Page 10 of 17
FM2.17-19 | Deaths from Physical Agents & Neglect — SDL Guide (Part 2)
Lightning and Electrocution
Lightning and domestic/industrial electrocution are both forms of electrical death, but they differ so fundamentally in mechanism, voltage, current characteristics, and PM findings that they must be treated as entirely distinct entities. Confusing them — particularly attributing Lichtenberg figures to domestic electrocution or vice versa — is a forensic error with serious ML consequences.
Lightning vs. Domestic Electrocution: Characteristic Skin Findings
Lightning:
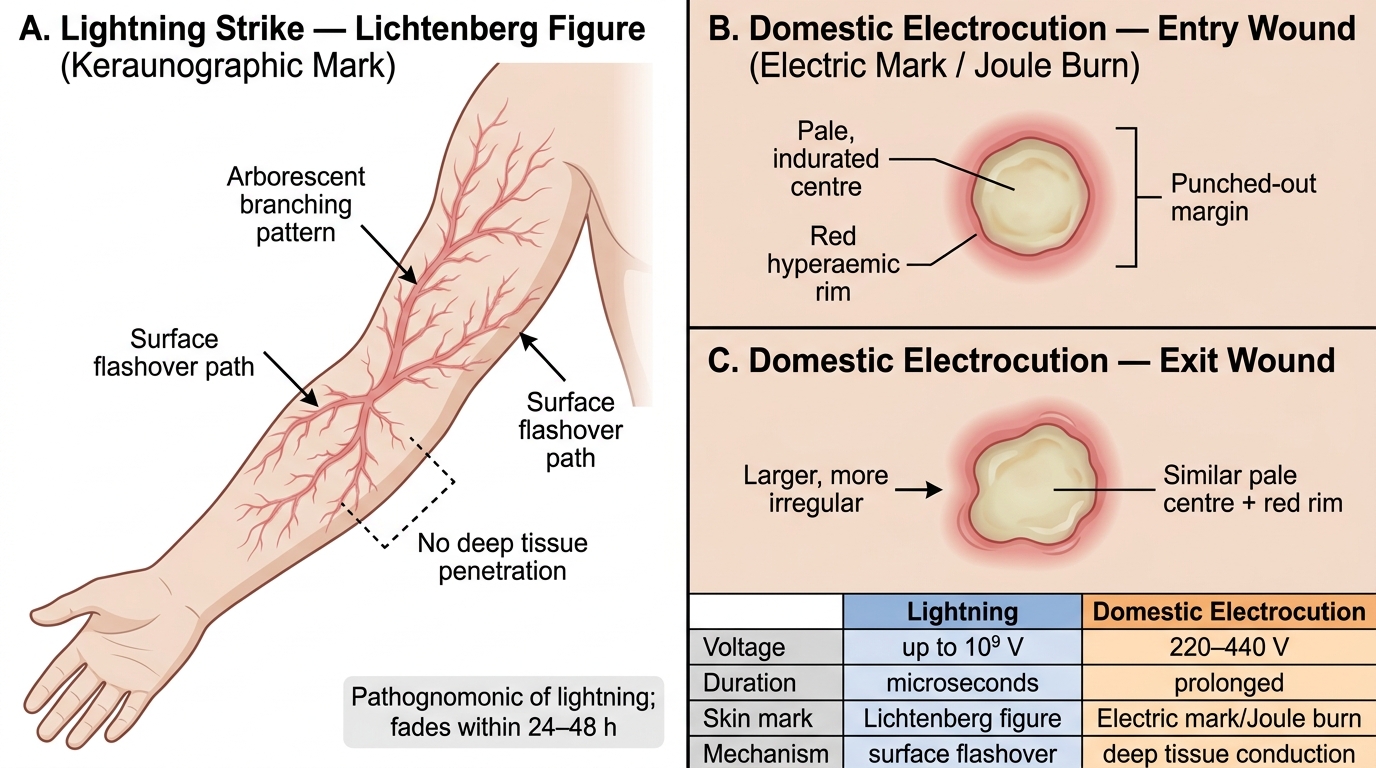
Lightning strikes carry an enormous voltage (up to 1 billion volts) and current (up to 200,000 amperes), but for an extraordinarily brief duration (microseconds). The massive energy discharge is primarily a flashover — the current travels over the surface of the body rather than through it, because the extremely brief duration does not allow deep tissue penetration.
