Page 6 of 22
DR8.2 | Herpes Simplex Recognition — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Differential Diagnosis and Investigations for Herpes Simplex
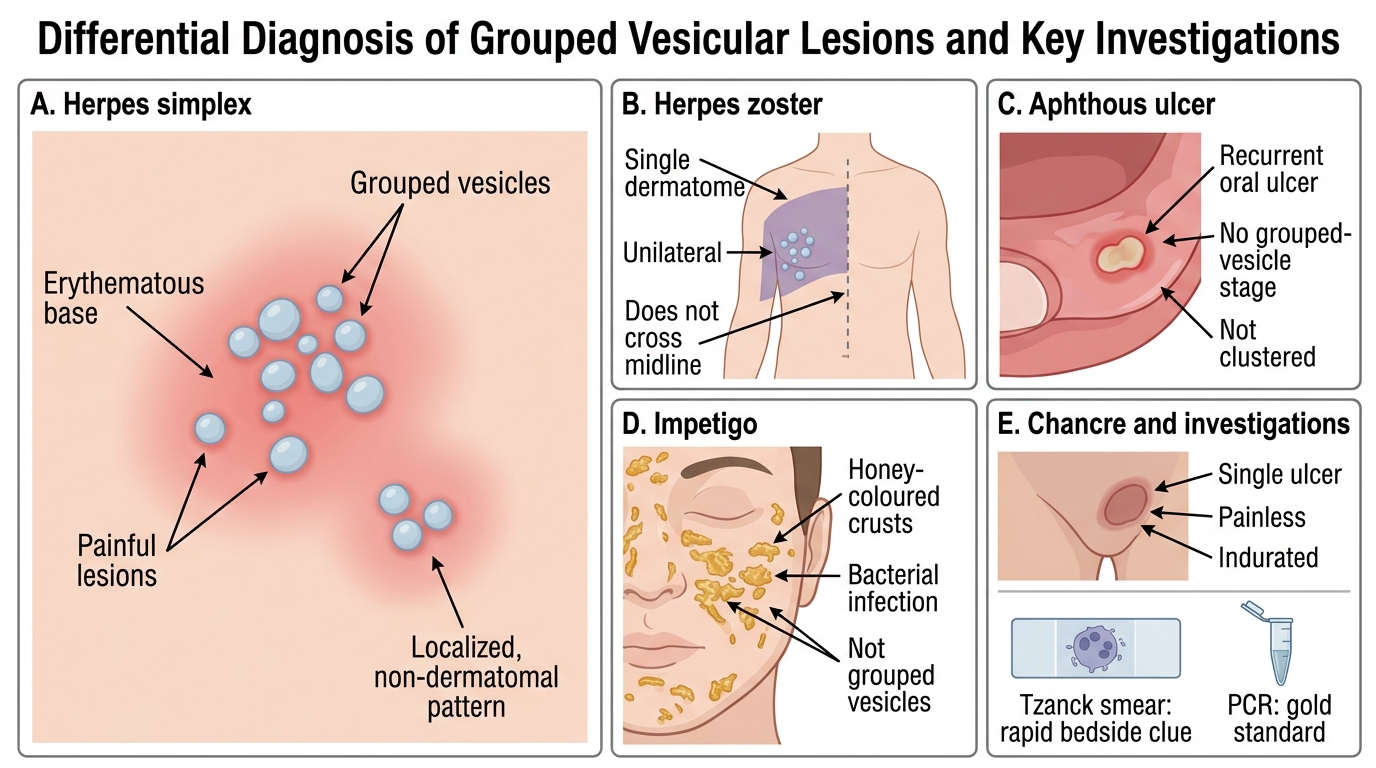
Several conditions mimic herpes simplex, and disciplined differentiation prevents both over- and under-treatment. The key discriminators are the lesion type (grouped vesicles versus other primary lesions), the distribution (localised versus dermatomal versus scattered), the pain character, and, where needed, a confirmatory test. Herpes zoster also produces grouped vesicles but is confined to a single dermatome, is unilateral and does not cross the midline — a pattern herpes simplex does not follow. Aphthous ulcers are painful oral ulcers but lack the preceding grouped-vesicle stage and the clustered pattern. Impetigo produces honey-coloured crusts rather than grouped vesicles on a red base and is bacterial. A syphilitic chancre is a single, painless, indurated ulcer — quite unlike the painful grouped vesicles of genital herpes — and must be considered in any genital ulcer. Investigations confirm the clinical impression: a Tzanck smear gives a rapid bedside clue, while PCR is the gold standard.
