Page 7 of 18
FM2.{20,24,26} | Special-Situation Autopsies: Custody, Negligence & Anaesthetic Deaths — SDL Guide
Learning Objectives
- Describe special protocols for autopsies in cases of death in custody and human rights violations per NHRC guidelines (FM2.20)
- Describe investigation of anaesthetic and operative deaths — special protocols, collection and preservation of material evidence (FM2.24)
- Demonstrate ability to work in a team for medico-legal autopsies in negligence, dowry death, and custody cases per NHRC guidelines (FM2.26)
INSTRUCTIONS
Certain categories of death carry an added dimension of institutional accountability and public scrutiny that demands protocols beyond the standard medico-legal autopsy. Deaths in police custody, deaths during anaesthesia, and deaths attributed to medical or institutional negligence are not merely clinical events — they are potential sites of systemic failure or criminal conduct by those in positions of trust. The enhanced protocols for these cases exist because the ordinary autopsy framework, while thorough, was designed primarily to investigate deaths in the community, not deaths that may implicate the state or the healthcare system. This module builds your competence in navigating these heightened-stakes scenarios.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed., Ch. 5, 7 (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed., Ch. 6, 8 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old man arrested two days ago for theft is found unresponsive in his jail cell. Police rush him to the casualty, where he is declared dead on arrival. His family arrives and alleges that the police beat him to death. The jail superintendent says he 'complained of chest pain and collapsed.' The duty doctor must now navigate a medicolegal situation vastly more complex than a standard road accident death: a death in state custody, allegations of institutional violence, a grieving and suspicious family, and the spectre of a human rights investigation. What protocols apply? Who conducts the autopsy? Where does the report go? And what special precautions ensure that neither evidence is missed nor the physician becomes complicit in a cover-up?
WHY THIS MATTERS
Special-situation autopsies — custodial deaths, anaesthetic deaths, negligence deaths — are encountered with significant frequency in Indian medical practice. India's National Human Rights Commission (NHRC) has issued specific guidelines precisely because these cases were routinely mishandled, leading to impunity for perpetrators of custodial violence. As a future clinician, you may be involved either as the forensic examiner or as a medical team member whose conduct is scrutinised. Understanding the enhanced protocols, the team-based approach, and the statutory framework is essential for both justice and your own professional protection.
RECALL
Revisit from earlier modules: (1) CRPC Section 176 — when is a magistrate inquest mandatory rather than a police inquest? (specifically: custodial deaths and deaths of married women within seven years of marriage); (2) the standard viscera preservation schedule — these apply to special autopsies too, but with additional specimens; (3) the distinction between cause and manner of death — in special-situation deaths, manner (homicide vs natural vs accidental) is frequently contested; (4) IPC Section 304A — negligence causing death (rash or negligent act not amounting to culpable homicide).
Medicolegal Scenario: Death in a Special Situation
Three categories of death share the common feature that the circumstances of death inherently raise questions about institutional or professional accountability, and that a routine medico-legal autopsy, even properly conducted, may be insufficient to address those questions without enhanced protocols.
Custodial deaths (FM2.20) include deaths occurring in police lock-ups, jails, remand homes, government psychiatric institutions, or any place where the state has assumed custody of a person. The 'special' element is that the state, which has a constitutional and statutory duty of care towards those in its custody, is simultaneously the primary suspect in cases of unnatural custodial death. This creates an inherent conflict of interest that the NHRC guidelines were specifically designed to address.
Anaesthetic and operative deaths (FM2.24) are deaths occurring during or immediately following surgical procedures, whether under general, regional, or local anaesthesia, or due to recognised or disputed complications of the procedure. The special element is that pharmacological agents, technical errors, equipment failure, and pre-existing disease all operate simultaneously, making causal attribution technically complex and medicolegally contested.
Negligence deaths (FM2.26 in part) are deaths attributed to acts or omissions — rash or negligent acts not amounting to intentional homicide — by healthcare providers, institutions, or other persons with a duty of care. These invoke IPC Section 304A (causing death by negligence) and may involve civil claims under consumer protection law. The forensic physician in these cases is typically asked not just 'what caused death?' but 'was the standard of care met?' — a question requiring both clinical and medicolegal expertise.
