Page 1 of 17
FM3.{1,3} | Asphyxia: General & Mechanical — SDL Guide
Learning Objectives
- Define asphyxia and describe the four classic stages of the asphyxial process
- Classify asphyxia systematically by mechanism and give examples of each type
- Describe the general post-mortem signs common to all asphyxial deaths and comment on their specificity
- Describe the clinical features, PM findings and medicolegal aspects of smothering, choking, traumatic asphyxia and sexual asphyxia
- Explain the medicolegal significance of asphyxial deaths and how a forensic physician approaches manner-of-death determination
INSTRUCTIONS
Asphyxial deaths are among the most common categories encountered in Indian medico-legal practice. Whether a body found with perioral bruising, a crowd-crush victim at a temple stampede, or an infant with unexplained cyanosis — the forensic physician must recognise the signs, classify the mechanism, and provide defensible testimony. This module builds the conceptual foundation for all asphyxial deaths. Subsequent SDLs extend these principles to hanging, strangulation, and drowning.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old woman is brought to the emergency department unresponsive. Bystanders report she was found collapsed at the base of a collapsed grain storage structure that had fallen on her. She has cyanotic lips, engorged neck veins, and pinpoint haemorrhages across both conjunctivae. The rescue team notes there is no external wound. The emergency physician asks the attending intern: 'What happened to her?' The intern recognises scattered subconjunctival petechiae but cannot explain why her face is congested while her torso appears pale. Can you?
WHY THIS MATTERS
Understanding asphyxia is foundational to forensic medicine because a substantial proportion of unnatural deaths — including many that initially appear natural — involve some form of asphyxial mechanism. In a busy government mortuary in India, asphyxial deaths account for a significant fraction of the forensic autopsies: they include hanging (the most common form of suicide in many Indian states), infanticide by smothering, accidental choking, crowd crushes, and deaths attributed to neglect. Each type leaves characteristic but overlapping PM signs, and the forensic physician must be able to (1) recognise the general asphyxial pattern, (2) identify the specific mechanism, (3) comment on the manner of death, and (4) provide an opinion that withstands cross-examination. Missing a smothering or misattributing a traumatic asphyxia as a cardiac event can have profound legal consequences.
RECALL
Before reading ahead, recall the following from Year-1 Physiology and Anatomy:
- Respiration and hypoxia: What happens to the brain when oxygen supply fails for 4–5 minutes? What are the cardiovascular responses to rising PaCO₂?
- Neck anatomy: Can you name the major blood vessels and cartilages of the neck (carotid arteries, jugular veins, hyoid bone, thyroid cartilage, cricoid, trachea)? These structures are critical in distinguishing hanging from strangulation.
- Lymphatic drainage of the head: Why does obstruction of venous return from the head cause such rapid congestion of the face and conjunctivae compared with the trunk?
Hold these in mind — they are the physiological scaffolding on which asphyxial pathology is built.
Stages and Pathophysiology of Asphyxia
Asphyxia is defined as a condition arising from interference with respiration, leading to insufficient oxygen reaching the tissues with concomitant accumulation of carbon dioxide in the blood. The word is derived from the Greek a (without) + sphyxis (pulse). In forensic medicine, the term is used specifically for mechanically-induced respiratory failure that results in death — it is a mechanism of death, not a single disease.