Key PM findings in lightning:
• Lichtenberg figures (feathering, arborescent burns, Keraunographic marks): PATHOGNOMONIC of lightning. These are red, branching, fern-like or arborescent skin markings following the surface discharge path. They appear within hours and typically fade within 24–48 hours, making early examination and photography essential. They are NOT simple burns — they are a combination of vascular congestion, capillary rupture, and electrothermal injury along the flashover path.
• Clothes blown off or torn: The steam explosion from body moisture heated by the current can explosively expand, ripping clothing from the body. Metal objects (buckles, zippers) may be magnetised.
• Keraunoparalysis: Temporary paralysis of limbs following lightning — a well-recognised, typically transient, phenomenon in survivors. Not a PM finding but important in clinical context.
• Entry/exit wounds: in lightning, may be present but are often absent due to the flashover mechanism; when present, they are less clearly defined than in domestic electrocution
• Cause of death: cardiac arrest (VF), respiratory arrest, or blast injury; PM shows no specific internal finding except visceral congestion and non-specific asphyxia signs
Domestic / industrial electrocution:
Domestic current (220–240V AC at 50 Hz in India) is lethal primarily by causing ventricular fibrillation — the 50 Hz frequency is in the critical range that disrupts cardiac conduction. High-voltage industrial current may also cause respiratory muscle paralysis or massive thermal injury.
Key PM findings in electrocution:
• Electric mark (Joule burn, electrical entry mark): a small, oval, punched-out lesion with a pale or yellow-white centre and a surrounding red rim at the site of current entry. The pale centre is coagulation necrosis; the red rim is reactive hyperaemia. The central pallor distinguishes it from a simple thermal burn. A corresponding exit wound is found where the current left the body (typically the feet if the person was standing).
• The electric mark may be subtle, easily missed on casual inspection — a careful search of the body in all suspected electrocution cases is mandatory.
• Internally: no pathognomonic findings; VF leaves no specific PM sign; occasionally muscle necrosis along the current pathway
• Clothing may be scorched or burnt at the entry point
• Cause of death: VF (most common); respiratory muscle paralysis; thermal injury (high voltage); fall from height after shock
Medicolegal distinction: Lightning is almost always an accident (rarely homicidal). Domestic/industrial electrocution may be accident, suicide (rare — clutching live wires), or homicide (tampering with electrical safety devices, pushing a victim onto live wires, rigging a fatal 'booby trap'). The context, scene investigation, and technical examination of the electrical installation are critical.
Radiation Injuries
Acute Radiation Syndrome: Phase Timeline and Dose Thresholds
Radiation injuries in medico-legal practice are encountered in three main contexts: occupational exposure accidents (radiologists, nuclear plant workers), accidents involving radioactive sources (abandoned radiotherapy equipment, theft of industrial radioisotopes), and — rarely — deliberate use of radioactive material as a weapon (radioactive poisoning). A basic classification and understanding of acute radiation effects is necessary for the forensic physician to recognise this rare but distinctive category of death.
Types of radiation:
• Ionising radiation (sufficient energy to ionise atoms and break chemical bonds): alpha particles (low penetrance, dangerous internally), beta particles (moderate penetrance), gamma rays and X-rays (high penetrance, whole-body exposure). Ionising radiation damages DNA (double-strand breaks), proteins, and lipid membranes.
• Non-ionising radiation: ultraviolet (UV), microwave, infrared, radiofrequency. These cause thermal injury and some mutagenic effects (UV) but are much less acutely lethal than ionising radiation in typical exposures.
