Page 11 of 35
DR10.6 | Syphilis Treatment Workflow — SDL Guide (Part 2)
Genital Ulcer Disease — Syndromic Management and Stage Integration
Genital Ulcer Disease: Syndromic Management and Stage Integration
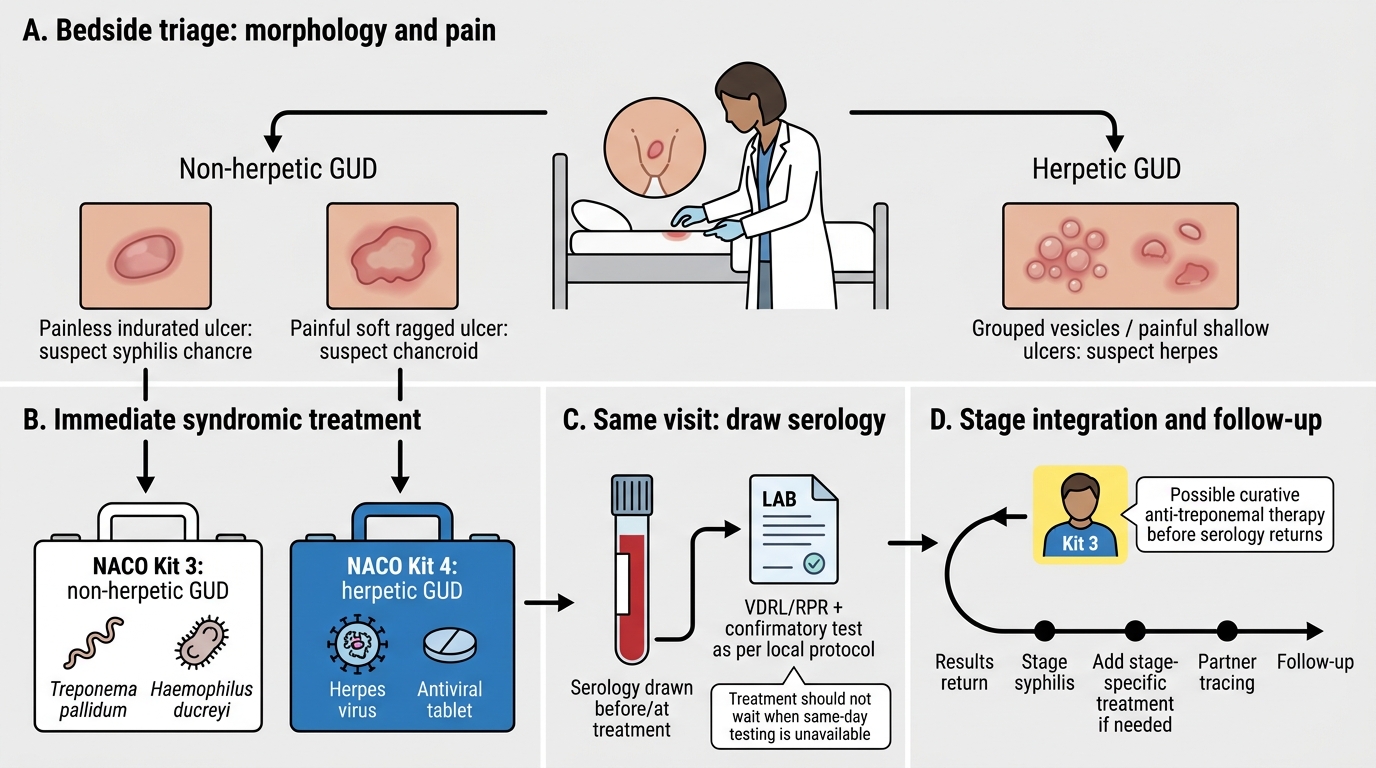
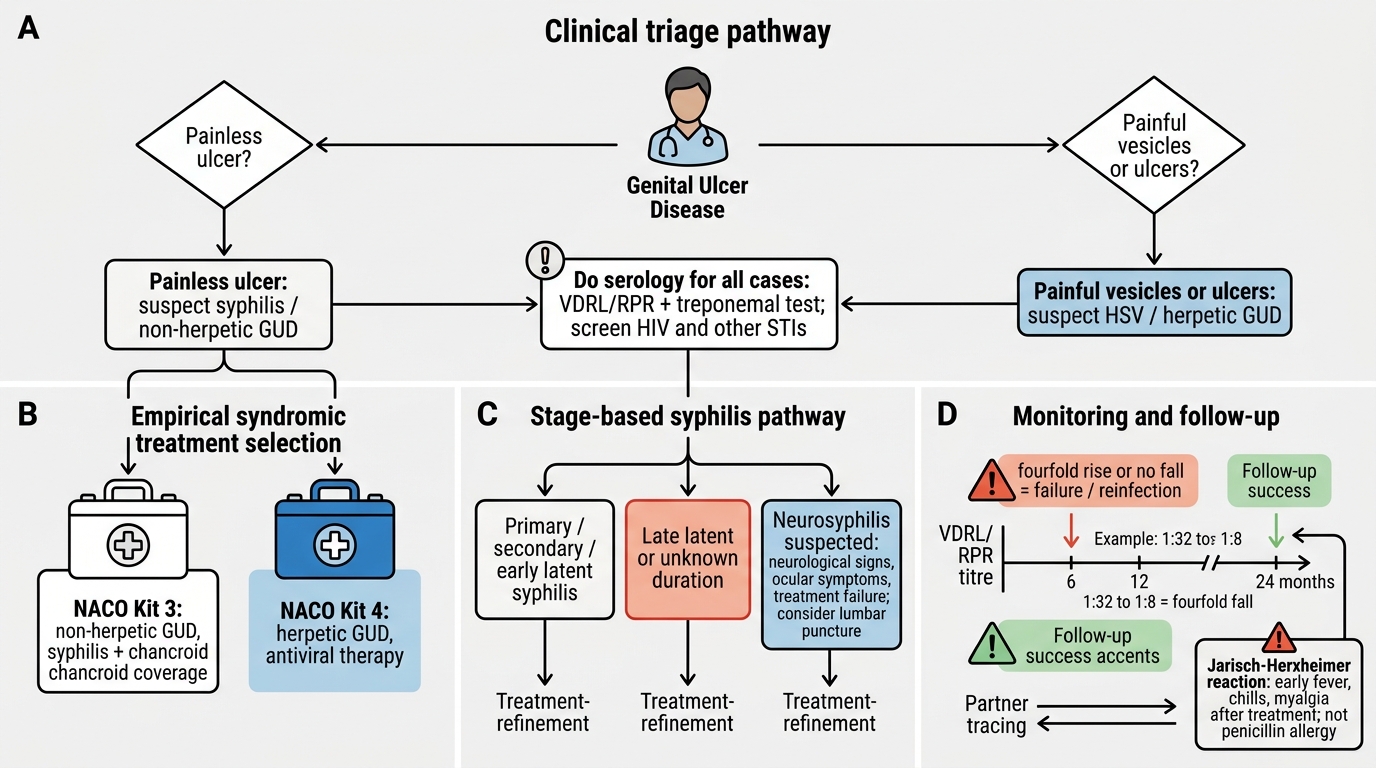
In practice, many patients present not with a confirmed serological diagnosis but with a genital ulcer at a clinic where same-day testing is unavailable, so syphilis treatment must integrate with the NACO syndromic approach to genital ulcer disease. The first triage at the bedside is morphology and pain: a painless indurated ulcer (syphilis) or a painful, soft, ragged ulcer (chancroid) places the patient in the non-herpetic GUD group, whereas grouped vesicles and painful shallow ulcers (herpes) place them in the herpetic group. The non-herpetic group is treated empirically with NACO Kit 3 (white), which is designed to cover both syphilis and chancroid simultaneously — exactly the syndromic principle of treating all the probable bacterial causes of the syndrome at once (per current NACO guidance, since kit contents are revised periodically). The herpetic group is treated with the antiviral Kit 4 (blue). This means that a patient with a syphilitic chancre may receive curative anti-treponemal therapy through Kit 3 at the very first visit, before serology even returns.
Integration with staging then follows: serology should still be drawn so that, once results return, the patient can be staged and given any additional stage-specific treatment needed, and so that partners can be traced and follow-up arranged. The syndromic kit gets effective treatment into the patient immediately; the serological work-up refines staging and monitoring afterwards. When facilities allow, definitive diagnosis is preferred, but it should never delay treating a clinically obvious ulcer.
Genital Ulcer Disease: Triage, Kit Selection, and Follow-up
- Non-herpetic GUD (syphilis + chancroid) → NACO Kit 3 (white) empirically, per current NACO guidance.
- Herpetic GUD (HSV) → Kit 4 (blue), antiviral.
- Draw serology anyway to stage, monitor, trace partners — the kit treats now, serology refines later.