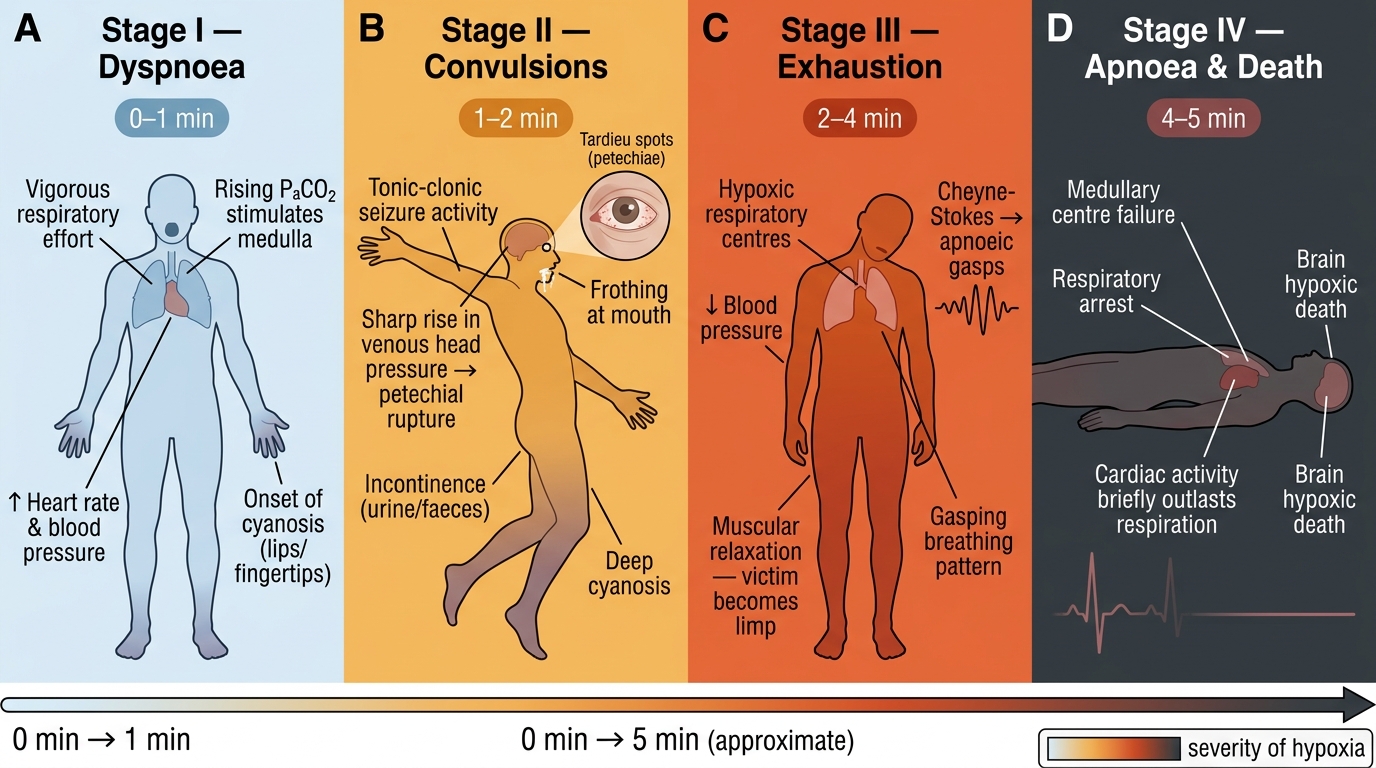
The Four Stages of Asphyxia: A Physiological Timeline (0–5 Minutes)
The asphyxial process passes through four recognisable and overlapping stages, each with its own physiological signature:
- Stage of dyspnoea (0–1 minute): The rising PaCO₂ stimulates the respiratory centres in the medulla. The victim struggles vigorously, taking deep, rapid inspiratory and expiratory efforts. Heart rate and blood pressure rise. This is the most vigorous phase — if restraint is involved, struggle marks may be produced here.
- Stage of convulsions (1–2 minutes): Hypoxia begins to affect the cerebral cortex. Generalised tonic-clonic convulsions may occur. Frothing at the mouth, incontinence of urine and faeces, and cyanosis deepen. Venous pressure in the head rises sharply — this is when Tardieu spots (petechial haemorrhages from overdistension and rupture of terminal venules) are produced.
- Stage of exhaustion (2–4 minutes): Respiratory efforts diminish as the respiratory centres become hypoxic. Respirations become slow and irregular (Cheyne-Stokes pattern), then gasping ('apnoeic gasps'). Blood pressure falls. The victim becomes limp.
- Stage of apnoea and death (4–5 minutes total): The medullary centres fail. Cardiac activity persists briefly beyond respiratory arrest (the heart is more hypoxia-tolerant than the brain), then cardiac arrest supervenes. Irreversible brain death follows within minutes of complete cerebral anoxia.