Acute radiation syndrome (ARS):
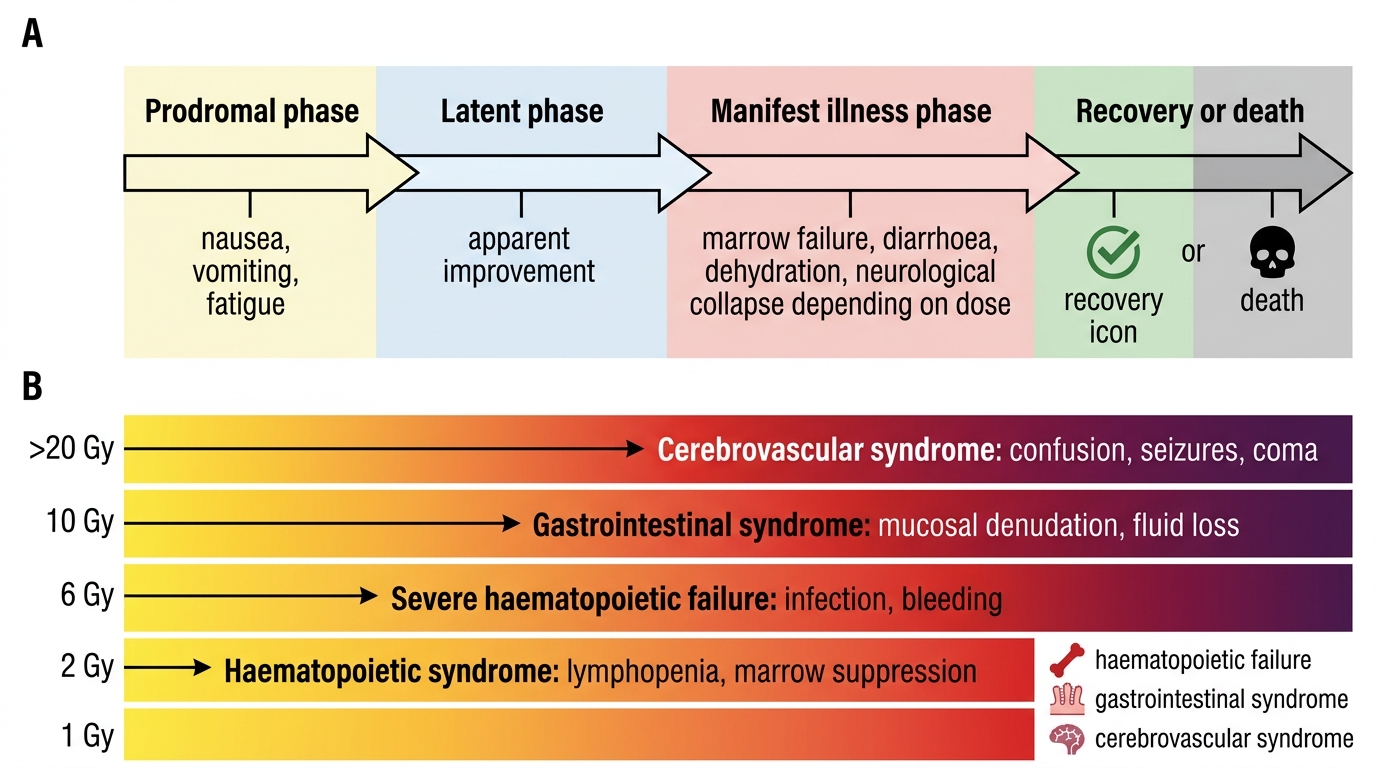
ARS follows whole-body exposure to high doses of ionising radiation. It progresses through four phases:
1. Prodromal phase (hours after exposure): nausea, vomiting, anorexia, diarrhoea — the 'initial response'; severity and onset time inversely correlate with dose (dose >1 Gy: vomiting within 3 hours is a reliable indicator of a significant exposure)
2. Latent phase (days to weeks): apparent improvement; bone marrow suppression is occurring silently; duration inversely proportional to dose
3. Manifest illness phase: bone marrow failure (doses 2–6 Gy) → pancytopenia, haemorrhage, infections; gastrointestinal syndrome (doses 6–10 Gy) → diarrhoea, haemorrhage, gut mucosal loss; cerebrovascular syndrome (doses >20 Gy) → cardiovascular collapse, cerebral oedema, death within days
4. Recovery or death: survival possible with medical support (bone marrow transplantation) at 2–6 Gy; doses above 6 Gy are generally lethal without aggressive haematological support; doses above 10 Gy are invariably lethal
PM findings in radiation deaths: Non-specific; depend on the dominant syndrome (haemorrhage throughout, gut mucosal necrosis, alopecia, skin erythema/desquamation). No pathognomonic autopsy sign; dosimetry reconstruction and biomarker analysis (chromosome aberrations in peripheral lymphocytes) are more important than PM morphology in establishing the dose.
