Page 8 of 17
FM3.4 | Drowning — SDL Guide
Learning Objectives
- Describe the types of drowning and explain the pathophysiology of each
- Distinguish freshwater from saltwater drowning by mechanism and haemodynamic effects
- Describe the clinical features and post-mortem findings of drowning in systematic sequence
- Explain the principles, procedure, and limitations of the diatom test and Gettler's chloride test
- Discuss the medicolegal aspects of drowning: ante-mortem vs post-mortem immersion, manner of death, and documentation
INSTRUCTIONS
Drowning is a leading cause of unnatural death in India, particularly among children under five and young adults in states with major water bodies. A body recovered from water presents forensic challenges distinct from land-based deaths: the water alters and obscures many PM signs, introduces ambiguity about timing, and the question 'did the person drown, or were they already dead when placed in the water?' is critically important. This module equips you to answer that question systematically.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old male student is found floating face-down in a river at dawn near a college campus. His friends report he had attended a party the previous evening and had not been seen since midnight. When the body is retrieved, the police constable notices persistent white froth around the mouth and nostrils, and the skin of the palms and soles appears wrinkled and pale like a washerwoman's hands. The duty doctor at the mortuary is asked: 'Was he alive when he entered the water, or was he already dead?' The answer to that question may be the difference between a tragic accident and a murder charge. How does the forensic physician approach this question?
WHY THIS MATTERS
Drowning is the third leading cause of unintentional injury death globally (WHO) and a significant cause of both accidental and homicidal death in India. The forensic physician investigating a drowning death faces a specific and practically important challenge: the medium itself — water — confounds many standard PM signs. External injuries may be from watercraft, river fauna, or ante-mortem violence. The body may have decomposed substantially. The central medicolegal question — was drowning the cause of death, or was the body disposed of in water after death? — can have profound legal consequences. This module builds the scientific framework to approach that question using the PM examination, forensic tests, and scene evidence.
RECALL
Recall from Year-1 Physiology:
- Osmosis: Water moves from a hypotonic environment into cells (freshwater) or from cells into a hypertonic environment (saltwater). Apply this to alveolar–capillary interface when water enters the lungs.
- Haemolysis: Hypotonic solutions cause red cell lysis; hypertonic solutions cause crenation (cell shrinkage). In freshwater drowning, absorbed water dilutes the blood — what happens to the red cells?
- Cardiac arrhythmia: Hyperkalaemia from haemolysis, or haemodilution lowering plasma electrolytes, can trigger ventricular fibrillation. What are the electrolyte triggers for VF?
Recall from as1-asphyxia: the general PM signs of asphyxia (Tardieu spots, cyanosis, fluid blood) — these are also present in drowning, but modified by the water exposure.
Pathophysiology of Drowning
Drowning is defined by the World Health Organization (2002) as a process resulting in primary respiratory impairment from submersion or immersion in a liquid medium. The definition specifically requires that the liquid medium — not another cause — is the primary factor in respiratory impairment. This definition has important forensic implications: a person can drown in as little as 2 cm of water (as in elderly people found face-down in a bath).
Drowning is classified by the physiological mechanism, and understanding this classification is prerequisite to interpreting PM findings:
Wet drowning (~85–90% of cases): Water is aspirated into the airways. As the victim submerges and cannot breathe, the involuntary struggle leads to aspiration of large quantities of water into the lungs. The lungs are markedly over-distended and waterlogged. This is by far the most common type.
Dry drowning (~10–15% of cases): When water first touches the larynx, a powerful and sustained laryngospasm occurs reflexively. The glottis remains closed; no water enters the lungs. Death occurs from asphyxia — the closed glottis prevents any air exchange, and cerebral hypoxia progresses to death. At PM, the lungs are dry — this is the diagnostic clue. Dry drowning is more likely when the water is very cold (intense laryngeal reflex) or in certain individuals with a hypersensitive laryngeal reflex.
Secondary drowning (near-drowning delayed death): A victim is rescued alive but later deteriorates and dies from delayed pulmonary oedema (also called 'delayed drowning'). The initial aspiration of water, even in small quantities, triggers surfactant loss, alveolar collapse, and a severe inflammatory response over 1–24 hours that produces acute lung injury. Clinical relevance: a rescued drowning victim must be observed for ≥24 hours even if initially well.
