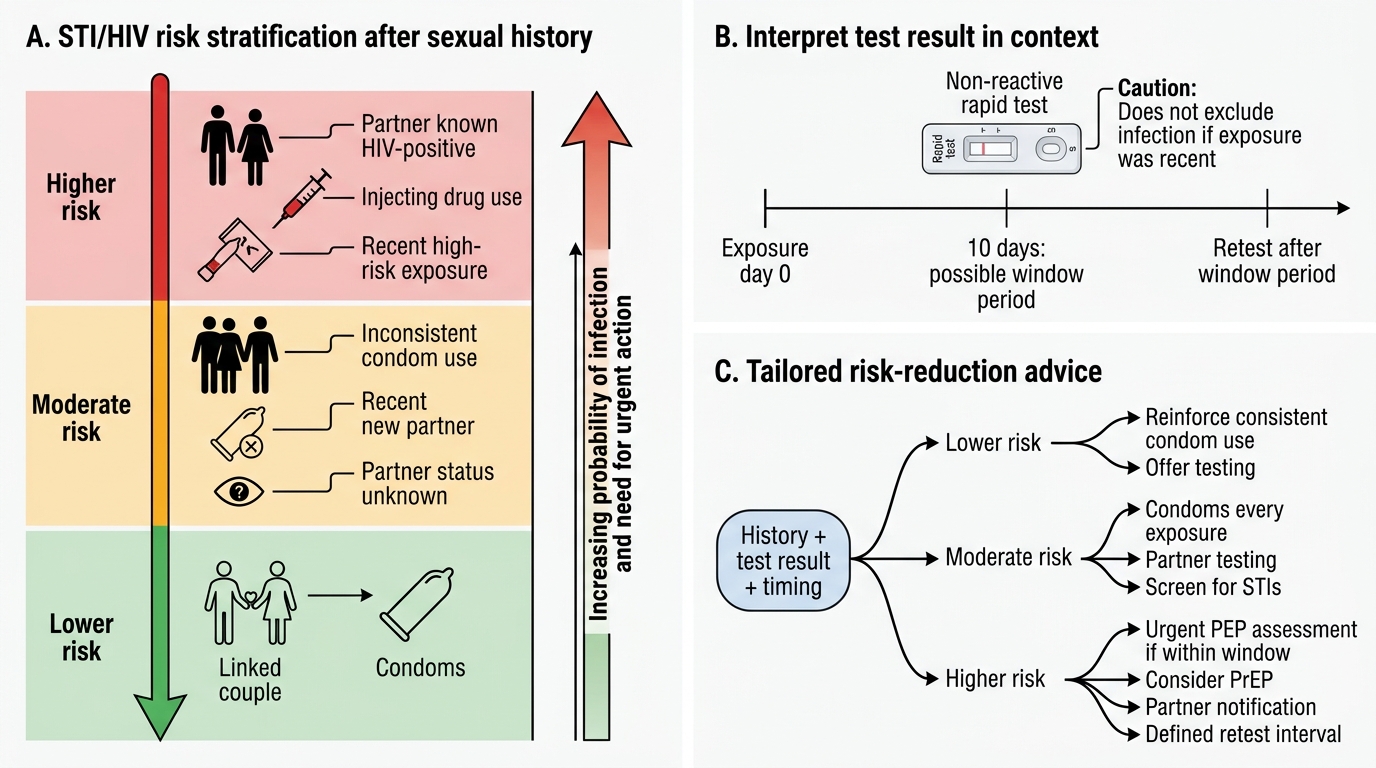
Once you have the history, you must interpret it to stratify risk and tailor advice, because generic advice is far less effective than advice matched to the patient's actual exposures. Broadly, you can think in terms of lower, moderate, and higher risk: a single mutually monogamous partnership with consistent condom use sits at the lower end; multiple partners, inconsistent or no condom use, a partner of unknown status, or a recent new partner pushes risk higher; and exposures such as a partner known to be HIV-positive, injecting drug use, or a recent high-risk exposure sit higher still and may trigger discussion of post-exposure or pre-exposure prophylaxis and a defined re-test interval. The point of stratifying is to make the counselling specific: for a higher-risk patient you emphasise consistent condom use, partner testing and notification, and a clear plan to re-test after the window period; for a lower-risk patient you reinforce what is working while still offering testing.
