Page 5 of 17
FM3.2 | Hanging & Strangulation — SDL Guide
Learning Objectives
- Describe the types of hanging, mechanisms of death, and characteristic post-mortem findings
- Describe the PM findings and distinguishing features of ligature strangulation and throttling
- Differentiate hanging from strangulation and throttling using PM and scene findings
- Explain the correct procedure for examination, preservation, and dispatch of ligature material
- Discuss the medicolegal aspects of manner-of-death determination in neck compression deaths
INSTRUCTIONS
Hanging is the most common method of suicide in many Indian states, and strangulation deaths are among the most forensically contested homicides in criminal courts. The distinctions between hanging, ligature strangulation, and throttling are medico-legally critical — they can determine whether a death is classified as suicide or murder under IPC Section 302. This module equips you with the precise PM criteria, examination sequence, and legal framework to give defensible expert testimony.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman is found suspended from a ceiling hook in her matrimonial bedroom at 6 AM. Her husband calls the police, stating he woke up and found her. The body is still warm. The rope loops once around the neck, the knot is at the right side, and the face is pale rather than congested. The police constable at the scene remarks: 'Clearly suicide.' The forensic medical officer arrives and notices the ligature mark is horizontal and at the level of the thyroid cartilage, not oblique. There are scattered petechiae on both conjunctivae and faint fingernail abrasions on the front of the neck. What does the medical officer note, and why might 'clearly suicide' be premature?
WHY THIS MATTERS
Hanging accounts for the largest single proportion of suicide cases in India, particularly in rural areas. Strangulation homicides — whether by ligature or hands — are the second most common cause of homicidal death after sharp-force injuries in several Indian forensic series. The ability to distinguish hanging from ligature strangulation from throttling is therefore the single most practically consequential skill in forensic medicine, directly determining whether a case proceeds as suicide, accident, or murder under IPC Section 302. Errors — certifying a strangulation homicide as a suicidal hanging — represent one of the gravest failures a forensic physician can make. This module teaches you to read the neck, read the scene, and interpret the ligature evidence with precision.
RECALL
Recall from Year-1 Anatomy:
- Neck structures: hyoid bone (at C3), thyroid cartilage (C4-5), cricoid, trachea, carotid arteries, jugular veins. The relationship of the ligature mark to the thyroid cartilage is the single most important positional clue in differentiating hanging from strangulation.
- Jugular veins are valveless: this explains the rapid facial congestion when venous return is obstructed.
- From Year-1 Physiology: the carotid sinus at the bifurcation of the common carotid (C3-4 level). Stimulation causes reflex bradycardia and vasodilation — this is the basis of vagal cardiac arrest in hanging and strangulation.
Recall from the previous SDL (as1-asphyxia): the four stages of asphyxia, general PM signs, and the concept that the mechanism of death in neck compression is multi-factorial.
Mechanism of Death in Hanging
Mechanisms of Death in Hanging
Hanging is defined as a form of asphyxia caused by suspension of the body by a ligature applied around the neck, where the compressing force is the weight of the body itself. This distinguishes it fundamentally from strangulation, where an external force is applied by another person (or, rarely, the victim in an unusual position). The mechanism of death in hanging is not simply 'airway obstruction' — it is multi-factorial, and the relative contribution of each mechanism depends on the type of hanging.
