Page 7 of 35
DR10.2 | Syphilis Diagnosis — SDL Guide
Learning Objectives
- Describe the clinical features of each stage of syphilis — primary, secondary, latent, and tertiary — and of congenital syphilis.
- Explain the immunopathogenesis of Treponema pallidum infection and how it produces the staged course.
- Distinguish non-treponemal (VDRL/RPR) from treponemal (TPHA/FTA-ABS/TPPA) serological tests and state the use of each.
- Select and interpret the appropriate diagnostic test for a given clinical presentation, including biological false positives.
- Relate diagnostic findings to staging so that treatment can be selected (covered fully in the treatment SDL).
INSTRUCTIONS
Syphilis is called the great imitator because it can mimic almost any disease, and it remains common in Indian STI clinics and antenatal screening. Diagnosing it correctly means recognising the stage from clinical features and then choosing — and interpreting — the right test, because no single test answers every question. This module builds that diagnostic logic from the bedside lesion to the serology report.
References
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, Ch. on Syphilis (textbook)
- IADVL Textbook of Dermatology, Ch. on Syphilis (textbook)
- NACO National Guidelines on Prevention, Management and Control of RTI/STI, Ministry of Health & Family Welfare, Government of India (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 30-year-old man notices a single, firm, painless sore on his penis. Because it does not hurt, he ignores it; within weeks it heals on its own, and he forgets it. Three months later he develops a faint rash on his palms and soles and a few grey patches in his mouth, again with no real discomfort. Each time, the very painlessness that reassures him is the clue that should alarm a clinician: a painless indurated ulcer followed by a palmoplantar rash is syphilis announcing itself in two of its classic stages. Recognising this staged, often painless story — and confirming it with the right tests — is the heart of diagnosing the great imitator.
WHY THIS MATTERS
Syphilis matters to you as a final-year student for three concrete reasons. It is common — screened for routinely in every antenatal clinic in India because untreated maternal syphilis devastates the fetus — so you will encounter positive serology and must know what it means. It is treatable and curable when diagnosed, but its complications (neurosyphilis, cardiovascular syphilis, congenital syphilis) are severe and largely preventable. And it is a diagnostic trap: a single serological test can mislead in both directions — a false positive in pregnancy or autoimmune disease, a false negative in the window period or in late disease — so you must understand which test answers which question. Getting the diagnosis right is what makes the (simple, cheap) treatment possible.
RECALL
Recall the foundations this builds on. From microbiology you know Treponema pallidum is a thin, motile spirochaete that cannot be grown on ordinary culture media and is visualised by dark-ground microscopy. From immunology you know that infection provokes both a specific antibody response (against treponemal antigens) and a non-specific antibody response (against a lipid, cardiolipin, released from damaged host cells) — a distinction that, as you will see, underlies the two families of serological tests. You also know from your STI reading that a genital ulcer can be painful or painless, and that the painless, indurated ulcer is the hallmark of primary syphilis, in contrast to the painful ulcers of chancroid and herpes.
