Page 1 of 6
FM9.1 | Child Abuse & Battered Baby Syndrome — SDL Guide
Learning Objectives
- Define child abuse and enumerate its major types with forensic significance
- Describe the classic triad of Battered Baby Syndrome (Caffey's syndrome) and its pathological basis
- Recognise the clinical features that distinguish non-accidental from accidental injury
- Apply POCSO Act 2012 and JJ Act 2015 mandatory reporting obligations in practice
- Document child abuse injuries accurately for medicolegal purposes
INSTRUCTIONS
Child abuse is one of the most consequential forensic diagnoses a clinician can make — getting it right protects a vulnerable child; getting it wrong can destroy a family or allow abuse to continue. This module equips you with the pattern-recognition skills, pathological understanding, and legal obligations needed to identify and respond to suspected child abuse with both clinical precision and professional responsibility.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old infant is brought to the emergency department by her parents, who report she 'rolled off the bed' that morning. On examination you find her unresponsive, with bilateral retinal haemorrhages on fundoscopy, a tense anterior fontanelle, and fresh bruising over both ears and the nape of the neck. The chest X-ray shows healing posterior rib fractures at different stages. The history is inconsistent with the injuries before you. What is the forensic significance of this constellation, and what are your legal obligations?
WHY THIS MATTERS
Child abuse is a global public-health and medicolegal emergency. In India, the Protection of Children from Sexual Offences Act 2012 (POCSO) and the Juvenile Justice (Care and Protection of Children) Act 2015 (JJ Act) create explicit mandatory reporting obligations for healthcare professionals. A doctor who fails to report suspected child abuse violates Section 19 of POCSO and can face criminal liability. Beyond the law, the forensic physician is uniquely positioned to recognise injury patterns that caregivers may deliberately conceal, to document findings that withstand legal scrutiny, and to trigger the protective mechanisms that keep children safe. Understanding Battered Baby Syndrome — the archetypal presentation — is therefore not merely academic: it is a professional imperative.
RECALL
Before proceeding, recall the following from your earlier studies:
- Wound classification: abrasion (epidermis only, no tissue gap), contusion (blunt force, intact skin, haemorrhage in tissue), laceration (blunt force, irregular torn edges, tissue bridges), incised wound (sharp edge, clean margins) — these distinctions matter when documenting child abuse injuries.
- Subdural haematoma: a collection of blood between the dura mater and the arachnoid mater, classically caused by tearing of bridging veins; in adults it is usually associated with significant trauma, but in infants the larger subarachnoid space and less-myelinated brain make even rotational acceleration-deceleration forces sufficient.
- Epiphyseal anatomy: metaphyses of long bones in infants are zones of rapid osteogenesis and are mechanically the weakest part of the growing bone — making them specifically vulnerable to traction-shear injuries.
Medicolegal Scenario: The Battered Child
The medicolegal concept of the battered child syndrome — later called Battered Baby Syndrome — was first systematically described by paediatrician John Caffey in 1946 and formalised by Kempe et al. in their landmark 1962 paper in JAMA. The syndrome is now also called Caffey's syndrome or non-accidental injury (NAI). Its forensic significance lies not in any single dramatic finding but in the constellation of injuries in a child whose given history cannot explain the observed trauma.
The central forensic challenge in child abuse is that abusers routinely fabricate innocent explanations — 'the baby fell off the bed,' 'the sibling was playing too rough,' 'I don't know how it happened.' A doctor trained in forensic medicine must be able to apply a systematic framework: does the injury pattern fit the stated mechanism? Is the developmental stage of the child consistent with the alleged activity? Are there injuries at different stages of healing, suggesting repeated episodes? Is the delay in seeking care suspicious?