Immersion syndrome (not true drowning): Sudden immersion in cold water triggers reflex vagal cardiac arrest — the victim dies from cardiac arrest before significant aspiration occurs. The face and hands are pale; there is minimal water in the lungs at PM. This is considered a separate entity from drowning by some authorities.
Freshwater vs saltwater drowning — haemodynamic differences:
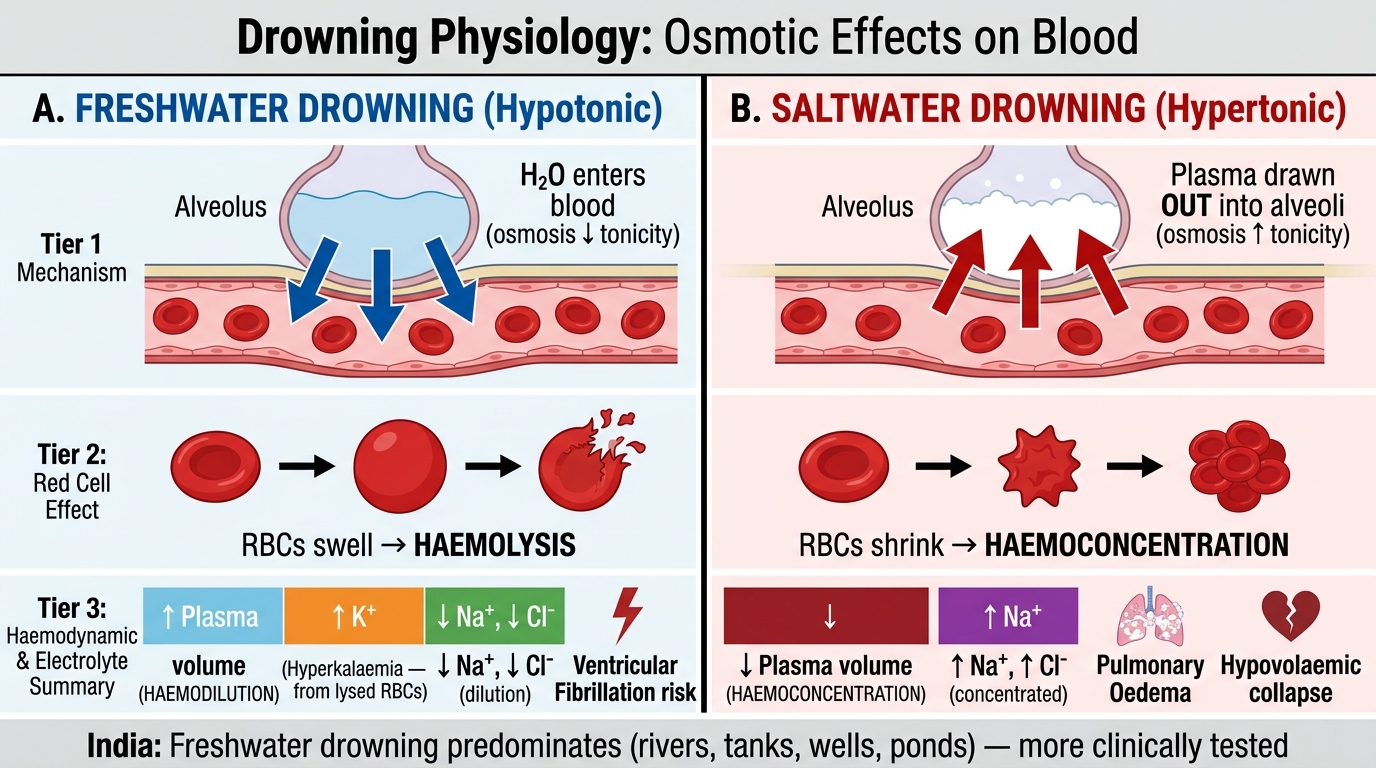
Freshwater vs Saltwater Drowning: Osmotic Mechanisms and Haemodynamic Consequences
Freshwater is hypotonic relative to plasma. When absorbed in large quantities through the alveolar membrane, it enters the pulmonary capillaries and causes:
• Haemodilution (plasma volume expands)
• Haemolysis (red cells swell and lyse in hypotonic plasma)
• Hyperkalaemia (from lysed red cells releasing intracellular potassium)
• Ventricular fibrillation triggered by the hyperkalaemia and haemodilution
• The blood becomes dilute and haemolysed — the left heart blood is less chloride-rich than the right (freshwater diluting the pulmonary venous return)
Saltwater is hypertonic. When absorbed, it draws plasma fluid into the alveoli, causing:
• Haemoconcentration (plasma volume decreases)
• Pulmonary oedema from plasma drawn into alveolar spaces
• Hypovolaemia and cardiovascular collapse
• The alveoli fill with protein-rich plasma fluid — frothy, blood-tinged
• The right heart blood is more dilute (saltwater diluting it) while left heart blood is more concentrated
In India, most drowning occurs in freshwater (rivers, tanks, wells, ponds), so freshwater drowning physiology is more commonly tested and clinically relevant.