The Chancre and Secondary Rash — Recognising Syphilis at the Bedside
Recognising Primary and Secondary Syphilis at the Bedside
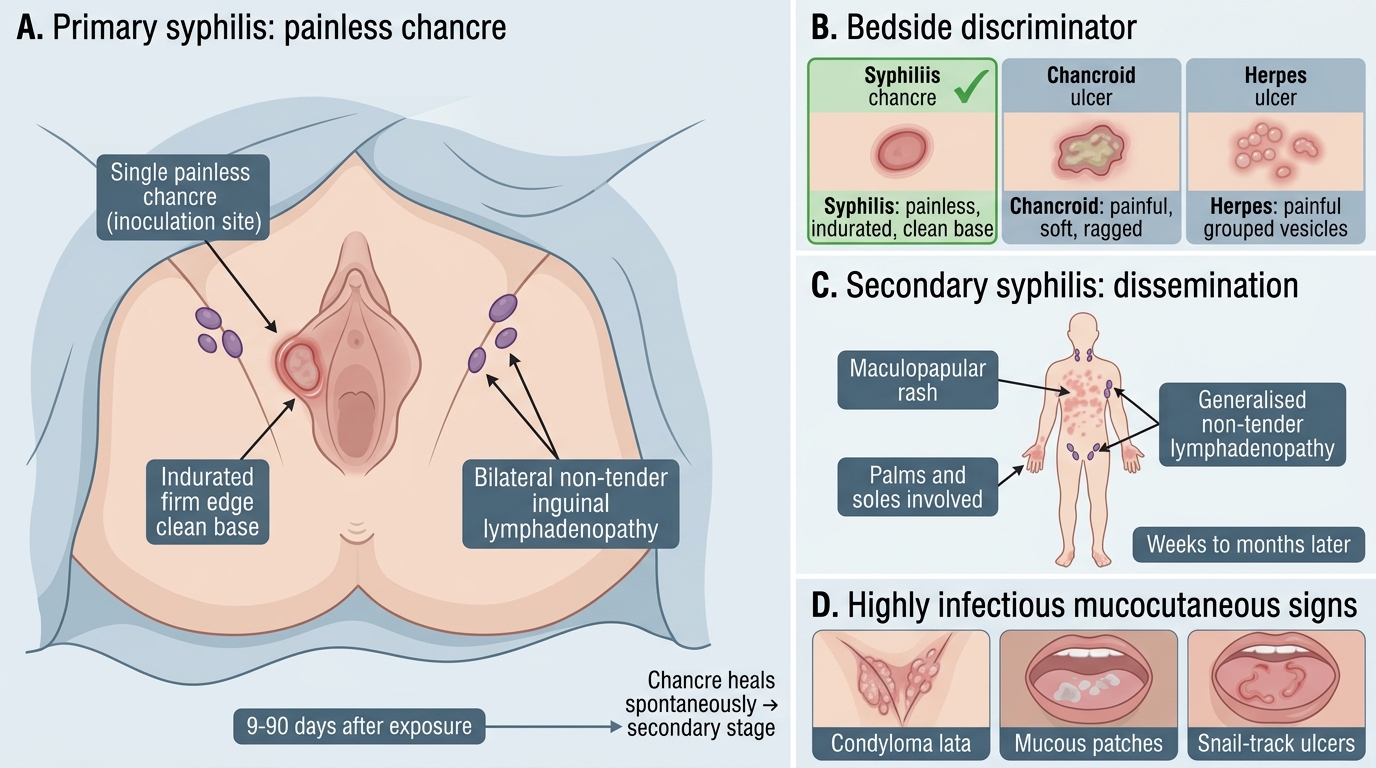
The diagnosis of syphilis begins with recognising its morphology at the bedside, because the clinical appearance often precedes — and guides — the laboratory. The lesion of primary syphilis is the chancre: a single, painless, indurated (firm-edged) ulcer with a clean base, appearing at the site of inoculation roughly nine to ninety days after exposure, and accompanied by non-tender, rubbery, bilateral inguinal lymphadenopathy. Its defining and counter-intuitive feature is that it does not hurt — painlessness is precisely what distinguishes the syphilitic chancre from the painful ulcers of chancroid and herpes, and it is the single most useful discriminator at the bedside. The chancre heals spontaneously over a few weeks even without treatment, which is why patients (and clinicians) miss it. Weeks to months later, secondary syphilis appears as the spirochaete disseminates: a characteristic maculopapular rash that classically involves the palms and soles, moist wart-like papules in warm intertriginous areas called condyloma lata, greyish mucous patches and "snail-track" ulcers in the mouth, and generalised non-tender lymphadenopathy. Secondary syphilis is highly infectious and, like the primary stage, tends to be more uncomfortable to look at than to feel.