ML context: Occupational exposure deaths require liaison with the Atomic Energy Regulatory Board (AERB) in India. Deaths from illicit radioactive sources may require involvement of national security agencies. Documentation of occupational radiation exposure records and dosimetry reports is as important as the PM examination.
Death from Starvation and Neglect
Provided image
Death from starvation and neglect occupies a distinct and ethically charged area of forensic medicine. It is encountered in two main contexts: children subjected to deliberate deprivation by caregivers (the most common medico-legal scenario in India, followed closely by elderly neglect), and individuals deprived of food and water in detention, captivity, or extreme poverty. The forensic physician must distinguish starvation from naturally occurring cachexia (cancer, tuberculosis, malabsorption) and document the findings with sufficient precision to support a case for criminal negligence or homicide.
Clinical progression of starvation:
Complete food deprivation causes death within 60–70 days in an adult (water deprivation causes death much sooner, within 3–5 days). The body passes through sequential phases of fuel mobilisation: glycogen stores (exhausted in 24 hours) → fat mobilisation (weeks, causing emaciation) → protein catabolism (muscles, viscera — the late, devastating phase). Progressive changes include:
• Weight loss, emaciation, loss of subcutaneous fat
• Weakness, apathy, mental deterioration
• In children: marasmus (severe weight loss, muscle wasting, wrinkled skin) or kwashiorkor (nutritional oedema from hypoproteinaemia) — important to distinguish from neglect-related starvation, though they may co-exist
• Late stage: peripheral oedema from hypoproteinaemia, ulcerations, hypothermia
• Death from cardiac arrhythmia, electrolyte imbalance, intercurrent infection, or cardiovascular failure
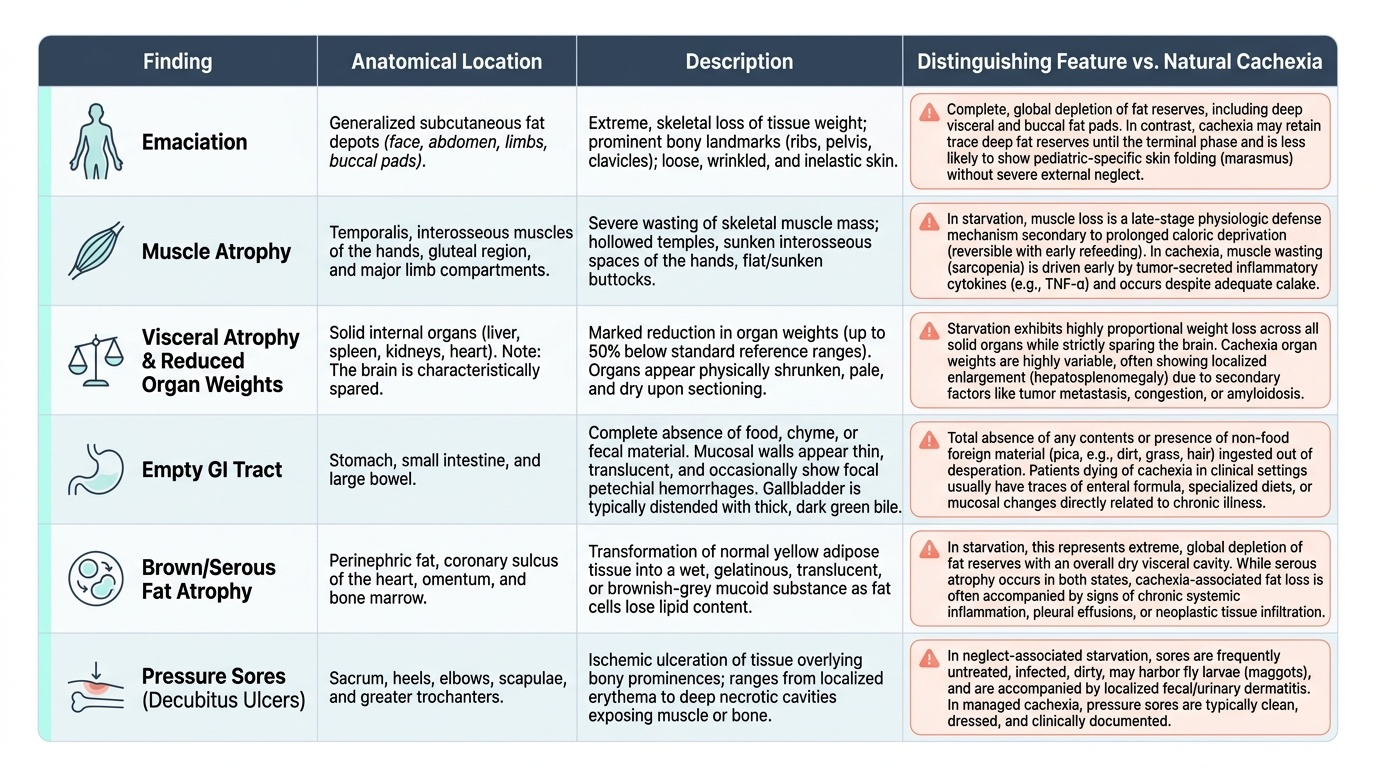
Post-mortem findings in starvation:
• Emaciation: skin and bone appearance; loss of all subcutaneous fat; skeletonised limbs
• Muscle atrophy: particularly temporal, gluteal, and limb muscles
• Visceral atrophy: liver, spleen, kidneys, adrenals — all markedly reduced in weight and size. The heart may also show atrophy. Organ weights below reference values for age/sex are documented.
• Gastro-intestinal tract: collapsed, thin-walled; virtually empty (no food residue); small intestine may show villous atrophy
• Skin: dry, wrinkled, inelastic, may show pressure sores (decubitus ulcers) in neglected persons confined to bed — these indicate both prolonged immobility and inadequate nursing care
• Fat: the stored neutral fat is brown or 'serous' (serosa appears as oily droplets under mesenteric serosal surfaces) in starvation, distinguishing it from normally-coloured white fat