The unifying theme is that evidence integrity and institutional independence are paramount. In all three categories, the forensic physician must be visibly free of institutional pressure, the examination must be unusually thorough, and the report must meet a higher evidentiary standard because it will face intense adversarial scrutiny.
Scientific and Pathological Basis of Special-Situation Deaths
Understanding the pathological spectrum expected in each special-situation category helps the forensic physician formulate the examination to detect (or exclude) the relevant findings. Missing a relevant finding in these high-stakes cases has direct consequences for justice outcomes.
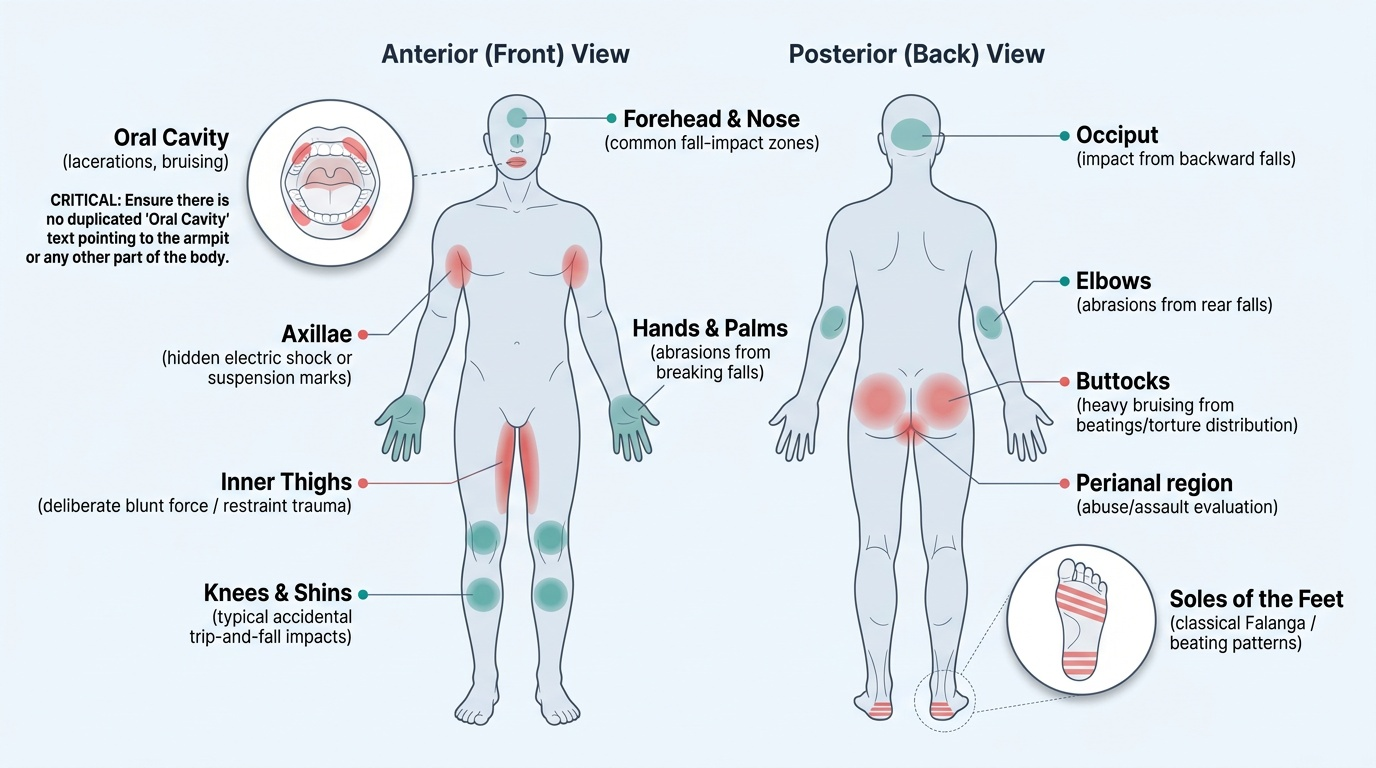
In custodial deaths, the pathological spectrum includes: (a) blunt force injuries — contusions, lacerations, fractures from beatings; these may be located on non-clothing-covered areas (head, face) or deliberately in areas usually hidden (soles of feet — falanga, axillae, buttocks — the notorious 'torture distribution'); (b) positional asphyxia from forced restraint (prone restrained position → mechanical asphyxia); (c) ligature/manual strangulation disguised as suicide by hanging; (d) neglect-related deaths — untreated medical conditions, dehydration, diabetic ketoacidosis, withdrawal states (alcohol, opioids); (e) sudden cardiac death precipitated by fear, assault, or severe pain (stress cardiomyopathy).