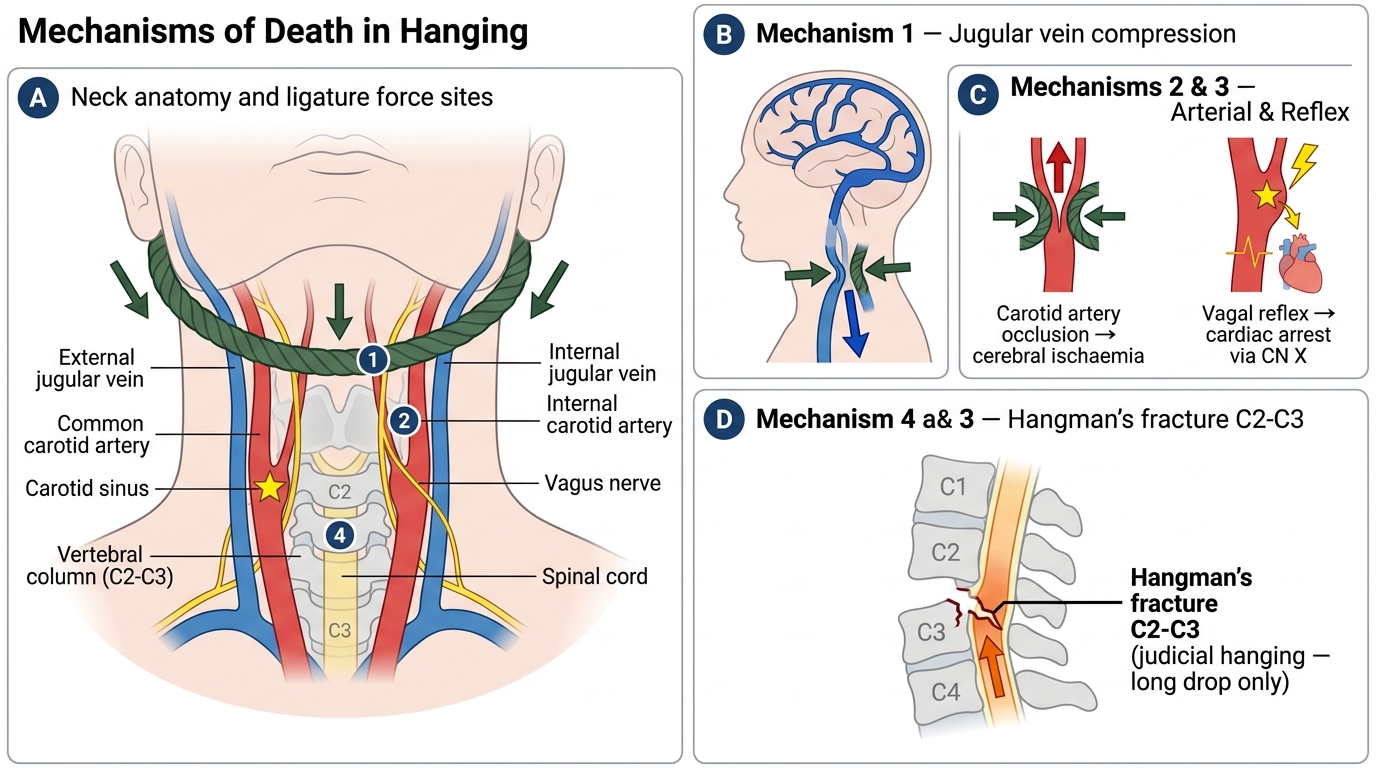
Four mechanisms contribute to death in hanging, typically acting in combination:
1. Obstruction of venous return (dominant in most cases): The ligature compresses the jugular veins, preventing blood from draining from the cranial vault. Arterial supply continues (carotid arteries require greater pressure to compress), leading to a progressive rise in intracranial venous pressure, cerebral oedema, and ultimately hypoxic unconsciousness within seconds to minutes. This is the dominant mechanism in typical hanging.
2. Arterial compression: Both carotid arteries can be occluded by the ligature in typical hanging, adding an ischaemic component to the hypoxia. The vertebral arteries, protected by the cervical spine, are less easily compressed.
3. Vagal inhibition (reflex cardiac arrest): Sudden stimulation of the carotid sinus or the vagi by the ligature can trigger reflex bradycardia and cardiac arrest. This explains why some hanged individuals show no asphyxial PM signs at all — death was too rapid for the congestion and petechiae to develop.
4. Fracture-dislocation of the cervical spine (occurs in judicial/long-drop hanging only): The deliberate long drop (calculated to produce a sudden decelerating force proportional to body weight) fractures and dislocates C2 on C3 — the 'hangman's fracture' — severing the spinal cord at the level of the respiratory centres. This is the intended humane mechanism in judicial execution because it produces instant death. It does NOT occur in suicidal or accidental hanging (which typically involves a short drop or suspension without a fall).
Types of Hanging and Post-Mortem Findings
Hanging is classified in two intersecting ways — by whether the body is fully or partially suspended, and by the geometry of the suspension point relative to the knot. These distinctions matter because they affect both the mechanism of death and the expected PM findings.