Recognising this morphology drives the diagnostic next step. A painless indurated genital ulcer prompts dark-ground microscopy of its exudate and serology; a palmoplantar rash with mucous patches prompts serology for secondary syphilis. The bedside pattern, in other words, tells you which test to order and how to read it.
- Primary: single, painless, indurated chancre + non-tender bilateral inguinal nodes; heals spontaneously.
- Secondary: palmoplantar maculopapular rash, condyloma lata, mucous patches, generalised lymphadenopathy; highly infectious.
- The painlessness of the chancre is the key bedside discriminator from chancroid and herpes.
Treponema pallidum and the Immunopathogenesis of Disease Stages
Treponema pallidum: Staged Disease and Diagnostic Immunopathogenesis
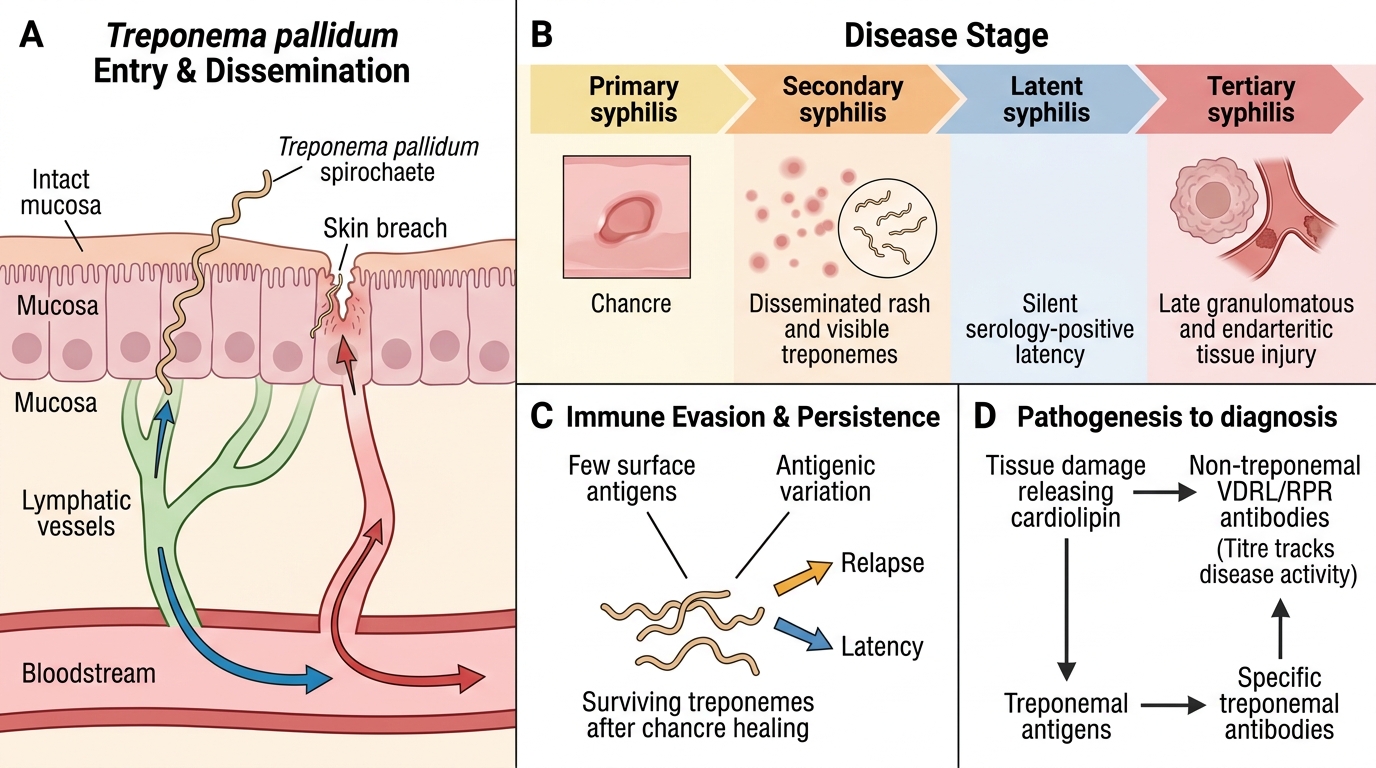
Understanding why syphilis unfolds in stages requires looking at the organism and the host response together. Treponema pallidum is a slender, motile spirochaete that is microaerophilic and cannot be cultured on artificial media; it invades through intact mucosa or minor breaks in skin and spreads early via the lymphatics and bloodstream, so that even the localised-looking primary chancre represents an already systemic infection. The host mounts an immune response that eventually clears the chancre, producing the apparent "resolution" of primary syphilis — but the organism is not eradicated, and surviving treponemes disseminate to cause the secondary stage. The spirochaete is remarkably good at evading immunity: it presents few surface antigens and varies them, which lets it persist and explains both the relapsing nature of early syphilis and the long, silent latent period that follows. During latency the infection is asymptomatic but serology remains positive; after years, in a minority of untreated patients, the chronic granulomatous and endarteritic damage of tertiary syphilis emerges.