The medicolegal scenario almost always begins with an inconsistent history. Classic indicators of suspicion include:
- An infant younger than 6 months presenting with fractures (infants this age cannot yet walk or climb)
- Multiple fractures in different bones at different stages of healing
- Intracranial injury in the absence of a high-velocity accident
- Retinal haemorrhages in a child without a documented road-traffic accident
- Patterned bruises (belt buckle, cord, cigarette burns) inconsistent with play injuries
- Perineal or genital injuries in a pre-ambulatory child
- Unexplained delay between injury and presentation
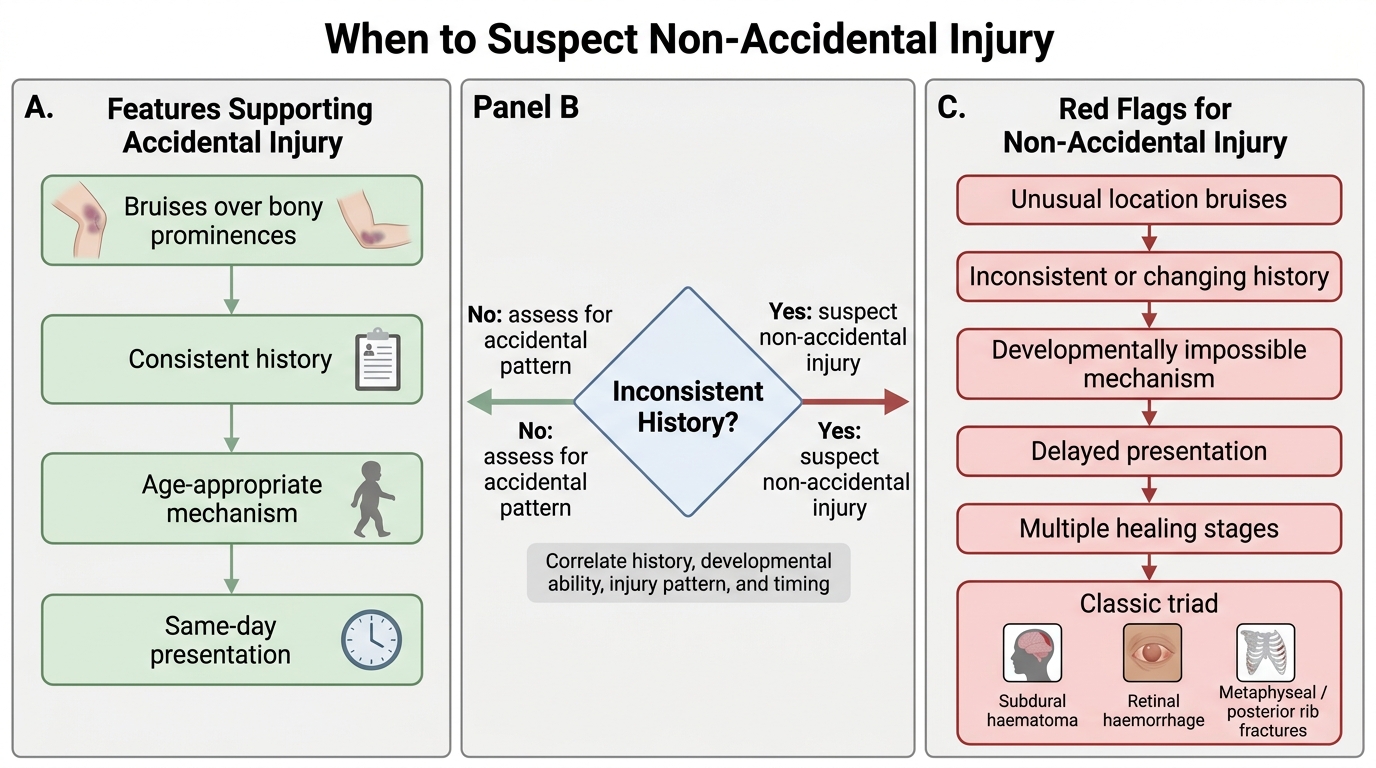
When to Suspect Non-Accidental Injury
Pathological Basis: How Child Abuse Injures
Understanding the pathological mechanisms behind the characteristic injury patterns of Battered Baby Syndrome is essential for convincing medicolegal testimony. The three components of the classic triad — (1) subdural haematoma, (2) retinal haemorrhage, and (3) metaphyseal and/or posterior rib fractures — arise from distinct but related biomechanical forces, and their co-occurrence is highly specific for non-accidental injury.