Post-Mortem Findings in Drowning
The PM examination of a drowning victim follows a systematic external-to-internal sequence. Water modifies many of the findings over time, and the completeness of the findings depends on how soon after death the body is examined and whether it has been in moving versus still water.
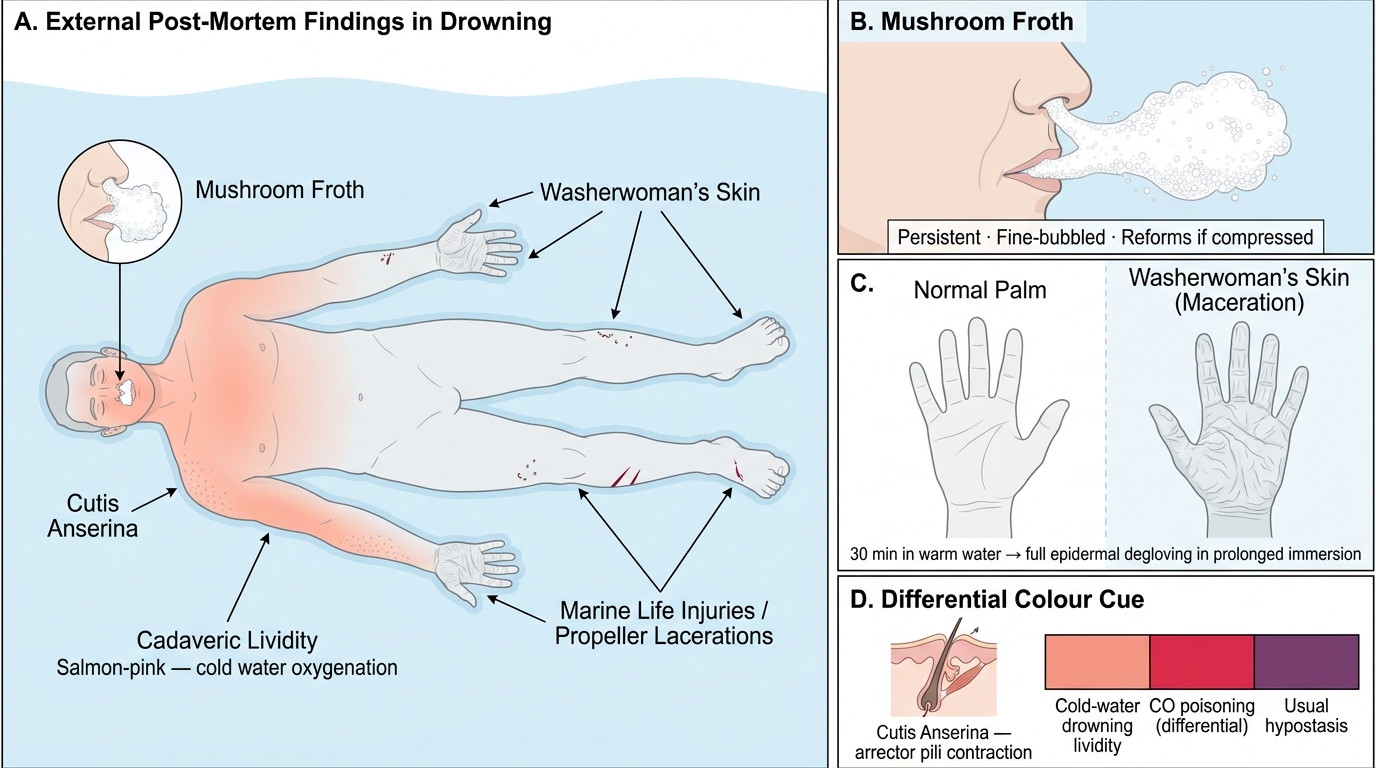
External Post-Mortem Findings in Drowning
External findings:
- Mushroom froth (froth at nose and mouth): Persistent, fine-bubbled, white, voluminous froth at the nostrils and lips — one of the most characteristic findings of drowning. Formed by the churning of air, water, and airway secretion during drowning. It is persistent (unlike agonal foam, which disperses quickly) and may extend several centimetres from the orifices. It can reform if compressed. Absent in dry drowning and in post-mortem immersion.