Monitoring Treatment Response, Retreatment Criteria, and the Jarisch-Herxheimer Reaction
Syphilis Treatment Follow-Up and Jarisch-Herxheimer Reaction
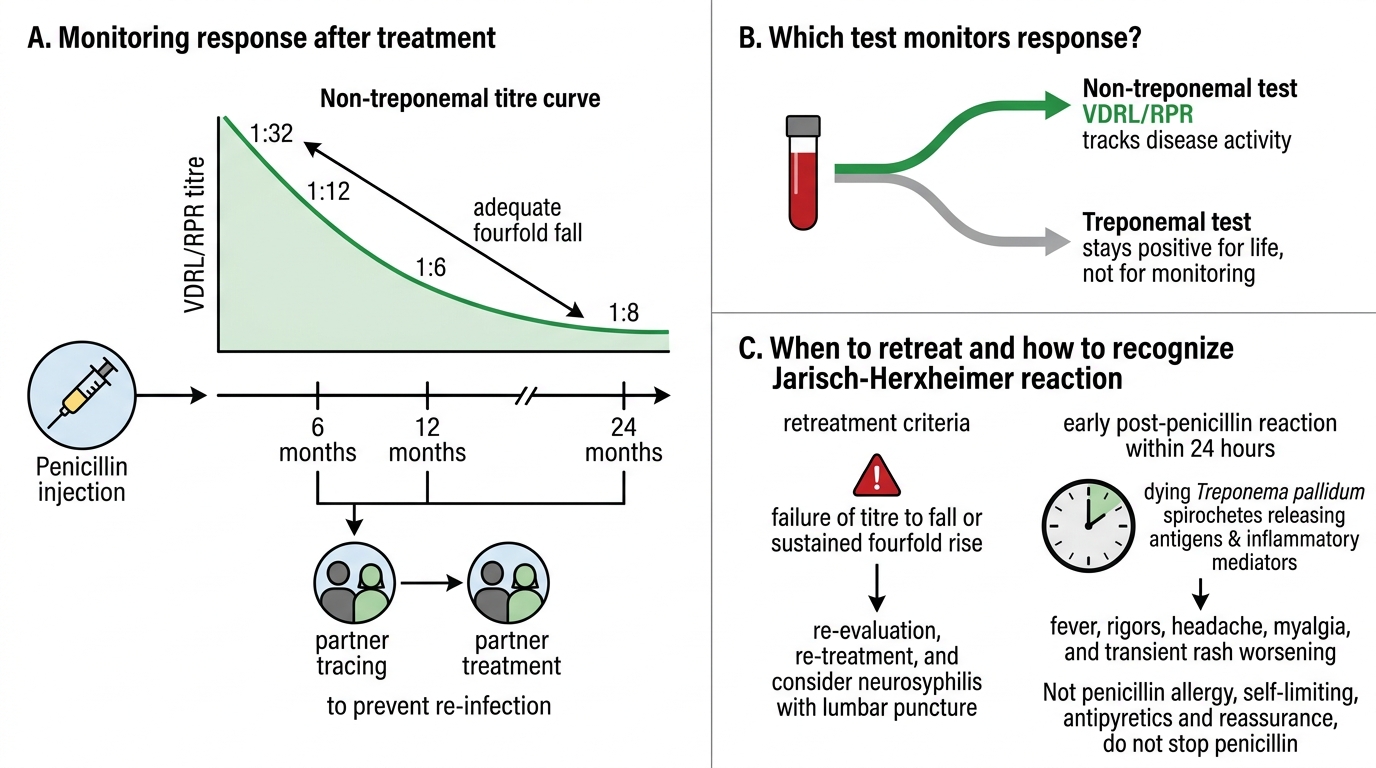
Treatment is not complete at the injection; you must monitor that it worked and manage its predictable early reaction. Monitoring uses the non-treponemal (VDRL/RPR) titre, checked at intervals (commonly around 6, 12, and 24 months): an adequate response is a fourfold (two-dilution) fall in titre — for example from 1:32 to 1:8 — within six to twelve months, reflecting resolving disease activity. Failure of the titre to fall, or a sustained fourfold rise, indicates treatment failure or re-infection and prompts re-evaluation, re-treatment, and consideration of neurosyphilis (with a lumbar puncture). Remember that treponemal tests stay positive for life and so are useless for monitoring — only the non-treponemal titre tracks response. Partner treatment and follow-up are part of the same workflow: trace and treat contacts to prevent re-infection.
The Jarisch-Herxheimer reaction must be recognised so it is not mistaken for penicillin allergy. Within about 24 hours of the first penicillin dose, particularly in early syphilis with a high spirochaete burden, the patient may develop fever, rigors, headache, myalgia, and a transient worsening of the rash — caused by the sudden release of antigens and inflammatory mediators from dying treponemes, not by hypersensitivity to penicillin. It is self-limiting and managed with antipyretics and reassurance; crucially, you do not withhold or stop penicillin because of it. Warning the patient in advance that this may happen prevents alarm and prevents the dangerous error of abandoning a curative drug.