Subdural haematoma in infants results from acceleration-deceleration forces that tear the bridging veins traversing the subdural space. In the infant brain, the subarachnoid space is proportionally larger, and the bridging veins are under greater tension. Violent shaking — the mechanism in Shaken Baby Syndrome — generates rotational accelerations 5–10 times greater than those sustained in typical household falls. The result is tearing of multiple bridging veins, bilateral subdural haematomas, and diffuse axonal injury. CT imaging shows hyperdense collections over both cerebral convexities, often with evidence of prior small haematomas (mixed-density collections indicating repeated injury).
Retinal haemorrhages in the shaken baby are bilateral, extend to the periphery of the retina, and frequently involve multiple layers (preretinal, intraretinal, subretinal). This pattern is virtually pathognomonic of severe rotational acceleration-deceleration injury. Unilateral or small flame haemorrhages occur in other conditions (birth trauma, severe anaemia, coagulopathy, meningitis), but the bilateral, peripheral, multi-layered pattern in the context of the clinical presentation points unmistakably to violent shaking.
Metaphyseal and posterior rib fractures have distinct mechanical origins. Metaphyseal corner fractures (also called 'bucket handle' fractures or classical metaphyseal lesions) result from traction and torsion applied to an infant's limbs during shaking or forceful grabbing — the cartilaginous metaphysis shears at the zone of provisional calcification. These fractures are highly specific for child abuse because the same mechanism does not occur in everyday falls. Posterior rib fractures result from squeezing — the infant's thorax is gripped and compressed, levering the ribs over the transverse processes. Both fracture types are essentially never caused by cardiopulmonary resuscitation.
Additional injury patterns associated with physical child abuse include:
- Patterned bruises: imprints of objects used (belt buckles, cords, hands, bite marks) — photographed and documented with a scale ruler
- Bruises in unusual locations: ears, neck, buttocks, lower abdomen — accidental bruises overwhelmingly occur over bony prominences (forehead, shins, elbows) in ambulatory children