- Washerwoman's skin (maceration): Pale, sodden, wrinkled skin of the palms and soles — the classical 'washerwoman's hands/feet'. Develops within 30 minutes of immersion in warm water and much more slowly in cold water. After prolonged immersion, the entire epidermis may detach ('degloving'). Not specific to drowning (occurs with any prolonged water exposure).
- Cutis anserina (goose skin): Erection of hair follicles producing a 'goosebump' appearance, due to post-mortem contraction of arrector pili muscles in cold water. Not specific to drowning.
- Cadaveric lividity: Pale pink ('salmon-pink') in cold water, due to oxygenation of haemoglobin from the cold water environment — may falsely suggest carbon monoxide poisoning. Lividity appears on the front of the body if floating face-down.
- Injuries: Marine life bites (post-mortem), contact with rocks or watercraft propellers, ante-mortem injuries from struggle or assault — all must be documented and distinguished.
Internal findings:
- Emphysema aquosum (over-inflated, waterlogged lungs): The lungs in wet drowning are markedly over-distended, pale or mottled, oedematous, pitting, and heavier than normal (normal lung weighs ~400 g each; drowning lung can exceed 1,000 g). Pressing the cut surface exudes watery fluid. Paltauf's haemorrhages: pale, yellowish subpleural haemorrhages resulting from rupture of overdistended alveoli.
- Water in the stomach: Small to moderate quantities of water, aquatic vegetation, sand, diatoms, or algae swallowed during drowning — absent in post-mortem immersion.
- Frothy fluid in airways: Water and froth in the trachea, bronchi, and bronchioles.
- General asphyxial signs: Tardieu spots, fluid dark blood (though saltwater drowning may produce more viscous blood), visceral congestion — modified by water exposure.
- Diatoms: Microscopic algae with silica cell walls — their presence in the bone marrow, liver, kidney, or brain (beyond the lungs) indicates vital circulation carrying them from the alveoli into the bloodstream — i.e., ante-mortem drowning.
SELF-CHECK
Which post-mortem finding most reliably suggests that the victim was alive (ante-mortem) when entering the water, rather than having been placed in the water after death?
A. Washerwoman's skin of the palms and soles
B. Mushroom froth at the mouth and nostrils
C. Diatoms found in the bone marrow or liver
D. Cutis anserina (goose skin)
Reveal Answer
Answer: C. Diatoms found in the bone marrow or liver
Washerwoman's skin, mushroom froth, and cutis anserina can all develop post-mortem after immersion (froth can form post-mortem in some circumstances, and skin maceration occurs with any prolonged water exposure). Diatoms in the bone marrow or distant organs (liver, kidney, brain) are powerful evidence of vital circulation — they require the heart to be beating during aspiration to carry the diatoms from the alveolar capillaries into the systemic circulation and ultimately to distant organs. A body placed in water after death may have diatoms in the lungs (passive entry) but NOT in the bone marrow or distant organs. This is the basis of the diatom test as evidence of ante-mortem drowning.
