Page 8 of 22
DR8.3 | Varicella Zoster Recognition — SDL Guide
Learning Objectives
- Recognise varicella (chickenpox) by its centripetal distribution and lesions in different stages simultaneously, and herpes zoster (shingles) by its dermatomal, unilateral pattern
- Explain how a single virus (VZV) causes varicella on primary infection and herpes zoster on reactivation
- Describe the clinical features, complications (including post-herpetic neuralgia) and diagnosis of varicella and zoster
- Differentiate varicella and zoster from their mimics and from herpes simplex, and outline antiviral, complication and prevention management
INSTRUCTIONS
Varicella zoster virus produces two clinically distinct diseases that every clinician must recognise on sight: varicella (chickenpox), the widespread itchy eruption of childhood, and herpes zoster (shingles), the painful dermatomal band of reactivation in adults and the elderly. This SDL builds the recognition skill for both — reading the polymorphic, centripetal rash of varicella with its lesions in different stages at once, and the unilateral dermatomal vesicles of zoster that do not cross the midline. Recognising these patterns, anticipating complications such as post-herpetic neuralgia and zoster ophthalmicus, and knowing when antivirals and referral are needed are core final-year competencies.
References
- Khanna N. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Viral Infections (Varicella and Herpes Zoster) (textbook)
- Sacchidanand S (ed). IADVL Textbook of Dermatology, 4th ed. Section: Varicella Zoster Virus Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 68-year-old man comes to you with three days of burning, stabbing pain across the left side of his lower chest, which he first thought was cardiac. Today a band of grouped blisters has erupted along exactly that strip of skin — and stops abruptly at the midline of his back and chest. The same virus that gave him chickenpox as a child has reawakened in a single nerve root, and the rash maps that nerve precisely. Recognising this dermatomal, unilateral eruption that does not cross the midline as herpes zoster — and recognising the polymorphic, centripetal rash of varicella in a child — lets you treat early, anticipate complications like post-herpetic neuralgia, and reassure correctly.
WHY THIS MATTERS
Varicella and herpes zoster are conditions you will diagnose throughout your career, in children and adults respectively. Varicella, though usually self-limiting, can be severe in adults, pregnant women, neonates and the immunocompromised, and is highly contagious. Herpes zoster causes significant morbidity through pain and post-herpetic neuralgia, can threaten sight when it involves the ophthalmic nerve, and — when it appears in a young, otherwise healthy adult or is unusually widespread — can be the first clue to underlying immunosuppression such as HIV. Recognising both promptly allows early antiviral therapy (which reduces complications), appropriate pain management, timely ophthalmology referral, and correct advice on contagion and prevention. This is high-yield, everyday clinical recognition.
RECALL
Recall from the viral foundations and herpes simplex SDLs, and from Microbiology, that varicella zoster virus is a herpesvirus that — like HSV — establishes lifelong latency in sensory ganglia and reactivates when cell-mediated immunity wanes. Recall the herpesvirus mechanism: primary infection, spread to and latency in dorsal root ganglia, and later reactivation back down a nerve to the skin. Recall too that a Tzanck smear from a fresh VZV vesicle shows multinucleate giant cells, identical to HSV, so cytology confirms a herpesvirus but cannot distinguish VZV from HSV. Keep in mind the role of waning immunity with ageing and immunosuppression — it is precisely this decline that precipitates zoster decades after the original chickenpox.