The forensic physician must examine the entire body surface, including areas not normally inspected in standard autopsies — the soles of the feet, the inner aspects of the thighs, the perianal region, the oral cavity — because deliberate torture tends to target areas where bruising is less visible.
Provided image
In anaesthetic deaths, the relevant pathological findings include: (a) evidence of hypoxia — cyanosis, petechial haemorrhages on conjunctivae and epicardium, cerebral oedema; (b) anaphylactic changes — mucosal oedema, angioedema, bronchospasm (inspect bronchi); (c) pulmonary embolism or fat embolism; (d) malignant hyperthermia — massive rhabdomyolysis (myoglobinuria, swollen pale muscles); (e) accidental overdose findings — cardiac arrhythmia patterns, drug-specific organ changes; (f) equipment-related findings — aspiration, failed airway management signs.
In negligence deaths, the forensic physician must document both what is present (the pathological changes) and what was absent or delayed (e.g. evidence that a treatable condition was not treated — an appendix perforated beyond the point where surgical management should have been available). This 'negative finding' documentation requires a detailed clinical opinion from a specialist in the relevant field, emphasising the team-based approach mandated by FM2.26.
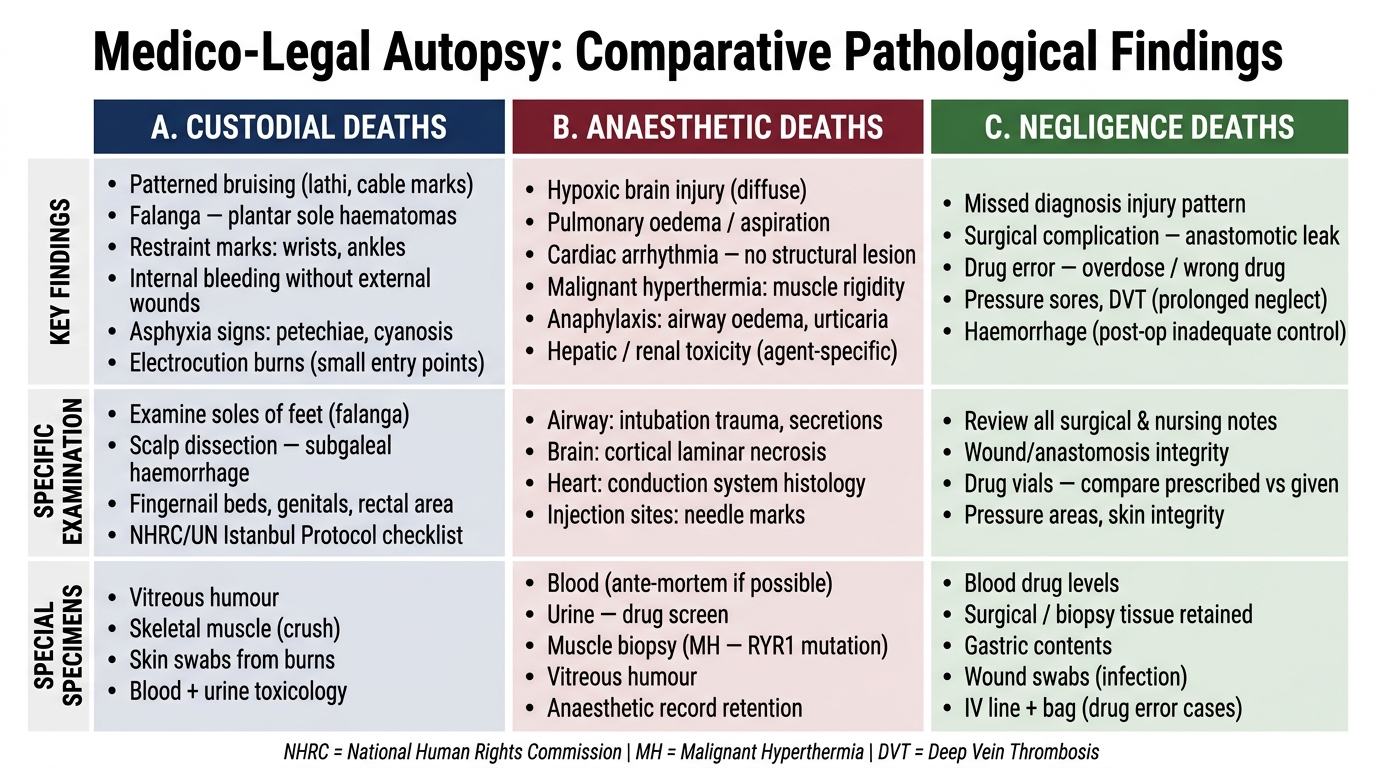
Comparative Pathological Findings: Custodial vs Anaesthetic vs Negligence Deaths
SELF-CHECK
In a suspected custodial torture death, the forensic physician should specifically examine the soles of the feet because:
A. Foot injuries are the most common pattern in all forms of homicide
B. Falanga (beating of the soles) leaves injuries in an area less visible to casual inspection, deliberately used by torturers to avoid detection
C. Petechial haemorrhages of the soles are pathognomonic of asphyxia
D. The soles are required to be examined by CRPC Section 176
Reveal Answer
Answer: B. Falanga (beating of the soles) leaves injuries in an area less visible to casual inspection, deliberately used by torturers to avoid detection
