Page 3 of 12
DR13.1 | Autoimmune Vesiculobullous Disorder Diagnosis — SDL Guide (Part 3)
Self-Assessment: Vesiculobullous Disorder Diagnosis
Vesiculobullous Disorder Diagnosis
Use the following structured reasoning to consolidate the competency before you move on. The goal is not to memorise a table but to be able to walk from a bedside finding to a confident diagnosis and an appropriate next step. Work through each prompt deliberately, stating your reasoning aloud or in writing, and check yourself against the principle that the level of the epidermal split — intra-epidermal in pemphigus, sub-epidermal in bullous pemphigoid — drives every downstream feature, from blister character to Nikolsky's sign to the immunofluorescence pattern. If you find yourself uncertain on any item, return to the relevant section above rather than guessing, because reversing the cleavage plane is the single commonest and most dangerous error in this topic.
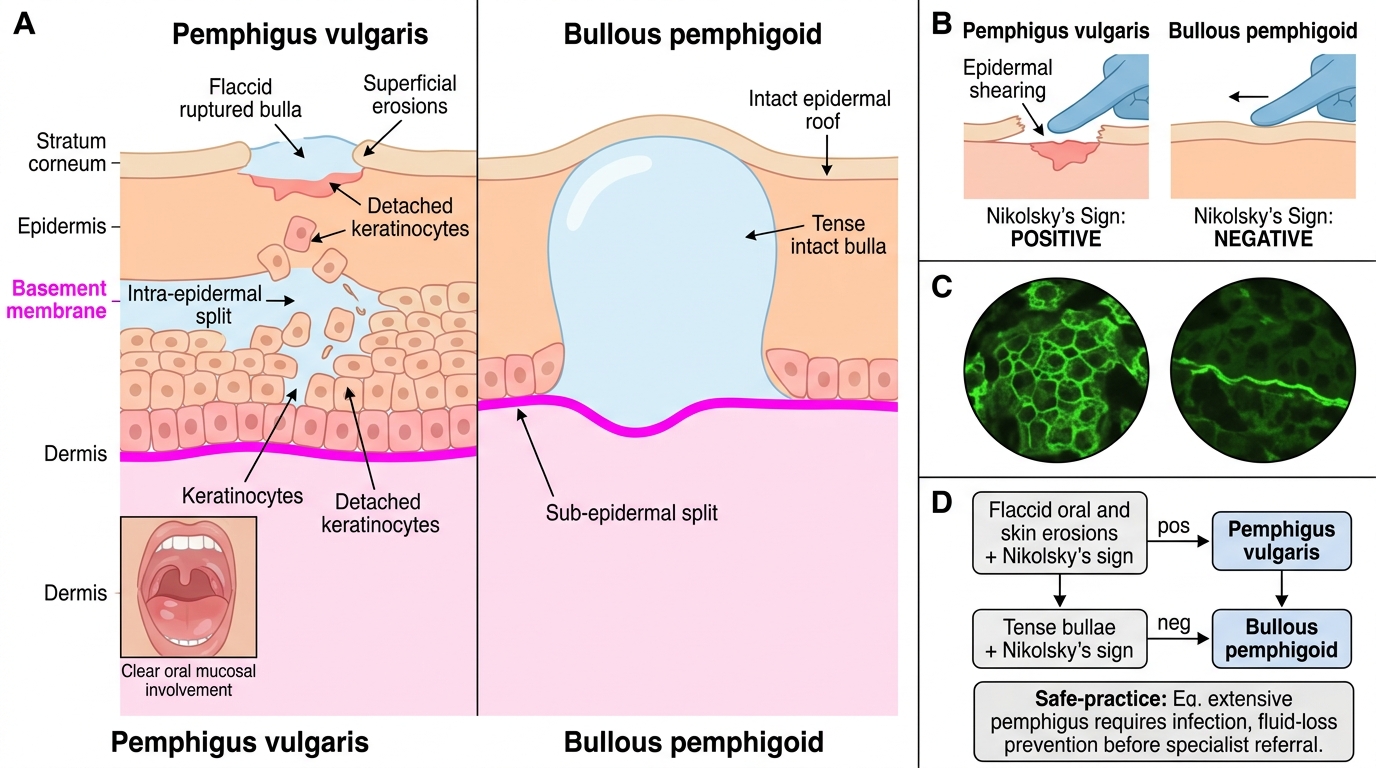
- Pattern recognition: For a patient with flaccid oral and skin erosions and a positive Nikolsky's sign, state the diagnosis, the split level, the target antigen, and the expected DIF pattern.
- Sign interpretation: Explain in one sentence why Nikolsky's sign is positive in pemphigus vulgaris but negative in bullous pemphigoid.
- Investigation choice: A patient has tense bullae and a negative Nikolsky's sign. List, in order, the investigations you would request and the result you expect from each.
- Safe practice: Name the complication that is the leading cause of death in extensive pemphigus and one step you would take to reduce that risk before referral.
CLINICAL PEARL
Anchor the whole topic to one rule and you will not reverse it under pressure: "Pemphigus is high, flaccid and positive; pemphigoid is deep, tense and negative." Pemphigus vulgaris splits HIGH (intra-epidermal, suprabasal acantholysis), gives FLACCID bullae and erosions with prominent oral disease, and has a POSITIVE Nikolsky's sign (anti-desmoglein 3/1). Bullous pemphigoid splits DEEP (sub-epidermal), gives TENSE bullae sparing the mouth in the elderly, and has a NEGATIVE Nikolsky's sign (anti-BP180/BP230). One caution: a positive Nikolsky's sign is not unique to pemphigus — it is also positive in Stevens-Johnson syndrome / toxic epidermal necrolysis and in staphylococcal scalded skin syndrome, so always read the sign together with the clinical context.