Recognising Varicella (Chickenpox): The Polymorphic Rash
Recognising Varicella: The Polymorphic Rash
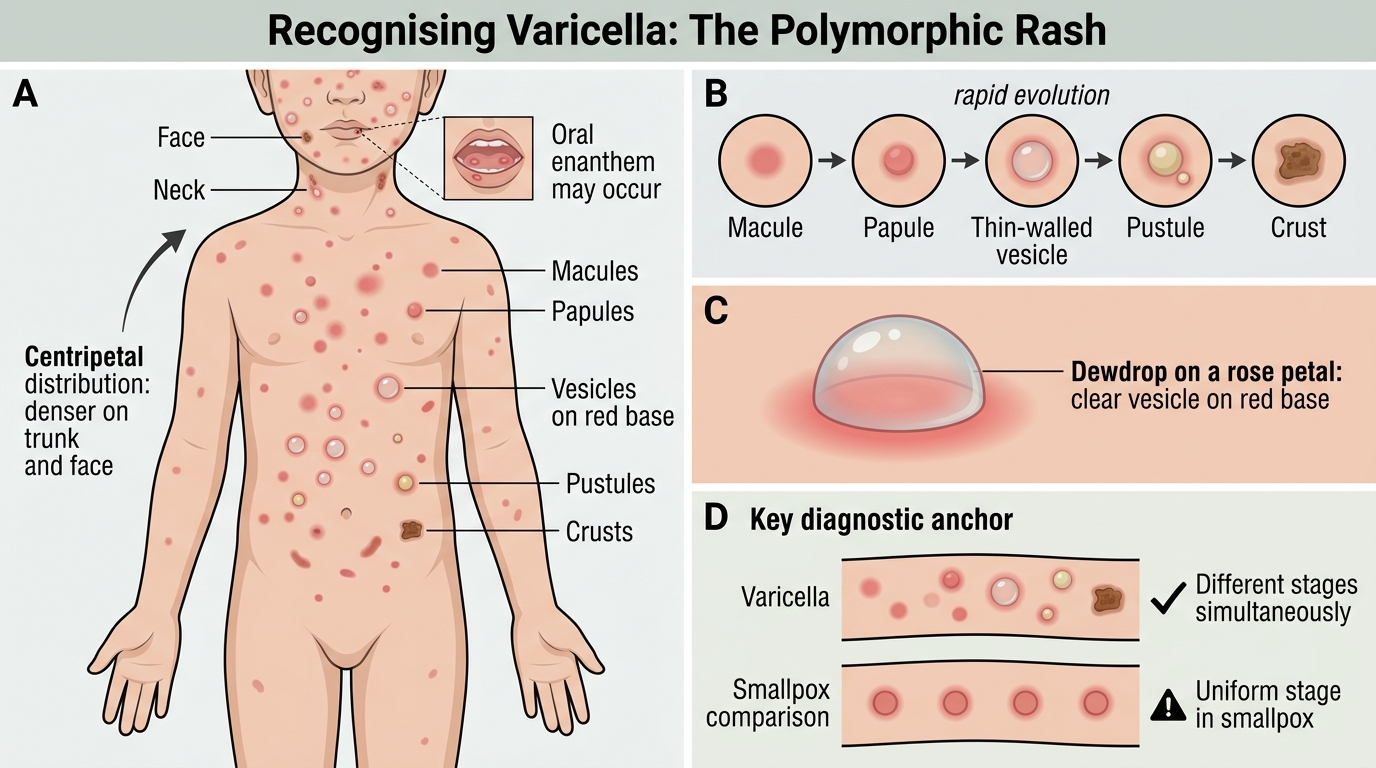
The single most reliable recognition feature of varicella is that lesions are present in several different stages at the same time — a property called polymorphism that immediately separates it from smallpox, in which all lesions are at the same stage. Varicella typically begins with fever and malaise, followed by an itchy eruption that starts on the trunk and face and spreads outward, giving a centripetal distribution that is denser centrally than on the limbs. Each lesion evolves rapidly through macule → papule → a thin-walled vesicle classically described as a 'dewdrop on a rose petal' (a clear vesicle on a red base) → pustule → crust, but because new crops keep appearing over several days, at any one moment you see macules, papules, vesicles and crusts side by side. Mucous membranes may be involved, producing shallow oral ulcers (an enanthem).
The features that make varicella recognisable are:
- Lesions in different stages simultaneously (macule, papule, vesicle, crust together) — the key diagnostic anchor.
- Centripetal distribution — denser on the trunk and face than on the limbs.
- The 'dewdrop on a rose petal' vesicle — a clear vesicle on an erythematous base.
- Preceding fever and malaise, marked pruritus, and possible mucosal (oral) involvement.