- Monitor with the non-treponemal titre; fourfold (2-dilution) fall by 6–12 months = adequate response.
- No fall or a fourfold rise → treatment failure/re-infection → re-evaluate (consider neurosyphilis) and re-treat.
- Jarisch-Herxheimer = self-limiting febrile reaction to dying spirochaetes, not allergy — treat symptomatically, do not stop penicillin.
SELF-CHECK
A pregnant woman with reactive syphilis serology gives a clear history of anaphylaxis to penicillin. What is the correct management?
A. Treat her with doxycycline 100 mg twice daily for 14 days instead of penicillin
B. Desensitise her to penicillin and then treat with the stage-appropriate penicillin regimen
C. Withhold all treatment until after delivery to avoid an allergic reaction
D. Treat her with a single dose of azithromycin
Reveal Answer
Answer: B. Desensitise her to penicillin and then treat with the stage-appropriate penicillin regimen
In pregnancy, penicillin is the only accepted treatment for syphilis because it reliably treats the fetus and prevents congenital syphilis; doxycycline is contraindicated (fetotoxic). A penicillin-allergic pregnant woman must therefore be desensitised to penicillin and then treated with the stage-appropriate penicillin regimen. Withholding treatment risks stillbirth and congenital syphilis.
Self-Assessment — Syphilis Treatment Decision Cases
Consolidate the treatment workflow by reasoning through the decisions that examiners and patients will put to you, stating the rationale each time. First, fix the stage-to-regimen map: primary, secondary, and early latent syphilis get a single dose of benzathine penicillin G 2.4 million units intramuscularly; late latent and tertiary (non-neurological) disease get three weekly doses; neurosyphilis needs intravenous aqueous crystalline penicillin G because benzathine fails to reach the CSF. Second, handle the special populations: in pregnancy penicillin is the only acceptable drug and a penicillin-allergic mother must be desensitised, never given doxycycline; congenital syphilis is treated with aqueous or procaine penicillin over ten days (confirm exact dosing against current national guidance). Third, manage the aftermath: monitor with the non-treponemal titre expecting a fourfold fall by six to twelve months, and recognise the Jarisch-Herxheimer reaction as a self-limiting response to dying spirochaetes that is treated symptomatically without stopping penicillin.
For every self-check question, connect the answer back to a principle — why the depot form, why penicillin in pregnancy, why benzathine fails in neurosyphilis, and why a febrile reaction after the first dose is not an allergy. Reasoning from principle is what makes the workflow robust under the variations real patients present.
- Map stage → regimen (single dose / weekly × 3 / IV for neurosyphilis).
- Pregnancy → penicillin only (desensitise); congenital → 10-day penicillin course.
- Monitor by non-treponemal titre (fourfold fall = success); Jarisch-Herxheimer is not allergy — never stop penicillin for it.
SELF-CHECK
A man treated for early syphilis develops fever, rigors, headache, and a transient worsening of his rash about 8 hours after his benzathine penicillin injection. What is this, and what should be done?
A. Penicillin anaphylaxis — stop penicillin permanently and switch to doxycycline
B. The Jarisch-Herxheimer reaction — a self-limiting reaction to dying spirochaetes; manage with antipyretics and reassurance and do NOT stop penicillin
C. Treatment failure — re-treat immediately with a higher dose
D. Neurosyphilis developing acutely — perform an emergency lumbar puncture and stop treatment
Reveal Answer
Answer: B. The Jarisch-Herxheimer reaction — a self-limiting reaction to dying spirochaetes; manage with antipyretics and reassurance and do NOT stop penicillin
Fever, rigors, headache, myalgia, and transient rash worsening within ~24 hours of the first penicillin dose in early syphilis is the Jarisch-Herxheimer reaction, caused by antigen release from dying Treponema pallidum — not penicillin allergy. It is self-limiting; manage symptomatically with antipyretics and reassurance and continue penicillin.
CLINICAL PEARL
Two errors cause the most harm in syphilis treatment, and both are easy to avoid. First, never substitute doxycycline for penicillin in a pregnant woman — penicillin is the only drug that reliably protects the fetus, so a penicillin-allergic mother is desensitised and treated with penicillin. Second, never stop penicillin because of the Jarisch-Herxheimer reaction — the fever and rigors hours after the first dose are the spirochaetes dying, not an allergy, so you reassure, give antipyretics, and continue. Warn every early-syphilis patient about this reaction in advance, and warn yourself never to mistake it for hypersensitivity.