- Burns: cigarette burns (circular, punched-out), contact burns (recognisable object shapes), scalding (immersion burns with sharp tide marks — 'glove and stocking' distribution)
- Abdominal trauma: duodenal haematoma, liver or spleen laceration — the second leading cause of death in physical abuse after head injury
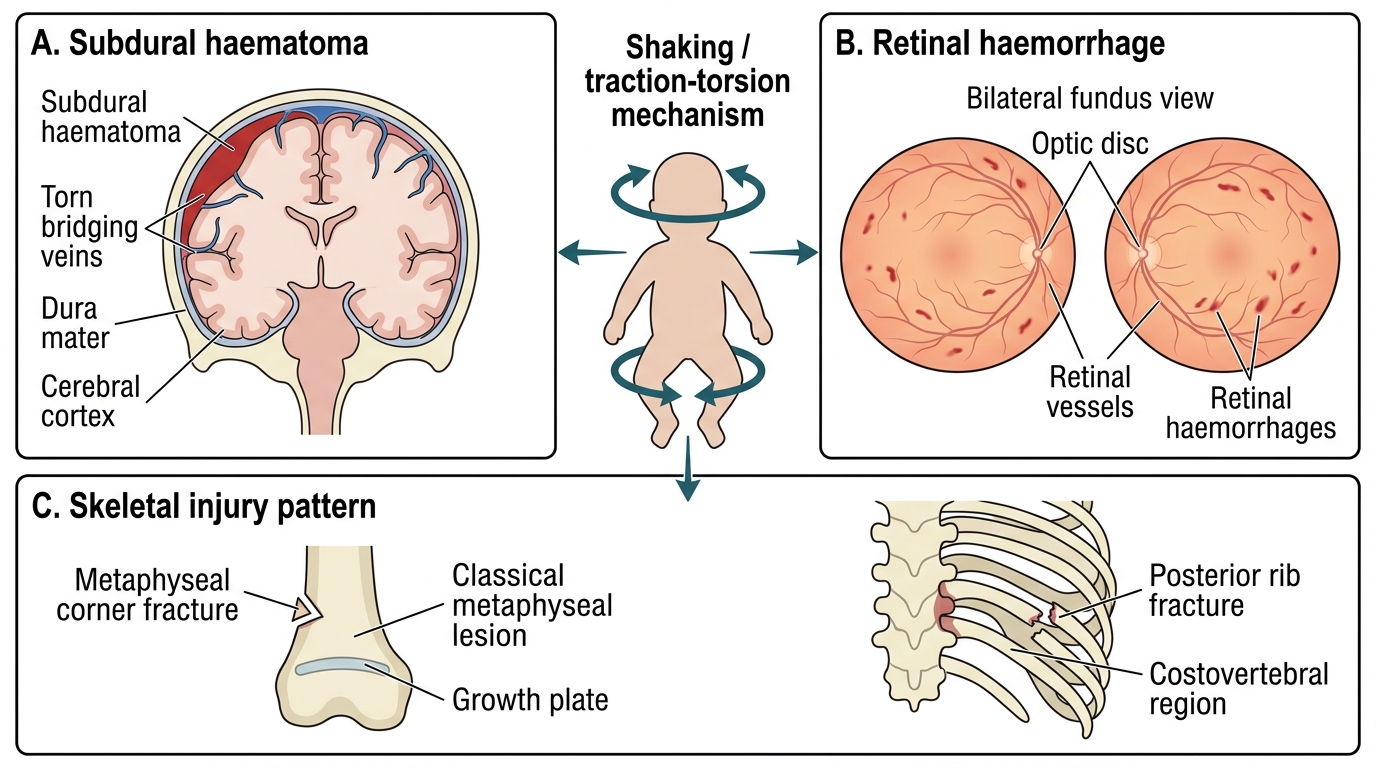
Classic Battered Baby Syndrome Triad
SELF-CHECK
Which of the following fracture patterns is MOST specific for non-accidental injury in an infant?
A. Linear parietal skull fracture
B. Metaphyseal corner (classical metaphyseal lesion) fracture
C. Mid-shaft femur fracture in a 3-year-old
D. Greenstick fracture of the radius
Reveal Answer
Answer: B. Metaphyseal corner (classical metaphyseal lesion) fracture
Metaphyseal corner fractures (classical metaphyseal lesions) are highly specific for non-accidental injury because they result from traction and torsion forces applied during shaking or forceful grabbing — a mechanism that does not occur in everyday accidental falls. Linear parietal skull fractures can occur from simple falls; mid-shaft femur fractures in ambulatory children can be accidental; greenstick fractures are common in accidental forearm injuries.
Clinical Examination and Pattern Recognition
The forensic physician's role in a suspected child abuse case begins with a thorough, systematic, and carefully documented clinical examination. The examination must be approached with two simultaneous goals: providing medical care for the injured child and generating medicolegal evidence that will withstand judicial scrutiny. Failure to document adequately at the time of examination cannot be remedied later.
History-taking is the first critical step. The history should be taken from all caregivers separately (inconsistencies between separate accounts are significant), noting the exact words used (quotation marks in the record). Key elements:
- The mechanism and circumstances of injury, in the caregiver's own words
- The timing and sequence of events — any delay between injury and seeking care
- Developmental assessment: could a child of this age and developmental stage have caused this injury accidentally?