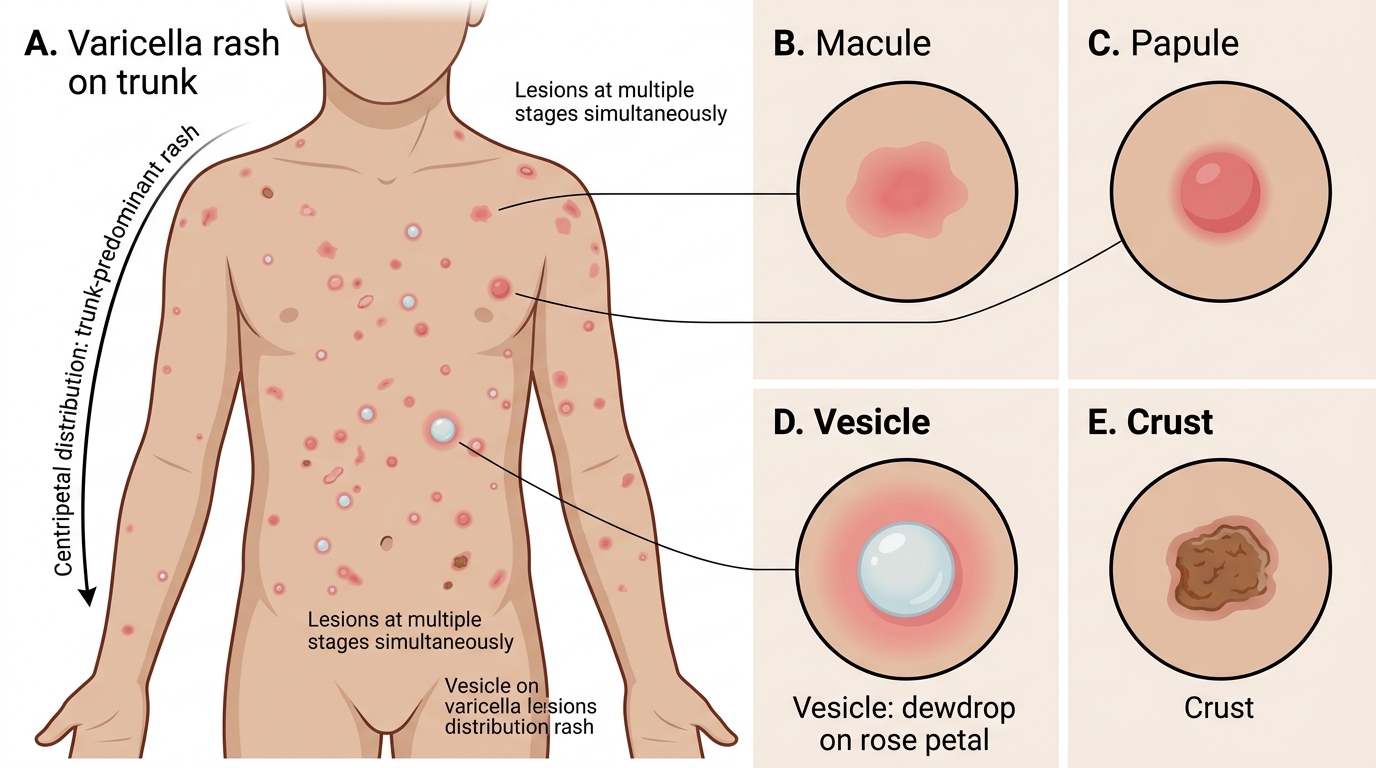
Varicella Rash: Trunk Distribution and Lesion Stages
Recognising Herpes Zoster (Shingles): Dermatomal Reactivation
Recognising Herpes Zoster: Dermatomal Reactivation
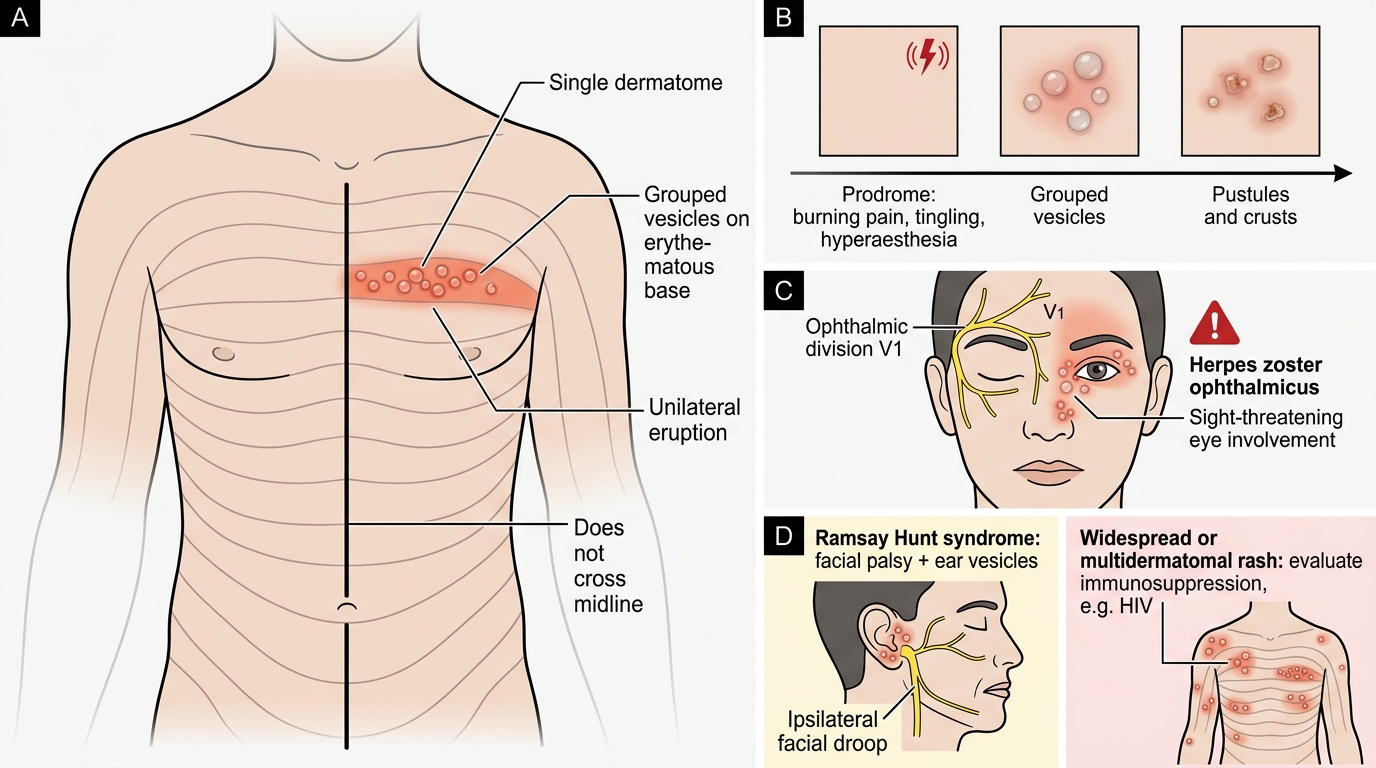
Herpes zoster is recognised by its strict confinement to a single dermatome: a band of grouped vesicles that is unilateral and does not cross the midline, mapping precisely onto the territory of the affected nerve root. The eruption is very often preceded by a prodrome of dermatomal pain, burning, tingling or hyperaesthesia that can begin days before any rash and may be mistaken for cardiac, pleuritic or abdominal pain depending on the dermatome involved. Once the rash appears, grouped vesicles on an erythematous base develop along the dermatome, evolve to pustules and crusts over several days, and heal — sometimes with scarring. Certain sites demand particular vigilance: involvement of the ophthalmic division of the trigeminal nerve (herpes zoster ophthalmicus) threatens the eye, and involvement of the facial/auditory nerves (Ramsay Hunt syndrome) causes facial palsy with ear vesicles.
The features that make herpes zoster recognisable are:
- Dermatomal, unilateral grouped vesicles that do not cross the midline — the defining pattern.
- A prodrome of dermatomal pain preceding the rash, sometimes mimicking visceral pain.
- Important danger variants: zoster ophthalmicus (ophthalmic division — sight-threatening) and Ramsay Hunt syndrome (facial palsy with ear vesicles).
- A widespread or multidermatomal eruption, or zoster in a young healthy adult, should prompt evaluation for immunosuppression (e.g. HIV).