Falanga is a form of torture involving systematic beating of the soles of the feet. It is specifically targeted because the resultant bruising is hidden by footwear and normal gait, making it less likely to be noticed or reported. Forensic examination of the soles is not mandated by CRPC Section 176 per se, but is required by the comprehensive examination standard and specifically highlighted in NHRC and human rights PM guidelines for custodial deaths.
Protocol for Autopsies in Custodial Deaths: NHRC Guidelines
The National Human Rights Commission (NHRC) of India has issued two relevant sets of guidelines that the forensic physician must know distinctly. The first is the general framework for investigating human rights violations, which sets principles of independent investigation, documentation, and reporting. The second — and more operationally specific — is the NHRC Guidelines for Investigation of Deaths in Custody (1997), which mandates a specific procedure for all custodial deaths, whether in police lock-ups or jails.
The key elements of the NHRC custodial death protocol are:
1. Mandatory magistrate inquest (CRPC Section 176): a police inquest alone (Section 174) is insufficient for custodial deaths. The magistrate must conduct an independent inquiry. The PM report goes to the magistrate directly, NOT through the police — this prevents interference by investigating officers who may have a conflict of interest.
2. Video-recording of the autopsy: the NHRC guidelines strongly recommend that the post-mortem examination of all custodial deaths be video-recorded in its entirety. This creates an independent evidentiary record that cannot be altered after the fact and allows subsequent review if findings are disputed.
3. Team-based examination (FM2.26): the autopsy should be performed by a minimum of two doctors — ideally a forensic medicine specialist and a histopathologist — with consultation from other specialists as required (e.g. a neurologist for head injuries, a cardiologist for cardiac findings). This prevents single-physician accountability and ensures specialist expertise for complex findings.
4. Special specimen collection: in addition to standard viscera, the protocol requires: (a) collection of blood for alcohol, drugs, and toxins; (b) collection of urine for drug screen; (c) swabs from injuries for microbiological analysis; (d) histology of all organs (including skin at injury sites) to assess the age of injuries and identify pathological changes; (e) photography of all injuries with a scale ruler.