The mechanism of death in asphyxia is, in essence, a cascade from hypoxia → raised venous pressure → cerebral oedema and anoxic neuronal death → cardiorespiratory arrest. The exact timing is influenced by the completeness of respiratory obstruction, pre-existing cardiovascular status, ambient temperature, and the victim's level of resistance.
Classification of Asphyxia
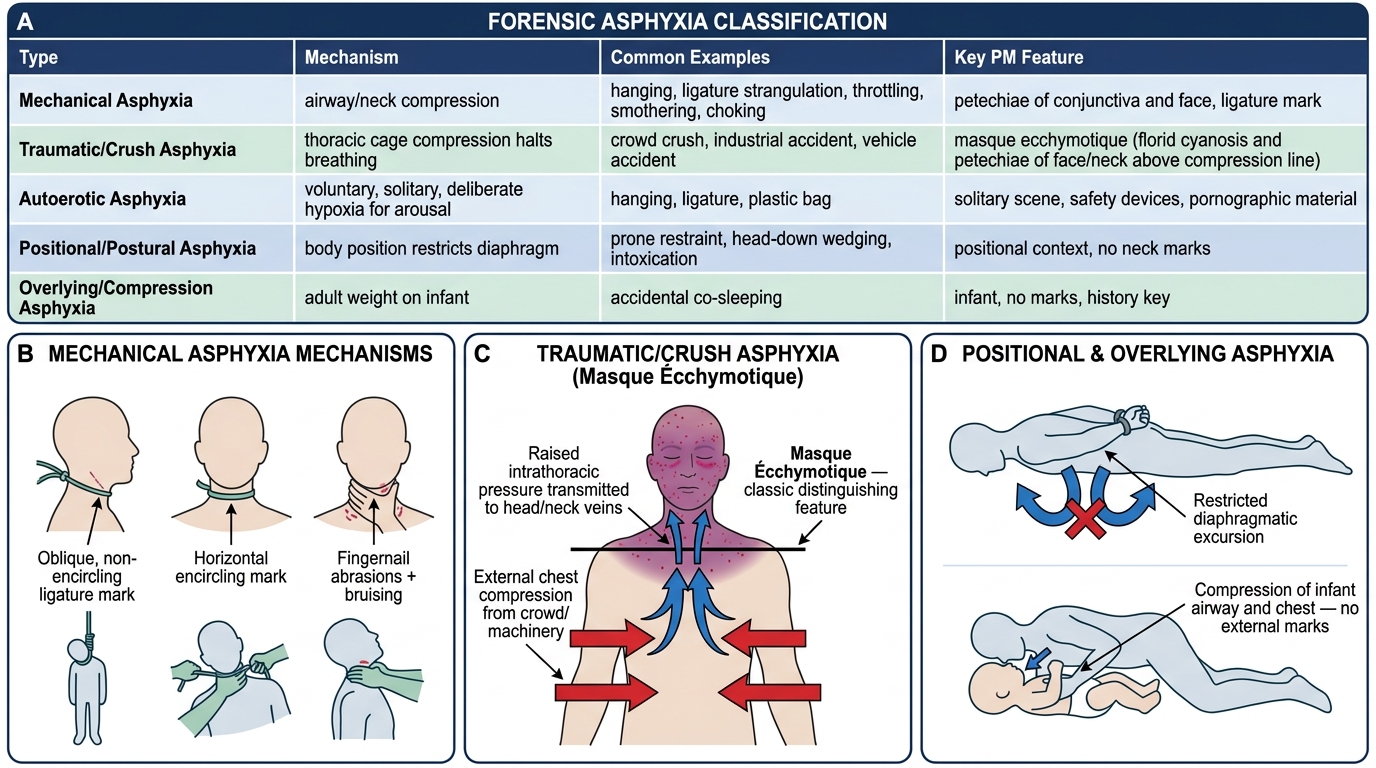
A systematic classification of asphyxia is essential for both examination and medico-legal practice, because mechanism determines investigation, PM findings, and court opinion. The most practically useful classification is by the external force or anatomical location of the obstruction:
Classification of Asphyxia Types: Mechanism, Examples & Post-Mortem Features
A. Mechanical asphyxia — the largest forensic category:
• Compression of the neck: hanging, strangulation by ligature, throttling (manual strangulation)
• Obstruction of the external airway (nose and mouth): smothering (pillow, hand), overlying (burking)
• Internal airway obstruction: choking (foreign body at larynx, trachea, bronchus); café-coronary syndrome (food bolus at larynx in elderly/inebriated)
B. Traumatic / crush asphyxia — the chest wall is compressed, preventing respiratory excursion: crowd crush, industrial accidents (machinery, building collapse), vehicle accident. The raised thoracic pressure is transmitted to the head and neck veins, producing the classic masque ecchymotique.