Interpreting the test result in context is part of the same skill. A non-reactive rapid test in a patient who had a high-risk exposure only ten days ago does not exclude infection, because the patient may still be within the window period — so you counsel re-testing. A reactive screening result requires the established confirmatory pathway and careful, supportive post-test counselling. Effective risk-reduction messages are concrete and behavioural — often summarised for patients as the ABC approach (Abstinence, Be faithful, correct and consistent Condom use) — adapted to the individual rather than recited as a slogan.
- Stratify risk (lower / moderate / higher) from the history and tailor advice accordingly.
- A non-reactive result within the window period does not exclude infection — counsel re-testing.
- Make risk-reduction messages concrete and behavioural (e.g. the ABC approach), individualised to the patient.
Applied Practice — Case-Based Sexual Health Counselling
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Case-Based Sexual Health Counselling Workflow
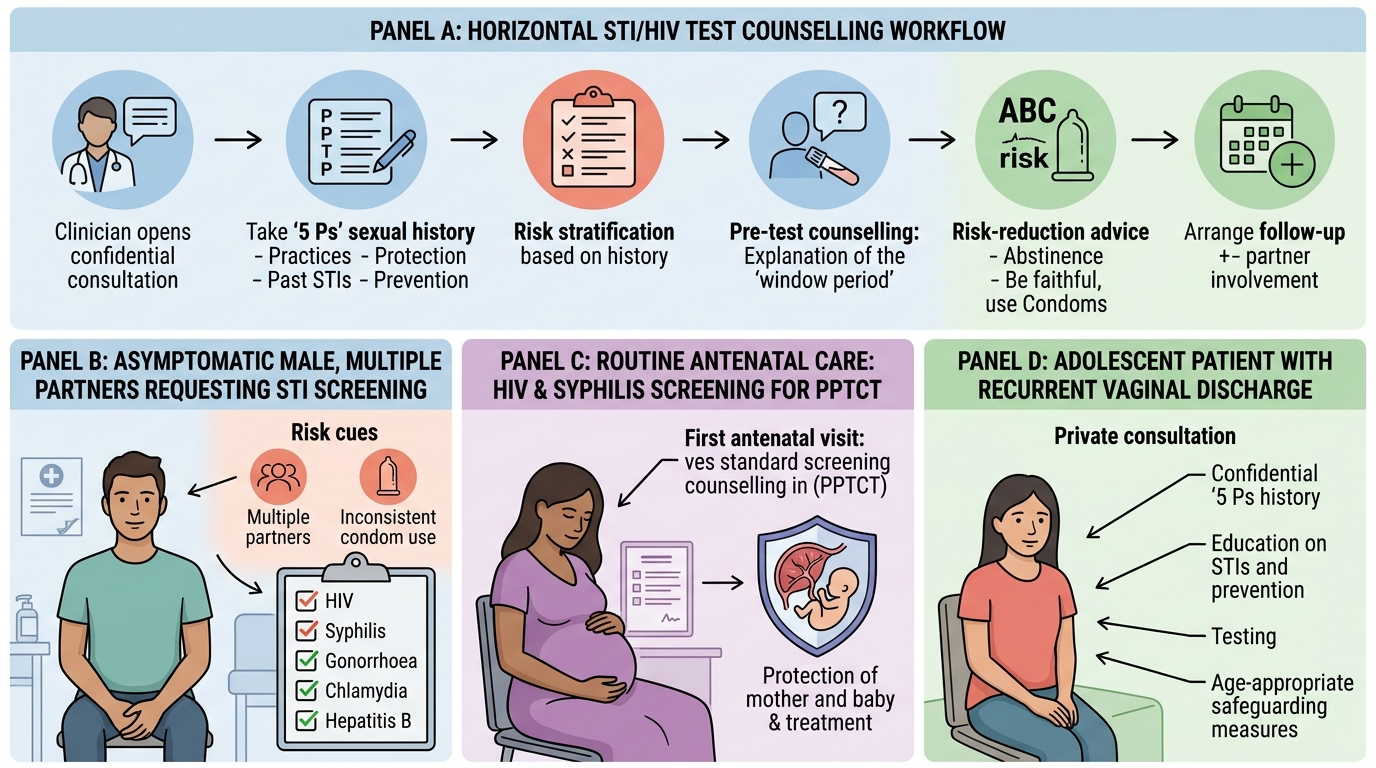
Applying the skill means rehearsing it on realistic cases until the structure becomes second nature. Consider a young man who requests STI testing and, on the 5 Ps, reports several recent partners and inconsistent condom use: here you assess him as higher risk, offer comprehensive screening including HIV with proper pre-test counselling, explain the window period for the test your centre uses, and agree a re-test plan and concrete condom-use advice. Consider a woman at her first antenatal visit: routine HIV screening under the prevention-of-parent-to-child-transmission programme is offered with pre-test counselling, because identifying and treating maternal HIV (and syphilis) protects the baby — and the counselling here is framed around the benefit of treatment for both mother and child. Consider an adolescent with recurrent vaginal discharge: a gentle, confidential 5 Ps history may reveal an unprotected new relationship, and the consultation becomes an opportunity for education, testing, and safeguarding consideration appropriate to age.