Forensic Tests for Drowning
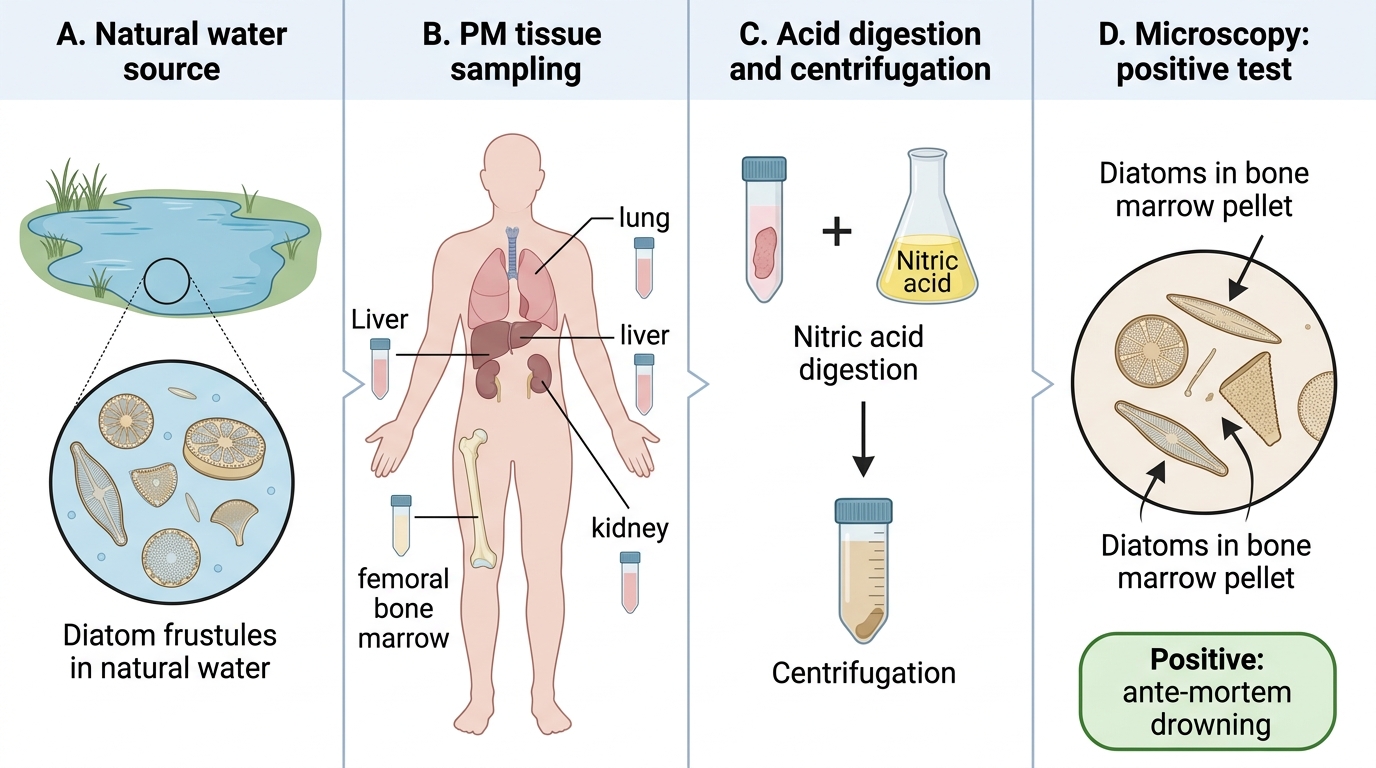
Diatom Test Procedure in Suspected Drowning
Because PM findings alone may not confirm drowning — especially in decomposed or dry-drowning cases — several forensic tests have been developed to supplement the PM examination. Of these, the diatom test is the most widely accepted and the most forensically robust.