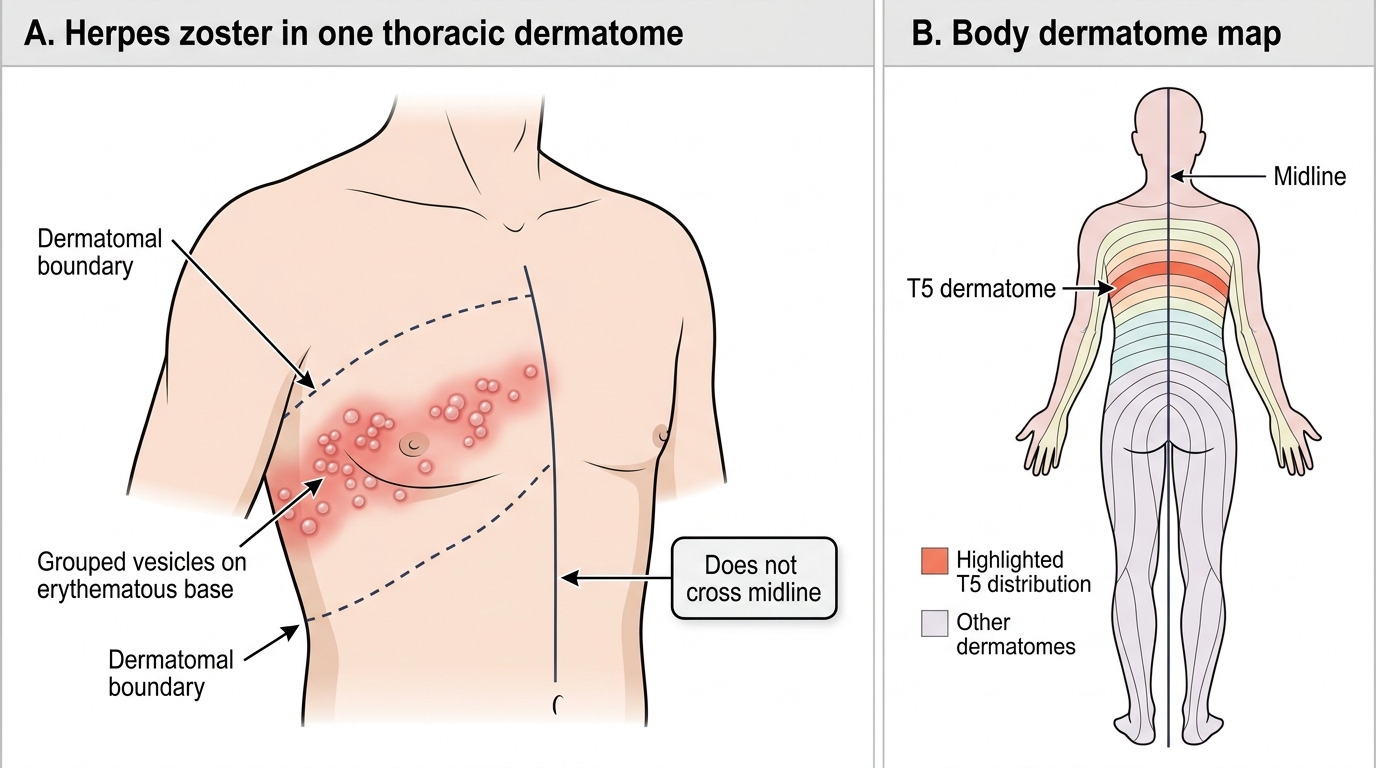
Herpes Zoster in a Single Thoracic Dermatome
SELF-CHECK
Which single feature most reliably distinguishes varicella (chickenpox) from smallpox on inspection of the rash?
A. Varicella spares the trunk and affects mainly the limbs
B. In varicella, lesions are present in different stages simultaneously, whereas in smallpox all lesions are at the same stage
C. Varicella lesions never involve mucous membranes
D. Varicella lesions are dermatomal and do not cross the midline
Reveal Answer
Answer: B. In varicella, lesions are present in different stages simultaneously, whereas in smallpox all lesions are at the same stage
The classic distinguishing feature of varicella is that lesions appear in successive crops, so macules, papules, vesicles and crusts are all present at the same time (polymorphism). In smallpox, by contrast, lesions evolve synchronously and are all at the same stage. Varicella is centripetal (trunk and face more than limbs), not limb-predominant, and may involve mucous membranes. A dermatomal, midline-respecting pattern describes herpes zoster, not varicella. Recognising simultaneous multiple stages is the key bedside anchor for varicella.