The practical differential and investigation points are:
- Herpes zoster: dermatomal, unilateral, does not cross midline (vs localised, non-dermatomal HSV).
- Aphthous ulcer: no grouped-vesicle stage, not clustered, recurrent oral ulcers.
- Impetigo: honey-crusted, bacterial, not grouped vesicles on erythema.
- Syphilitic chancre: single, painless, indurated genital ulcer (vs painful grouped vesicles).
- Investigations: Tzanck smear (multinucleate giant cells — confirms herpesvirus, not subtype); PCR (gold standard); viral culture; direct fluorescent antibody (DFA).
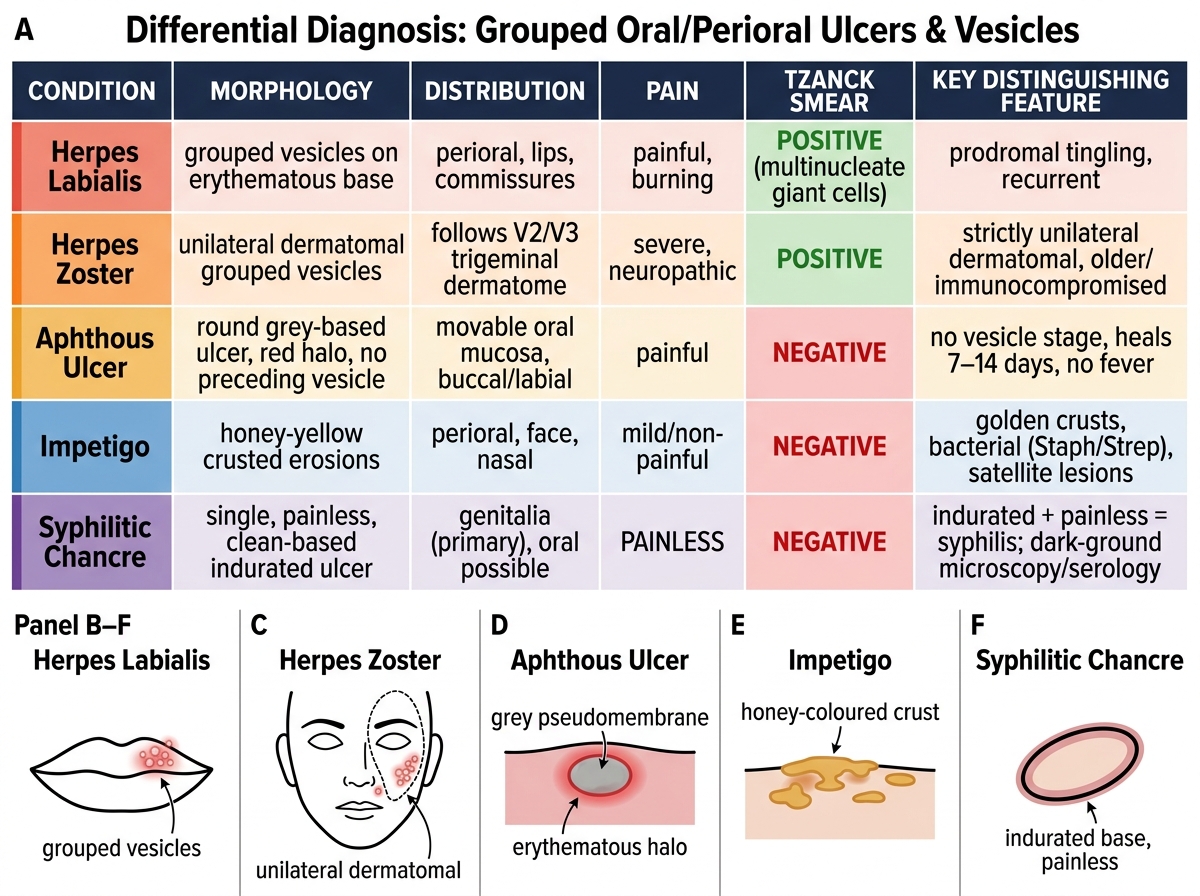
Differential Diagnosis of Grouped Oral/Perioral Ulcers and Vesicles
SELF-CHECK
A 30-year-old man presents with a single, painless, indurated ulcer on the glans penis. Which feature most argues AGAINST genital herpes simplex?