Classification by suspension:
• Complete/typical hanging: The entire body weight is borne by the ligature; feet are entirely off the ground. The full weight compresses the neck vessels, accelerating unconsciousness.
• Incomplete/atypical hanging: Part of the body rests on a surface (kneeling, sitting, lying). Despite the partial weight, the neck compression is sufficient to compress the jugular veins and carotid arteries and cause death. Many suicidal hangings in India are incomplete — the individual finds a low attachment point (bed-post, door handle, window grill) and simply leans forward. Incomplete hanging is equally lethal.
Classification by knot position (affects ligature mark pattern):
• Typical hanging (central/anterior knot): Knot below chin, rope diverges laterally and posteriorly over the neck, ligature mark is highest laterally and lowest anteriorly — classically described as an inverted-V or U-shape from the front.
• Atypical hanging (knot at side or back): Knot at the side (most common in suicidal hanging) or posterior; mark is oblique and asymmetric.
Hanging vs. Ligature Strangulation — Ligature Mark Comparison
The ligature mark in hanging — five key features:
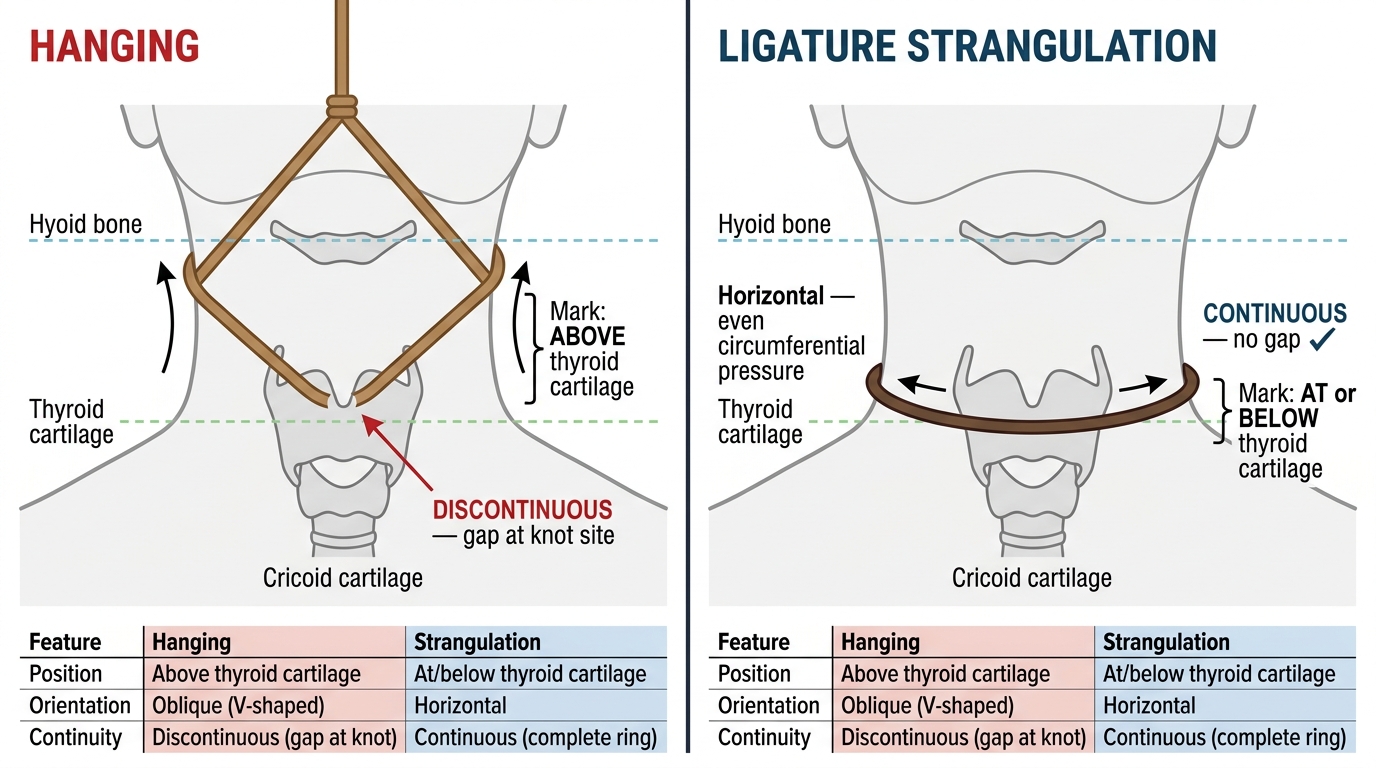
1. Position: ABOVE the thyroid cartilage (typically at the level of the larynx or higher), because the neck rope rides upward under body weight
2. Orientation: OBLIQUE — highest at the sides and back, lowest at the knot; directed upward toward the point of suspension
3. Continuity: DISCONTINUOUS — there is a gap at the knot site where the skin is not compressed
4. Texture: Parchment-like — dry, brownish, hard, abrasive — from skin compression and post-mortem drying (not a vital reaction, this forms rapidly post-mortem)
5. Pattern: May reflect the weave or pattern of the ligature material
Other PM findings in hanging:
• Face: May be pale (if complete hanging with good carotid compression) or congested with petechiae (if incomplete, or if venous obstruction predominated). Pallor is more common in typical/complete hanging; congestion with Tardieu spots in incomplete or atypical.
• Subconjunctival petechiae if venous phase predominated