Diatom test (Incardona test):
Diatoms are unicellular photosynthetic algae with intricate silica cell walls (frustules) that are resistant to acid digestion and decomposition. They are found in virtually all natural water bodies, with characteristic species compositions that differ by location and season. During wet drowning, the aspirated water carries diatoms across the alveolar-capillary membrane into the pulmonary circulation. Because the left ventricle continues to pump for a minute or two after the onset of drowning asphyxia, these diatoms are distributed systemically — reaching the bone marrow, liver, kidney, and brain. This requires vital circulation and therefore indicates that the victim was alive during the aspiration event.
Procedure: Tissue samples from the lungs, bone marrow (femoral shaft, sternum), liver, and kidney are taken at PM. They are digested in concentrated nitric acid, centrifuged, and the pellet is examined under the microscope for diatom frustules.
Positive result: Diatoms in bone marrow and/or distant organs (liver, kidney, brain) — strongly suggests ante-mortem drowning.
Limitations of the diatom test:
1. Diatoms in drinking water: In areas where tap water contains diatoms (filtered but not sterilised), diatoms may be present in the lungs or even gut of any recently deceased person — not just drowning victims. A control sample from the local water supply should always be examined in parallel.
2. False negative: Decomposition, dry drowning (no water aspirated), or drowning in diatom-poor water (well water, heavily treated water) can give a negative result. A negative diatom test does NOT exclude drowning.
3. Species match: The diatom species found in the tissues should ideally match the species in the water body where the victim was found. A mismatch can suggest drowning at a different location.
4. Contamination: Meticulous technique is required to avoid environmental diatom contamination.
Gettler's chloride test (blood electrolyte method):
Proposed by Charles Norris and Alexander Gettler in the 1920s, this test exploits the differential dilution/concentration of chloride ions in blood from the left and right heart chambers:
• Freshwater drowning: Large volumes of hypotonic water are absorbed from the pulmonary alveoli into the pulmonary veins and returned to the left heart. The left heart blood is therefore more dilute — its chloride concentration is lower than that of the right heart blood.
• Saltwater drowning: The hypertonic saltwater draws plasma into the alveoli, concentrating the blood remaining in the pulmonary veins. The left heart blood has higher chloride concentration than the right.
• In post-mortem immersion (body placed in water after death): No circulation occurs, so no differential dilution develops — both chambers have similar chloride levels.