A. The lesion is on the genitalia
B. The ulcer is single, painless and indurated, whereas genital herpes typically presents as painful grouped vesicles or erosions
C. The patient is sexually active
D. There is no fever
Reveal Answer
Answer: B. The ulcer is single, painless and indurated, whereas genital herpes typically presents as painful grouped vesicles or erosions
Genital herpes simplex characteristically presents as painful grouped vesicles on an erythematous base that erode into shallow, tender ulcers; recurrences are preceded by a prodrome. A single, painless, indurated ulcer is the classic primary chancre of syphilis, not herpes. The site (genitalia) and sexual activity are common to both and do not distinguish them, and absence of fever is non-specific. Recognising that a painless indurated ulcer points to syphilis rather than herpes is essential, because it changes the investigation (dark-ground microscopy/serology) and management entirely. A Tzanck smear would not show multinucleate giant cells in a syphilitic chancre.
Management of Herpes Simplex
Management of Herpes Simplex
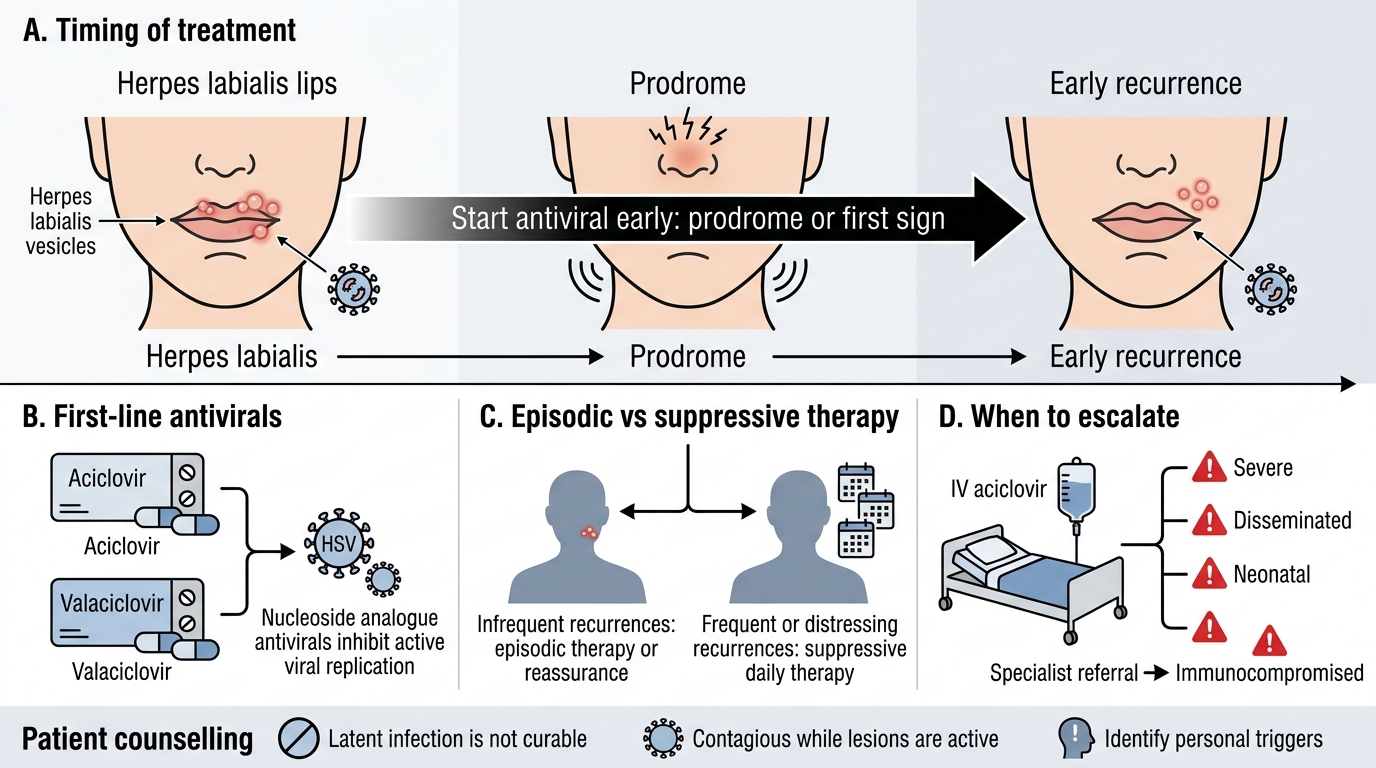
Management of herpes simplex rests on antiviral therapy that controls episodes, combined with patient education, and on recognising the minority who need more than simple measures. The mainstay drugs are the nucleoside analogues aciclovir and valaciclovir, which are most effective when started early — ideally during the prodrome or at the very first sign of a recurrence — because they act on actively replicating virus. For most patients with infrequent recurrent herpes labialis, episodic treatment or simply reassurance is appropriate; for those with frequent or distressing recurrences, suppressive (daily) therapy reduces the frequency of episodes. Severe, disseminated, neonatal or immunocompromised disease requires intravenous aciclovir and prompt specialist involvement, as these situations carry real risk. Counselling completes management: patients should understand that the virus is not curable, that it is contagious while lesions are active, and what their personal reactivation triggers are.