VZV Pathogenesis: Primary Infection to Reactivation
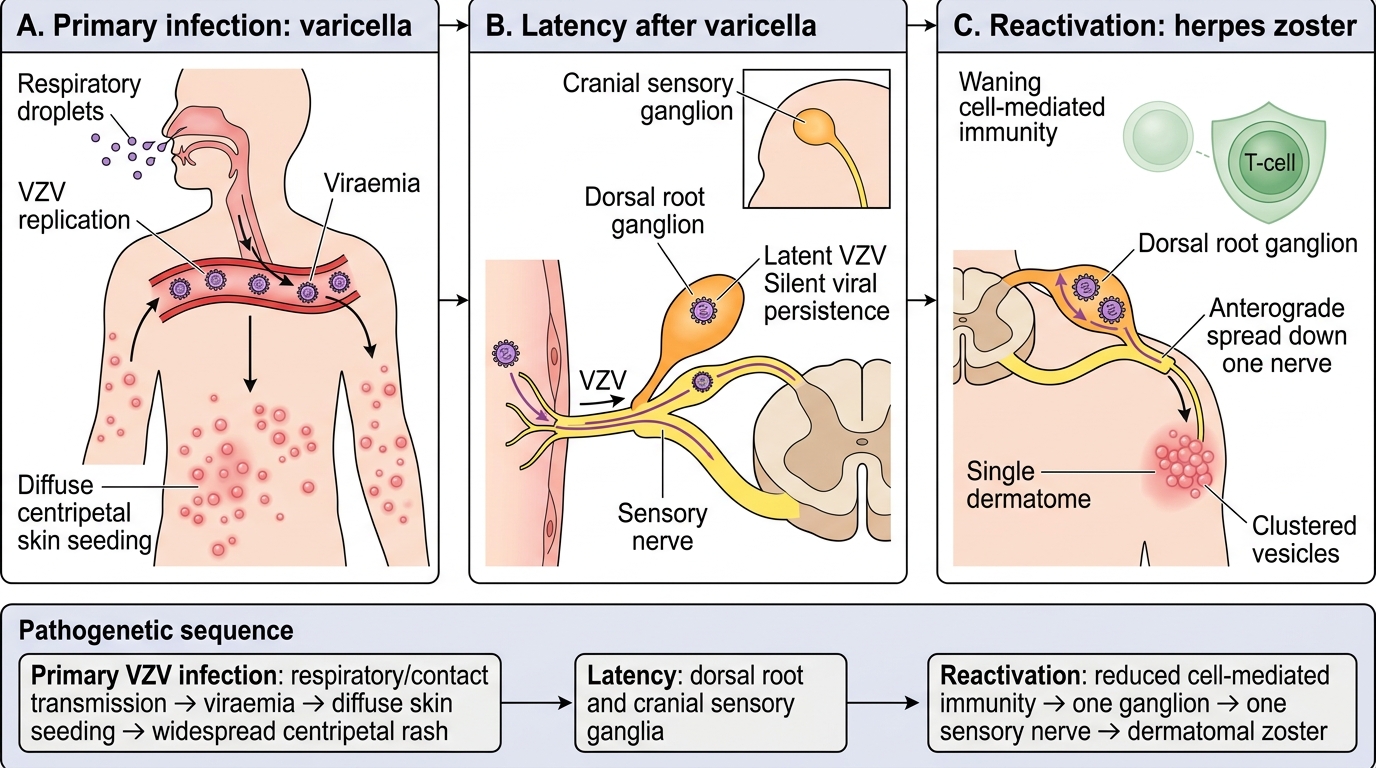
VZV Pathogenesis: Varicella to Zoster
Understanding that varicella and herpes zoster are two phases of a single viral life cycle explains why one virus produces two such different rashes. Primary infection with VZV occurs by respiratory droplet inhalation or direct contact with vesicle fluid; the virus replicates, produces a viraemia, and seeds the skin diffusely — giving the widespread, centripetal eruption of varicella. After the primary illness resolves, the virus is not cleared: it travels along sensory nerves and establishes latency in the dorsal root (and cranial sensory) ganglia, where it persists silently for decades. Reactivation occurs when cell-mediated immunity wanes — with advancing age, HIV infection, malignancy, chemotherapy or immunosuppressive therapy — at which point the virus replicates in a single ganglion and travels back down that one sensory nerve to the skin, producing the dermatomal eruption of herpes zoster. This is why zoster is confined to one dermatome and why it is commoner in the elderly and the immunocompromised.
The pathogenetic sequence to hold in mind is:
- Primary infection (varicella): respiratory/contact transmission → viraemia → diffuse skin seeding → widespread centripetal rash.
- Latency: VZV persists in dorsal root and cranial sensory ganglia after varicella resolves.
- Reactivation (zoster): waning cell-mediated immunity (ageing, HIV, malignancy, immunosuppression) → replication in one ganglion → spread down a single nerve → dermatomal rash.
- The same waning-immunity principle explains why widespread or atypical zoster should prompt a search for an immunocompromising cause.