Limitations: The test has significant limitations — post-mortem ion redistribution between cardiac chambers begins within hours of death and can confound the results. It is now regarded as a supplementary historical test rather than the primary forensic test; the diatom test has largely superseded it in modern forensic practice. However, its principle is important for examinations and understanding the physiology of drowning.
Other tests: Lung float test (Ploucquet): whether the lungs sink or float in water — based on air content. Less reliable than diatom test. Haematological tests for haemolysis and electrolytes — useful in fresh cases.
Medicolegal Aspects of Drowning
Provided image
The forensic investigation of drowning is built around three core medicolegal questions, each with a different evidence base and each carrying different legal implications.
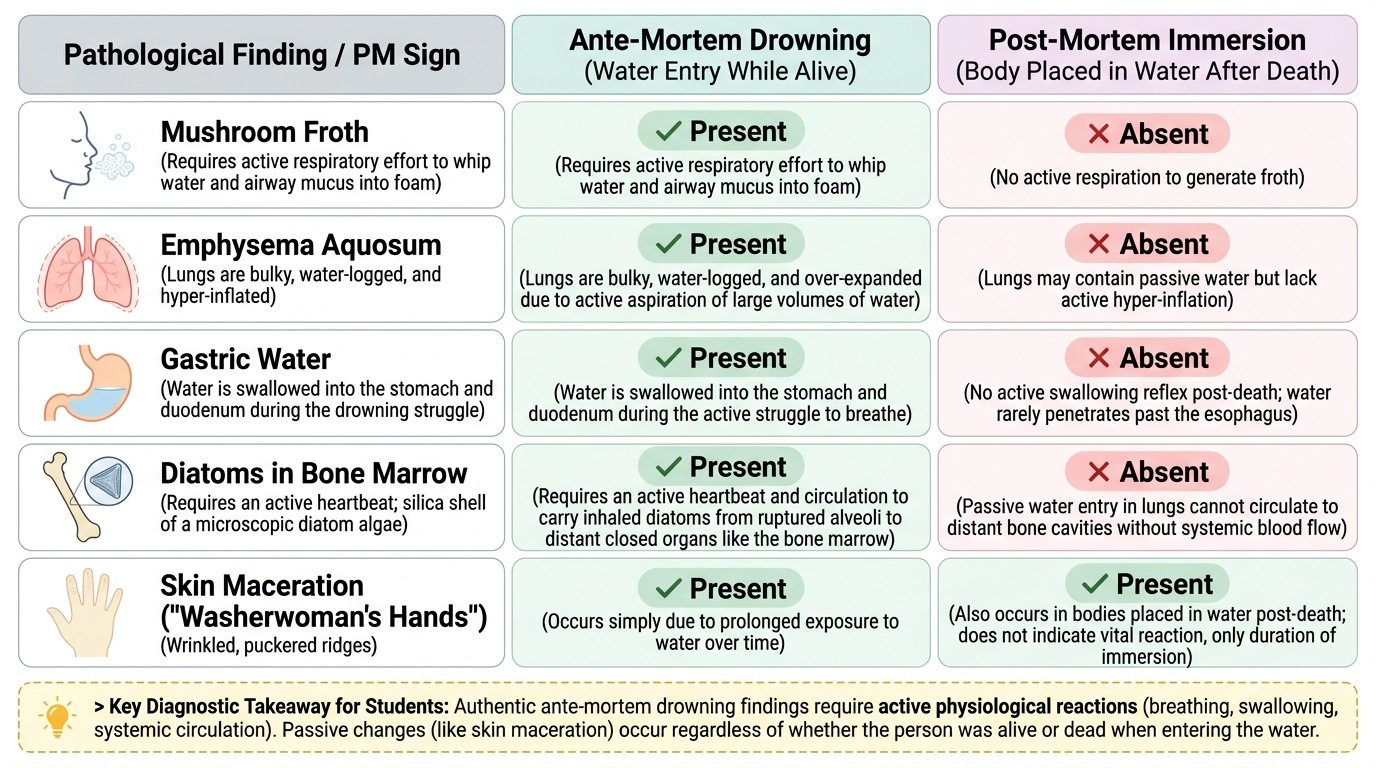
- Was the victim alive when they entered the water (ante-mortem immersion) or was the body placed in water after death (post-mortem immersion)?This is the most critical ML question. Evidence of vital reaction in the water: •Mushroom froth— requires active respiratory effort to form; absent in post-mortem immersion •Emphysema aquosum— requires living respiratory effort to aspirate such large volumes •Water in the stomach and gut— swallowed during drowning struggle; absent post-mortem •Diatoms in bone marrow and distant organs— requires ante-mortem circulation (see above) •Signs of struggle: skin injuries consistent with ante-mortem trauma, defensive wounds •Gettler's chloride differential — if early case and results reliable
Post-mortem immersion will show: generalised water maceration (washerwoman skin), no froth, collapsed or normal lungs (not emphysematous), no gastric water, possible cause of death evident elsewhere (stab wound, gunshot, blunt head injury hidden under decomposition).
2. What was the manner of death?
• Accident: the most common manner in India; associated with non-swimming children, festive bathing, alcohol intoxication (blood alcohol level from vitreous humour if available), epileptic seizure, or misjudgement of depth/current
• Homicide: evidence of restraint (wrists tied, weighted object attached), ante-mortem injuries inconsistent with accidental drowning, witness accounts; infant drowning (bathtub drowning) is a critical homicide scenario
• Suicide: a history of mental illness or suicidal ideation, multiple entries into the water noted at scene; suicide notes; weighted objects deliberately attached to oneself are rare
• Undetermined: when decomposition has obliterated findings and no circumstantial evidence is available
3. Was the drowning associated with alcohol or drug intoxication?
Alcohol is a significant contributing factor in a substantial proportion of accidental drowning deaths in Indian forensic series. Alcohol impairs swimming ability, judgment, and thermoregulatory capacity. Blood for alcohol estimation should be taken from the femoral vein (peripheral blood) at PM. In decomposed cases, vitreous humour or urine provides less confounded alcohol levels.