The management principles are:
- First-line antivirals: aciclovir or valaciclovir, started as early as possible (prodrome/first sign).
- Episodic therapy for infrequent recurrences; suppressive (daily) therapy for frequent or severe recurrent disease.
- Intravenous aciclovir for severe, disseminated, neonatal or immunocompromised infection — with specialist referral.
- Patient education: incurable latent infection, contagious while lesions are active (avoid skin contact, kissing, sharing utensils/razors), identify and where possible avoid triggers; consider partner counselling and STI screening for genital herpes.
Note: the antiviral doses used for episodic recurrent disease differ from those for primary or suppressive therapy; prescribe to a current formulary rather than from memory.
Self-Assessment: Herpes Simplex Recognition
Herpes Simplex Recognition: Morphology, Distribution, and Differentials
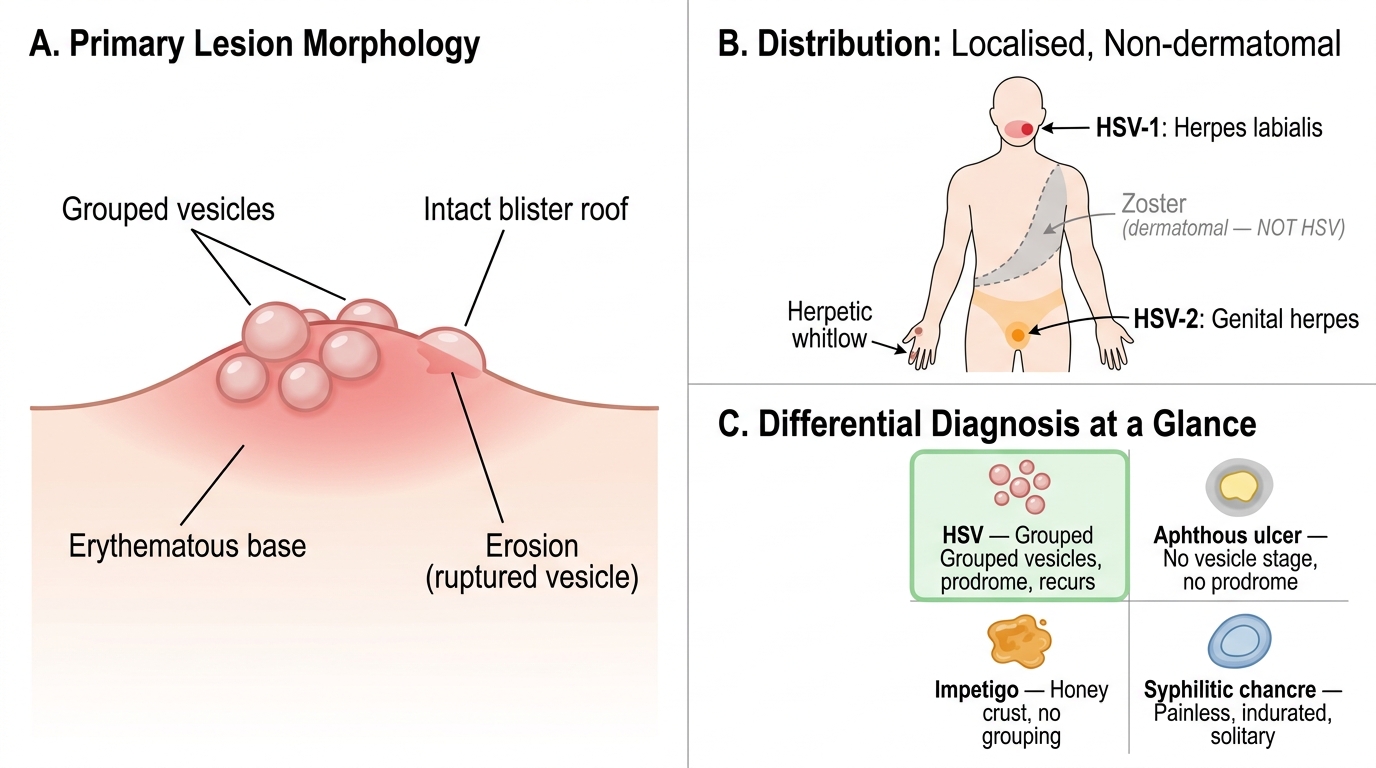
The aim of this closing section is to confirm that you can recognise herpes simplex on sight and separate it cleanly from its mimics, then choose the right next step. Recognition here is a short ordered process: read the primary lesion (grouped vesicles on an erythematous base), note the prodrome and the tendency to recur at the same site, place the distribution (localised and non-dermatomal), and only then decide whether a confirmatory test or treatment is needed. The scenarios you should be able to handle include the everyday recurrent cold sore, the painful genital eruption that needs distinguishing from a syphilitic chancre, the severe paediatric gingivostomatitis of primary infection, and the danger situations in neonates and the immunocompromised. Use the self-check below to rehearse moving from clinical picture to diagnosis to action, and notice where your reasoning hesitates.
For each scenario, ask in order:
- Is the primary lesion a group of vesicles on an erythematous base, with a prodrome?
- Is the distribution localised and non-dermatomal (HSV) rather than dermatomal (zoster)?
- Does the picture fit herpes simplex, or does a mimic (aphthous ulcer, impetigo, syphilitic chancre) fit better?