This immunopathogenesis directly explains the diagnostic tests. Tissue damage releases host lipids (cardiolipin) that provoke a non-specific antibody — the basis of the non-treponemal VDRL and RPR tests, whose titre rises and falls with disease activity. The organism's own antigens provoke specific treponemal antibodies — the basis of the confirmatory TPHA, FTA-ABS, and TPPA tests, which, once positive, generally stay positive for life because they reflect ever having been infected rather than current activity.
- T. pallidum: uncultivable spirochaete, disseminates early via lymph/blood; primary syphilis is already systemic.
- Immune evasion (antigenic variation) explains latency and the staged, relapsing course.
- Tissue damage → cardiolipin → non-treponemal antibodies; organism antigens → treponemal antibodies — the two test families.
Clinical Staging of Syphilis — Primary Through Tertiary and Congenital
Clinical Staging of Syphilis
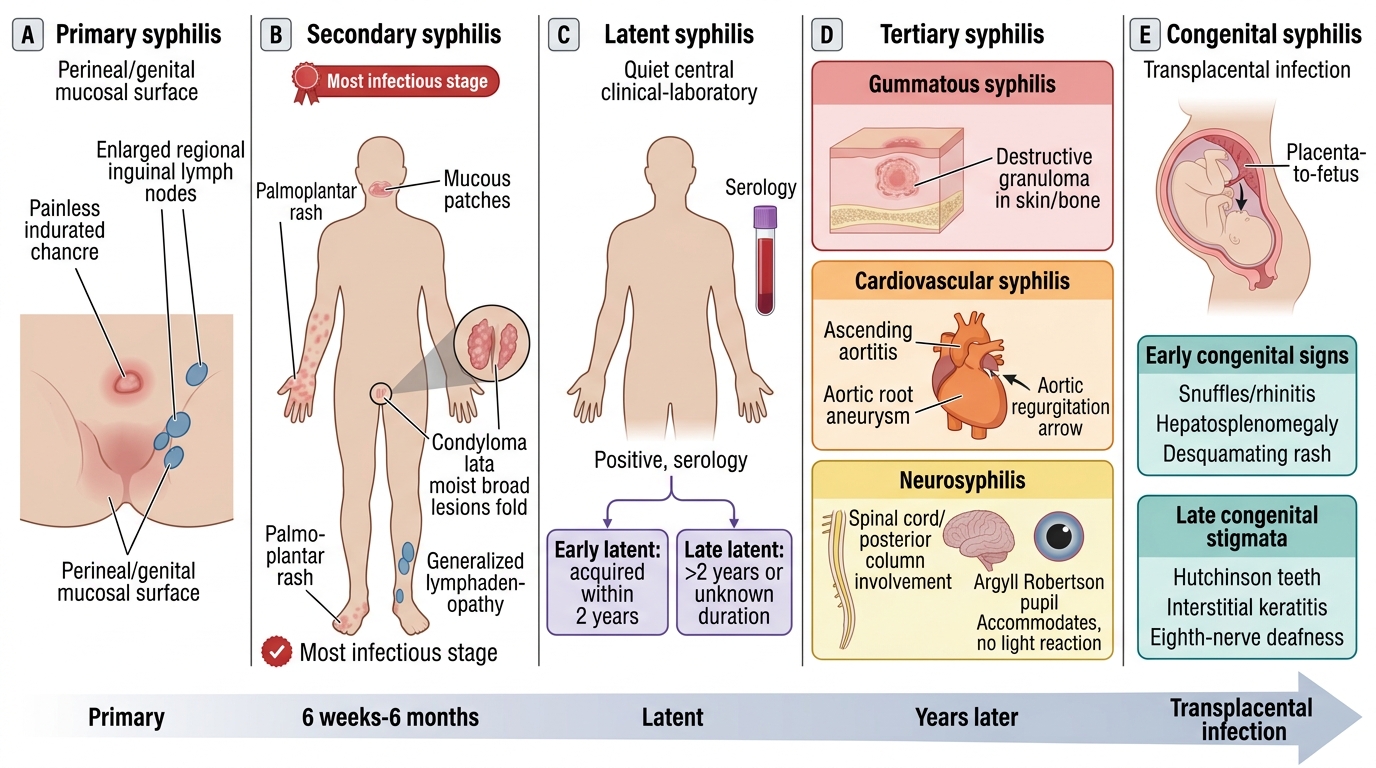
Staging syphilis precisely is essential because the stage determines both the diagnostic interpretation and the treatment. Primary syphilis is the chancre with regional lymphadenopathy. Secondary syphilis, six weeks to six months later, is the disseminated stage — palmoplantar rash, condyloma lata, mucous patches, generalised lymphadenopathy, sometimes with constitutional symptoms — and is the most infectious stage. After secondary features resolve, the patient enters latent syphilis, defined by positive serology without clinical signs; this is divided by duration into early latent (acquired within the preceding two years, still potentially infectious and capable of relapse) and late latent (more than two years or of unknown duration, with a lower infectivity) — a distinction that matters because it changes the treatment regimen. Tertiary syphilis, developing years later in a minority of untreated patients, comprises gummata (destructive granulomas in skin, bone, or viscera), cardiovascular syphilis (aortitis with aortic root aneurysm and aortic regurgitation), and neurosyphilis (tabes dorsalis, general paresis, and the Argyll Robertson pupil that accommodates but does not react to light). Congenital syphilis, from transplacental infection, produces early signs (rhinitis/snuffles, hepatosplenomegaly, a desquamating rash) and late stigmata (Hutchinson's teeth, interstitial keratitis, eighth-nerve deafness — Hutchinson's triad — plus saddle nose and Wimberger's sign on radiology).
Knowing where a patient sits on this spectrum is what lets you order and interpret the right test and, ultimately, choose the right penicillin regimen.