Documentation requirements:
• Systematic external examination including all injuries, with photography
• Internal examination including lung weights, froth, stomach contents
• Tissue samples for diatom test (bone marrow, liver, kidney, lung) — must be collected at initial PM, not later
• Blood samples for toxicology (alcohol, drugs) before any contamination
• Documentation of water temperature, salinity/freshwater character, flow conditions at the recovery site — this contextualises the diatom species match and decomposition timeline
Infant drowning deserves special mention: bathtub drowning in infants (<3 years) is a well-recognised presentation of child abuse. Typically the infant is held face-down in a small amount of water. The PM may show perioral bruising, bruises from restraint, and drowning signs. Accidental drowning in infants typically requires enough water to allow full submersion. The forensic physician should refer to child safeguarding authorities if the clinical history is implausible.
SELF-CHECK
A body is found floating in a pond. Post-mortem examination shows no mushroom froth, lungs that are collapsed and of normal weight, a stab wound on the back, and generalised skin maceration. Which conclusion is most strongly supported?
A. Wet drowning in the pond, with secondary decomposition
B. Dry drowning with laryngospasm
C. The victim likely died of the stab wound before entering the water (post-mortem immersion)
D. Secondary (near-drowning) delayed pulmonary oedema
Reveal Answer
Answer: C. The victim likely died of the stab wound before entering the water (post-mortem immersion)
The absence of mushroom froth, collapsed lungs of normal weight (no emphysema aquosum), and a stab wound point to a cause of death other than drowning, with the body subsequently placed in water. Wet drowning would produce emphysematous, waterlogged lungs and froth. Dry drowning would show dry, collapsed lungs but typically in the context of cold-water immersion and without a stab wound as an alternative cause of death. The generalised maceration is consistent with prolonged water immersion after death, not ante-mortem drowning. This scenario illustrates 'drowning as disposal of a body' — a homicide.
CLINICAL PEARL
Take bone marrow for the diatom test at the initial PM — not later. The diatom test requires intact tissue samples from the femoral bone marrow, liver, kidney, and lung. Once the body has been released and reassembled, the opportunity to sample pristine marrow is gone. Even in a case initially considered a straightforward accidental drowning, preserve samples: if the manner of death is later contested and the samples were not taken, no test can establish ante-mortem drowning. The mantra: 'Collect first, decide later.'
KEY TAKEAWAYS
Drowning is defined as respiratory impairment from submersion in a liquid medium. Types include wet drowning (~85–90%, water aspirated), dry drowning (~10–15%, laryngospasm, dry lungs at PM), secondary (near-) drowning (delayed pulmonary oedema hours after rescue), and immersion syndrome (vagal cardiac arrest in cold water).
Freshwater aspiration causes haemodilution, haemolysis, and hyperkalaemia leading to ventricular fibrillation. Saltwater aspiration causes haemoconcentration and pulmonary oedema from plasma drawn into alveoli. Most Indian drowning is freshwater.
PM findings include mushroom froth (characteristic, requires vital respiratory effort), washerwoman's skin (non-specific, occurs post-mortem too), emphysema aquosum (waterlogged, over-distended lungs), cutis anserina, and gastric water. The diatom test — finding diatoms in bone marrow or distant organs — is the most forensically robust test for ante-mortem drowning; a positive result requires vital circulation. Gettler's chloride test is a historical supplementary method.
The central medicolegal question is whether death preceded or followed water entry. Positive vital reaction evidence (froth, emphysema aquosum, gastric water, diatoms in distant organs) points to ante-mortem drowning. The manner of death — accident, homicide, or suicide — is determined from the PM findings, scene investigation, and circumstantial evidence.
REFLECT
The hook scenario: the forensic medical officer must answer whether the young student was alive when he entered the river. He plans to collect tissue samples for the diatom test and blood for alcohol. But the family insists there is 'no way' he drowned accidentally — they believe he was killed and disposed of. The police ask if the PM findings can establish this. Reflect on what findings at PM would support versus refute the claim that this was a homicide with post-mortem immersion. What are the limitations of the available forensic tests? What will you include in your PM report to clearly frame what the evidence can and cannot say?