- What single confirmatory test, if any, and does an antiviral change the outcome here?
SELF-CHECK
A Tzanck smear from a herpes labialis lesion is positive. What does this confirm, and what is the appropriate first-line treatment for a troublesome recurrence caught early?
A. It confirms HSV-1 specifically; treat with oral antibiotics
B. It confirms a herpesvirus (multinucleate giant cells) but not the subtype; treat early with oral aciclovir or valaciclovir
C. It confirms molluscum contagiosum; treat with cryotherapy
D. It confirms syphilis; treat with benzathine penicillin
Reveal Answer
Answer: B. It confirms a herpesvirus (multinucleate giant cells) but not the subtype; treat early with oral aciclovir or valaciclovir
A positive Tzanck smear shows multinucleate giant cells, confirming a herpesvirus infection but not distinguishing HSV-1 from HSV-2 or HSV from VZV — subtype identification needs PCR. The appropriate first-line treatment for a troublesome recurrent herpes labialis episode is a nucleoside analogue antiviral, aciclovir or valaciclovir, started as early as possible (ideally in the prodrome) because the drugs act on replicating virus. Antibiotics treat bacterial infection (e.g. impetigo), cryotherapy treats molluscum, and benzathine penicillin treats syphilis — none is the treatment for herpes simplex.
CLINICAL PEARL
Recurrence at the same site after a tingling prodrome is the clinical fingerprint of herpes simplex — and a Tzanck smear, while useful, confirms only that you are dealing with a herpesvirus, never which one. When you see a genital ulcer, force yourself to separate the painful grouped vesicles/erosions of herpes from the single, painless, indurated chancre of syphilis, because the two diverge completely in investigation and treatment. Start aciclovir or valaciclovir as early as possible (the prodrome is ideal); the drugs work on replicating virus, so a late start adds cost with little benefit. Always treat severe, neonatal, disseminated or immunocompromised herpes as urgent — these are the situations where recognition genuinely saves lives.