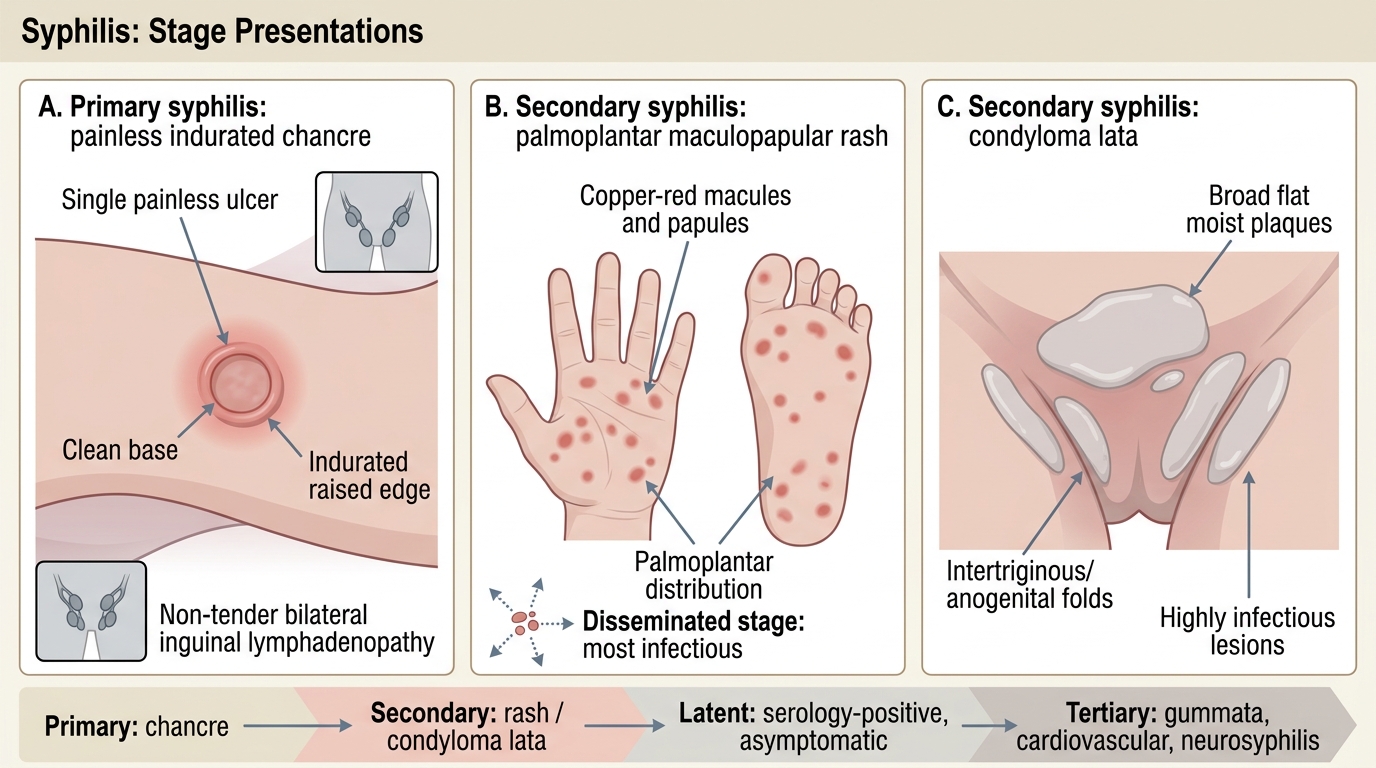
Syphilis Stage Presentations
- Primary = chancre; Secondary = disseminated (most infectious); Latent = serology-positive, asymptomatic (early <2 y vs late >2 y).
- Tertiary = gummata, cardiovascular, neurosyphilis (incl. Argyll Robertson pupil).
- Congenital = early signs (snuffles, hepatosplenomegaly) and late stigmata (Hutchinson's triad, saddle nose).
SELF-CHECK
Which clinical description correctly characterises the lesion of PRIMARY syphilis?
A. A painful, soft, ragged ulcer with a dirty base and a tender suppurative inguinal node
B. A single, painless, indurated ulcer with a clean base and non-tender bilateral inguinal lymphadenopathy
C. Grouped vesicles that rupture to form painful shallow ulcers
D. A beefy-red, friable, painless ulcer with no lymphadenopathy
Reveal Answer
Answer: B. A single, painless, indurated ulcer with a clean base and non-tender bilateral inguinal lymphadenopathy
The primary chancre is a single, painless, indurated ulcer with a clean base and non-tender bilateral inguinal lymphadenopathy. Its painlessness distinguishes it from chancroid (painful, soft, ragged, tender bubo) and herpes (painful grouped vesicles). The beefy-red friable ulcer describes donovanosis.