Across all three, the same moves recur: open safely, take the 5 Ps, stratify risk, counsel before testing with a clear window-period explanation, deliver individualised risk-reduction advice (the ABC messages adapted to the person), and arrange follow-up and partner involvement. Rehearsing aloud — ideally in role-play — is what converts the framework into fluent, humane practice.
- Higher-risk patient: comprehensive screening + pre-test counselling + re-test plan + condom advice.
- Antenatal patient: routine PPTCT HIV (and syphilis) screening framed around benefit to mother and baby.
- Adolescent: confidential, age-appropriate history with education, testing, and safeguarding awareness.
SELF-CHECK
A patient had a single high-risk unprotected exposure 10 days ago and now has a non-reactive HIV rapid test. Using a fourth-generation antigen/antibody combination assay, what is the correct counselling?
A. The non-reactive result definitively excludes HIV infection; no further testing is needed
B. The result may be within the window period (roughly 10–33 days for a 4th-generation assay), so re-testing after the window is advised before HIV can be excluded
C. The patient must already have AIDS because the test is negative
D. The test should be ignored and treatment for HIV started immediately
Reveal Answer
Answer: B. The result may be within the window period (roughly 10–33 days for a 4th-generation assay), so re-testing after the window is advised before HIV can be excluded
A fourth-generation Ag/Ab combination assay detects infection earlier than antibody-only tests, but a window period of roughly 10–33 days still applies. A non-reactive result only 10 days after exposure cannot exclude infection, so the patient should be counselled to re-test after the window period. Always state the test generation, and verify the exact window against current NACO ICTC guidance.
Self-Assessment — Counselling Communication Scenarios
Use these self-checks to confirm you can both recall the framework and apply it in sensitive situations. First, be able to recite and explain the 5 Ps — Partners, Practices, Protection, Past STI history, Pregnancy intention — and what each one detects, because in an OSCE the marks come from systematically covering all five with non-judgmental, open-ended questions. Second, be precise about the window period: it is test-generation dependent, so a defensible answer names the test (a fourth-generation Ag/Ab assay turns positive earlier, roughly ten to thirty-three days; an antibody-only test may take up to about forty-five days) and notes that the local value should be confirmed against current ICTC guidance rather than quoted as a universal fact. Third, rehearse the ethics: confidentiality, voluntary consent, and the careful, supportive handling of a discordant couple's results, where one partner is reactive and the other non-reactive and your duty of confidentiality must be balanced with the public-health imperative to prevent transmission.
For each self-check question, state your reasoning. If you can explain why the window period matters, why consent must be voluntary, and why risk-reduction advice should be individualised rather than recited, you have learned a clinical skill rather than a list.
- Recall and apply the 5 Ps with non-judgmental, open-ended questions.
- Give a test-specific window-period answer and flag local verification.
- Handle confidentiality, consent, and discordant results with care.
CLINICAL PEARL
The single most powerful technique for taking a sexual history is normalising the questions: open with a line such as "I ask all my patients these questions so I can give you the best care — everything you tell me is confidential." This one sentence does more to elicit honest answers than any clever wording that follows, because it removes the patient's fear of being judged and signals that the enquiry is routine, not accusatory. Pair it with open-ended questions and the patient's own vocabulary, and even difficult histories open up.