Page 3 of 17
FM3.{1,3} | Asphyxia: General & Mechanical — SDL Guide (Part 3)
Medicolegal Inference and Certification in Asphyxial Deaths
Medicolegal Decision Framework for Asphyxial Deaths
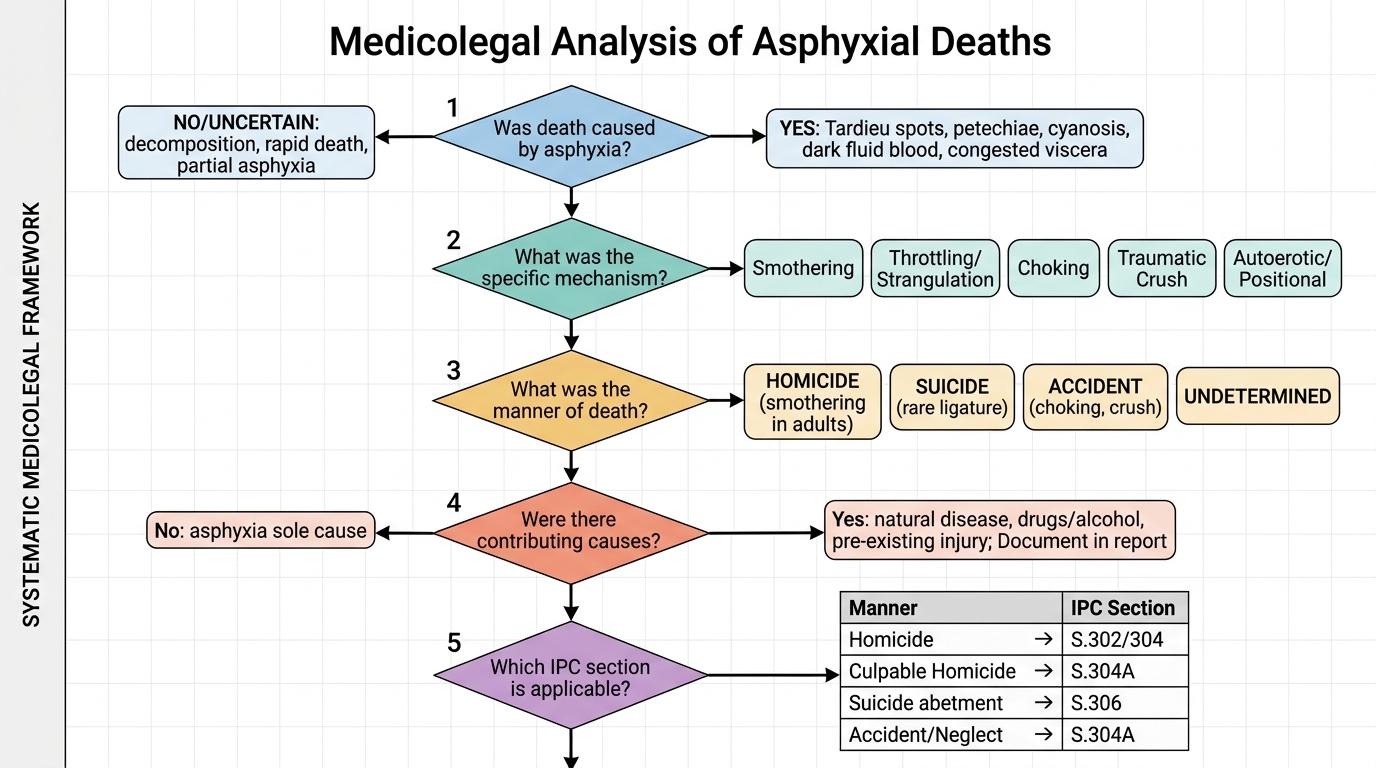
The forensic physician examining an asphyxial death must address five medicolegal questions with systematic rigour, drawing on the PM findings, scene investigation, witness statements, and clinical history.
1. Was death caused by asphyxia? This is established by the PM findings: the general asphyxial constellation (Tardieu spots, petechiae, cyanosis, fluid dark blood, congested viscera) combined with the specific findings for the mechanism (ligature mark, masque ecchymotique, foreign body, perioral injuries). A negative result does not exclude asphyxia — partial asphyxia, rapid death, or decomposition can modify all these signs.
2. What was the specific mechanism? The precise type (smothering, throttling, traumatic, autoerotic, positional) must be identified insofar as the evidence permits. Each mechanism has legal implications that differ substantially.
3. What was the manner of death? Manner = intent and circumstance: homicide, suicide, accident, or undetermined. General principles:
• Smothering in adults: strongly suggests homicide unless the victim was unconscious
• Choking: almost always accident
• Traumatic crush asphyxia: almost always accident or neglect
• Autoerotic asphyxia: accidental by intent, though the death is unintentional
• Positional asphyxia: accident (often with intoxication) or rarely neglect
4. Were there other contributing causes of death? Asphyxia may be accompanied by trauma (rib fractures in crush), head injury (from falling in hanging), or pre-existing disease. The death certificate should reflect the primary mechanism and significant contributors.
5. IPC and legal framework: The precise IPC section charged depends on the manner of death and the intent of the perpetrator. IPC Section 302 (murder) applies if homicidal asphyxia is proven with intent. Section 304 (culpable homicide not amounting to murder) if intent is less clear. Section 304A (causing death by negligence — e.g. crowd management failure leading to crush asphyxia). The forensic physician does not determine guilt but provides the medical evidence on which the court determines the IPC charge.
Inquest and certification: All suspected unnatural asphyxial deaths must be referred for inquest (executive magistrate under CrPC Section 174, or police inquest in some states). The forensic physician's PM report becomes part of the court record. Death must not be certified as natural if the PM findings suggest asphyxia. When findings are equivocal, the certificate should state 'pending further investigation.'
CLINICAL PEARL
Tardieu spots are a sign of asphyxia — not proof of it. They appear in any death associated with raised venous pressure: vigorous CPR, heart failure, and even violent vomiting during the agonal phase can produce them. Conversely, they may be absent in rapid asphyxia (vagal cardiac arrest), deaths with severe anaemia, or if the body has been submerged. The PM report should always describe Tardieu spots within their clinical context — 'petechial haemorrhages on the visceral pleura consistent with, but not diagnostic of, raised venous pressure as seen in asphyxial deaths' — rather than asserting them as proof of a specific mechanism.
SELF-CHECK
The masque ecchymotique (traumatic cyanosis) in crush/traumatic asphyxia is characterised by intense violet-blue discolouration, petechiae, and oedema of the face and upper chest with a sharp lower demarcation. What is the physiological mechanism for this sharply demarcated distribution?
A. Direct trauma to the facial blood vessels from the compressing object
B. Retrograde transmission of raised intrathoracic pressure through valveless jugular veins to the capillary beds of the face and upper extremities
C. Blockade of the thoracic lymph ducts preventing facial lymph drainage
D. Sympathetic vasoconstriction of the trunk arteries diverting blood to the face
Reveal Answer
Answer: B. Retrograde transmission of raised intrathoracic pressure through valveless jugular veins to the capillary beds of the face and upper extremities
When the thorax is compressed, intra-thoracic pressure rises sharply and is transmitted retrograde through the superior vena cava into the jugular veins, which — unlike the peripheral veins of the lower body — are valveless above the clavicle. This back-pressure ruptures the tiny capillaries and venules of the face, eyelids, and upper neck, producing petechiae and oedema confined to the region drained by the superior vena cava. The lower body remains pale because the inferior vena cava and its tributaries are compressed separately and do not communicate with the superior venous circuit at this pressure level.