• Protrusion of tongue, froth at mouth
• Neck dissection: performed at PM — shows haemorrhage in strap muscles, bruising around the carotid sheaths, and rarely thyroid cartilage fracture (more common in elderly)
• Hyoid fracture: occurs in a minority; more common in the elderly (ossified hyoid) and in throttling than in hanging
• Fracture-dislocation C2-C3: only in judicial hanging
SELF-CHECK
In a typical suicidal hanging, what is the expected position and orientation of the ligature mark on the neck?
A. Below the thyroid cartilage, horizontal, continuous around the neck
B. Above the thyroid cartilage, oblique, discontinuous at the knot
C. At the thyroid cartilage, vertical, with bilateral symmetry
D. Below the thyroid cartilage, oblique, continuous at the knot
Reveal Answer
Answer: B. Above the thyroid cartilage, oblique, discontinuous at the knot
In hanging, the body weight causes the rope to ride upward, so the ligature mark forms ABOVE the thyroid cartilage (distinguishing it from strangulation, where the mark is at or below). Because the rope converges upward toward the suspension point, the mark is OBLIQUE — highest at the sides/back, lowest anteriorly. There is a GAP (discontinuity) at the knot site because the skin is not compressed there. These three features — position above thyroid cartilage, oblique orientation, and discontinuity at knot — together distinguish hanging from ligature strangulation.
Strangulation by Ligature: Mechanism and PM Findings
Ligature Strangulation — Post-Mortem Neck Findings and Comparison with Hanging
Ligature strangulation differs from hanging in a single, legally critical way: the compressing force is applied by another person (or, very rarely, by the victim in an unusual fixed-ligature position), not by the weight of the body. The ligature is tightened by a human hand, a twisted stick (garrotte), or a mechanical device. The victim is typically lying, sitting, or kneeling — not suspended.
The mechanism of death is identical to hanging — jugular vein compression → cerebral venous hypertension → hypoxia — but because the body weight is not involved, the dynamics of neck compression differ, and the PM findings reflect these differences clearly.