• Distinguishing from natural cachexia (cancer, TB, malabsorption): a careful history, examination of the circumstances, and histological examination of tissues are required. Cancer cachexia will show a primary tumour or metastases. TB will show characteristic granulomata. Neglect starvation in a child with normal parents and access to food stands in sharp contrast to a bed-bound cancer patient.
ML framework for neglect deaths:
In India, criminal neglect leading to death is prosecuted under:
• IPC Section 304A (causing death by negligence) — for cases where the duty of care (parent, guardian, nurse, institution) existed and was breached, without specific intent to cause death
• IPC Section 302 (murder) — if evidence of deliberate deprivation with intent to cause death
• Juvenile Justice Act 2015 and Protection of Children from Sexual Offences Act (POCSO) 2012 provide additional framework for child victim cases; note that POCSO is primarily for sexual offences but the Juvenile Justice Act addresses child neglect and abuse comprehensively
• Maintenance of Parents and Senior Citizens Act 2007 — provides civil recourse for elderly neglect in India
Documentation: Measurement of all organ weights against standard tables, body weight, body mass index estimate (arm circumference as proxy), photographs of emaciation, and detailed scene investigation (was food available? was the person confined?) are essential.
SELF-CHECK
A body is found in a house fire. Post-mortem examination shows the body is in a flexed 'boxing' posture with charred skin. Histological examination of the burn margin shows no leucocytic infiltration, no vascular congestion, and thin watery blister fluid. The trachea is clean, and blood carboxyhaemoglobin is 2%. These findings most strongly suggest:
A. The victim was alive during the fire and died from smoke inhalation
B. The pugilistic attitude indicates the victim was fighting for their life
C. The victim was likely dead before the fire started (post-mortem burns)
D. The fire was too rapid for a vital reaction to develop
Reveal Answer
Answer: C. The victim was likely dead before the fire started (post-mortem burns)
The combination of absent vital reaction (no leucocytic infiltration, no hyperaemia, thin watery non-protein-rich blister fluid), normal/low carboxyhaemoglobin (2% — below any threshold of significant exposure), and clear trachea (no soot) indicates that the victim was NOT breathing during the fire, i.e., was likely dead before the fire started. The pugilistic attitude is a post-mortem heat artefact caused by muscle protein coagulation — it does NOT indicate ante-mortem activity. A forensic opinion should state that findings are consistent with post-mortem exposure to fire, raising the possibility that fire was used to conceal the actual cause of death.