- Previous medical history, prior fractures, prior hospital attendances
- Family composition and dynamics
Physical examination must be head-to-toe, with every finding recorded using precise anatomical terms, measurements, and a body diagram. Key elements:
- Bruises: location (anatomical region), size, shape, colour, patterning; age estimation from colour (fresh = red/blue, 24–72 h = blue/purple, 4–7 days = green/yellow, >7 days = yellow/brown — but note overlapping ranges make exact dating unreliable; multiple bruises at different colour stages suggest repeated injury)
- Burns: type, location, margins (sharp margins = forced immersion; splash/pour patterns suggest accidental)
- Fundoscopy: mandatory in every suspected case — bilateral retinal haemorrhages as described above
- Skeletal survey: full skeletal X-ray series (skull, thorax, long bones, pelvis, hands, feet) — the radiological standard of care in suspected physical abuse; isotope bone scan is a complementary investigation
Distinguishing accidental from non-accidental injury requires a structured comparison:
| Feature | Accidental | Non-accidental (suspicious) |
|---|---|---|
| History | Consistent with injury | Inconsistent or changing |
| Developmental stage | Injury possible for age | Impossible for stated age |
| Injury locations | Bony prominences (forehead, shins) | Ears, neck, buttocks, trunk, genitalia |
| Fracture type | Simple, single | Metaphyseal, posterior rib, multiple stages |
| Delay in presentation | Immediate or same-day | Hours to days |
| Previous attendances | Rare | Multiple, different facilities |
Dating injuries has limits: bruise colour dating has wide confidence intervals; fracture callus formation provides a better estimate (periosteal reaction appears at 7–10 days; definite callus at 14–21 days). Radiological staging of healing fractures is therefore an important evidence base in recurring abuse.
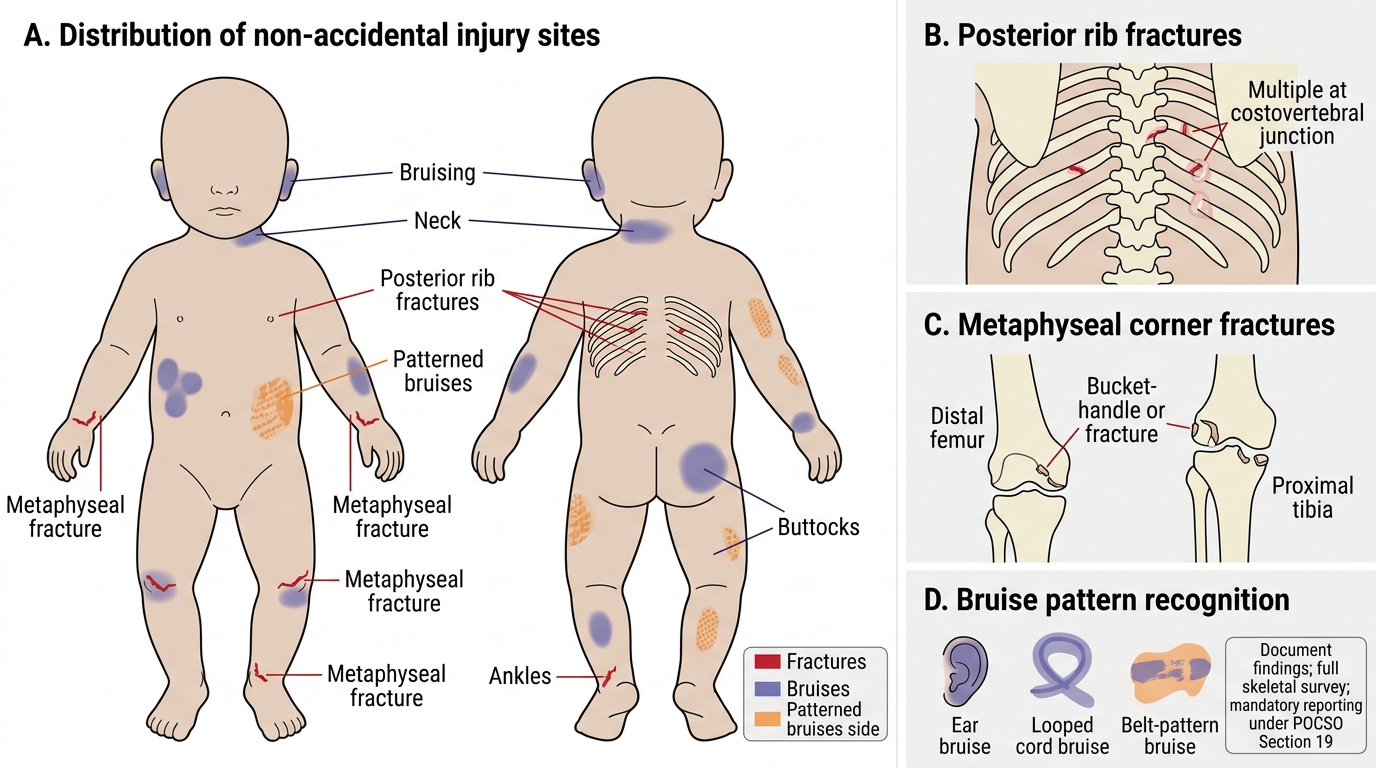
Non-Accidental Injury Sites in an Infant
SELF-CHECK
A 14-month-old child is brought in with bilateral retinal haemorrhages, subdural haematoma on CT, and posterior rib fractures at multiple healing stages. The caregiver states 'he fell out of the cot.' What is the MOST appropriate next step from a medicolegal standpoint?
A. Accept the history and treat the injuries medically
B. Request a full skeletal survey and document all findings for reporting under POCSO
C. Wait for parent consent before performing further investigations
D. Report only if there is a confession of abuse