5. Documentation of the entire body surface: a body chart must be completed, mapping every external finding including colour, size, and precise anatomical location of each bruise, wound, or mark. The distribution of injuries must be assessed for consistency with the alleged history (e.g. 'slipped and fell' vs multiple injuries in different locations at different ages).
6. NHRC notification: state authorities are required to notify the NHRC of all custodial deaths within 24 hours. The PM report is eventually submitted to the NHRC as part of the inquiry file.
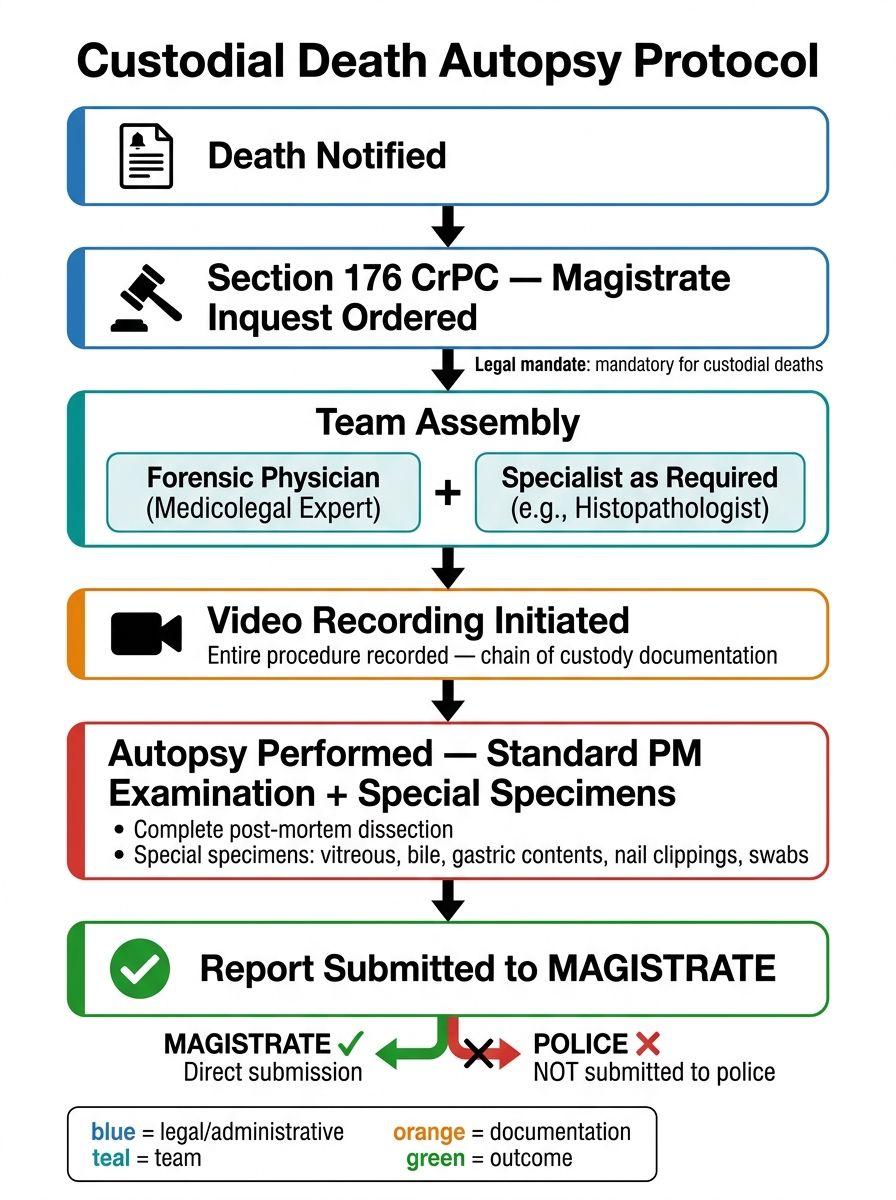
Custodial Death Autopsy Protocol — Section 176 CrPC Flowchart