The ligature mark in ligature strangulation — distinguishing features vs hanging:
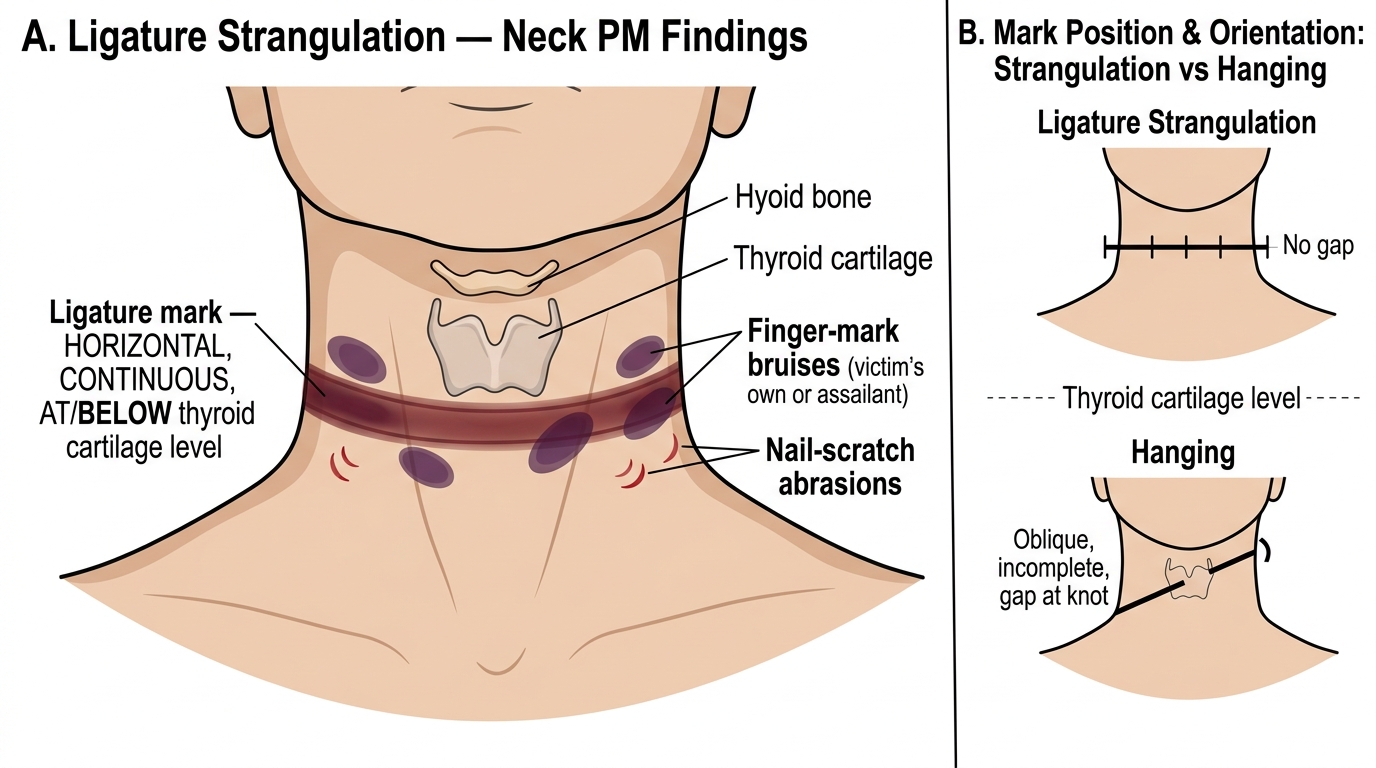
1. Position: AT or BELOW the level of the thyroid cartilage — because the applied ligature sits at the mid-neck level, not pulled upward by gravity
2. Orientation: HORIZONTAL — running transversely around the circumference of the neck
3. Continuity: CONTINUOUS — because the ligature encircles the entire neck evenly, without a gap; there is typically no 'knot gap'
4. Character: The mark may show impression of the ligature weave/pattern; it is firmer and deeper than in hanging because active force was applied
5. Superimposed signs: Evidence of a struggle may include peripheral bruising, satellite abrasions, or nail marks near the ligature mark from the victim's attempts to remove it
Additional PM findings in ligature strangulation:
• Marked facial congestion, cyanosis, and petechiae — more prominent than in typical hanging because the victim struggles longer before losing consciousness
• Bilateral prominent subconjunctival haemorrhages
• Evidence of struggle: defence wounds on the hands (nail marks, abrasions from grabbing the ligature), bruising on the limbs from restraint
• Internal neck dissection: bruising of the strap muscles, laryngeal cartilage fracture (more common than in hanging), hyoid fracture possible
• Haemorrhage in the carotid sheath: from vessel compression under active force
It is almost always homicide in adults. Suicide by ligature strangulation is extremely rare (one would need to maintain tension while losing consciousness — physiologically near-impossible without a fixed mechanism). Every ligature strangulation in an adult must be investigated as a homicide until proven otherwise.