C. Sexual (autoerotic) asphyxia — deliberate, voluntary, and typically solitary reduction of oxygen during sexual activity to heighten arousal. Mechanism may be hanging, ligature, or plastic bag. The person intends to release themselves before loss of consciousness but the mechanism becomes unintentional.
D. Positional / postural asphyxia — the body position (particularly in intoxication, certain restraint positions, or neurological disability) mechanically restricts diaphragmatic movement: e.g., head-down position, prone restraint with wrists behind back, or wedging in a confined space.
E. Overlying / compression asphyxia — an adult rolling over an infant (accidental), or deliberate weight on the chest/face (homicide).
This schema maps cleanly onto the PM findings expected and the legal questions that arise in each scenario.
SELF-CHECK
Which stage of asphyxia is characterised by vigorous respiratory efforts, rising blood pressure, and is the phase during which Tardieu spots begin to form?
A. Stage of dyspnoea
B. Stage of convulsions
C. Stage of exhaustion
D. Stage of apnoea
Reveal Answer
Answer: B. Stage of convulsions
Tardieu spots form during the stage of convulsions (stage 2, approximately 1–2 minutes into asphyxia), when cerebral hypoxia causes venous congestion and raised pressure in the terminal venules of visceral serosal surfaces and conjunctivae, leading to their rupture as petechial haemorrhages. The stage of dyspnoea precedes this and is characterised primarily by vigorous ventilatory effort and cardiovascular stimulation; Tardieu spots form as venous pressure escalates into the convulsive stage.
Post-Mortem Signs of Asphyxial Deaths
The general PM signs of asphyxia form a recognisable constellation, but it is critical to understand that no single sign is pathognomonic — each has a differential diagnosis. The forensic value lies in the pattern, not the individual finding.
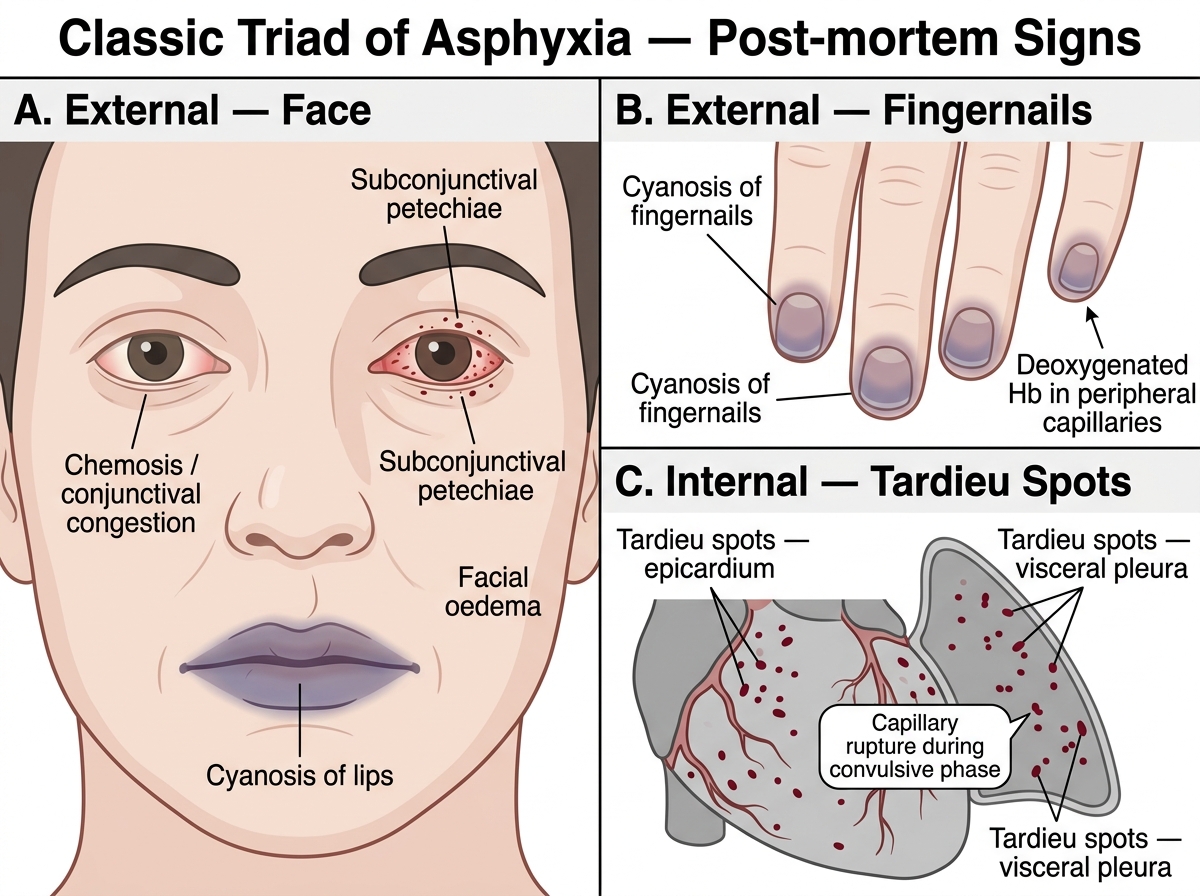
Classic Triad of Asphyxia: External and Internal Post-mortem Signs
External signs:
- Cyanosis: Blue-purple discolouration of the lips, fingernails, and mucous membranes due to deoxygenated haemoglobin accumulation in peripheral capillaries. Present in most asphyxial deaths, but also in any hypoxic death and some poisonings (e.g. nitrites, sulphaemoglobin).
- Congestion of the face and conjunctivae: Particularly prominent when the neck veins are obstructed (hanging, strangulation). The face becomes plethoric and cyanotic; the conjunctivae are injected and swollen (chemosis).
- Subconjunctival and scleral petechiae: Haemorrhagic spots on the bulbar conjunctiva — a sensitive and easily-inspected sign. Not exclusive to asphyxia (also raised venous pressure from any cause, CPR).
- Facial oedema and puffiness: Due to venous obstruction. More marked in neck-compression deaths.
Internal signs:
- Tardieu spots (taches de Tardieu): Petechial haemorrhages on the visceral pleura, epicardium, and occasionally under the meningeal coverings. These are 1–2 mm, numerous, and result from overdistension and rupture of capillaries and terminal venules during the convulsive phase. They are a classic asphyxia sign but are NOT pathognomonic — they also occur in any death associated with raised venous pressure, CPR, and vomiting during agonal phase.
- Fluidity of blood: Asphyxial deaths tend to produce dark, fluid blood due to the high CO₂ content at time of death, which shifts the oxygen dissociation curve and activates fibrinolytic pathways. Clotting is poor.
- Venous congestion of viscera: Liver, spleen, and kidneys are congested (dark and oedematous). The right heart is typically distended with blood.
- Pulmonary oedema: Alveolar oedema may be present, particularly with prolonged or partial asphyxia.
Limitations and caveats: Many of these signs (cyanosis, petechiae, congestion) can be absent in rapid asphyxial deaths (e.g. sudden vagal cardiac arrest in immersion syndrome) or modified by intervening decomposition, CPR, or prior cardiopulmonary disease. The absence of these signs does not exclude asphyxia.