Reveal Answer
Answer: B. Request a full skeletal survey and document all findings for reporting under POCSO
The constellation of bilateral retinal haemorrhages, subdural haematoma, and posterior rib fractures at multiple healing stages constitutes the classic Battered Baby Syndrome triad — highly specific for non-accidental injury. The clinician must (a) complete a full skeletal survey as standard care, (b) document all findings meticulously, and (c) report under Section 19 of POCSO Act 2012 — mandatory reporting does not require parental consent or a confession. A cot fall cannot explain this pattern.
Medicolegal Framework: Reporting, Legislation & Inference
India has two primary legislative instruments that govern the forensic physician's obligations in child abuse cases. Both impose mandatory duties, and understanding their scope is essential for competent practice.
POCSO Act 2012 (Protection of Children from Sexual Offences Act) primarily governs sexual offences against children but contains reporting provisions applicable to all suspected child abuse when the victim is under 18 years of age. The age threshold of <18 years is absolute — there are no exceptions for consent or marriage. Key provisions:
- Section 19 — Mandatory Reporting: Every person (including a doctor) who has reasonable grounds to believe that a sexual or other offence under POCSO has been committed MUST report to the Special Juvenile Police Unit (SJPU) or local police. Failure to report is a criminal offence under Section 21, punishable with imprisonment up to 6 months and/or fine.
- Aggravated penetrative sexual assault (Sec 5–6) includes offences committed by persons in a position of trust (teachers, doctors, family members).
- Non-contact offences (voyeurism, exhibitionism, online abuse) are explicitly included.
Juvenile Justice (Care and Protection of Children) Act 2015 (JJ Act) provides the broader child protection framework, including the concept of 'children in need of care and protection' (CNCP). Key obligations include:
- Section 34 — Reporting: Every person who becomes aware of a child in need of care and protection must report to the Child Welfare Committee (CWC) or the police.
- Child Protection Officer (CPO): designated in every district to coordinate response to child abuse reports.
- The JJ Act works in tandem with POCSO — a report can trigger both CWC intervention (child protection) and criminal investigation (police/SJPU).
IPC provisions relevant to child abuse:
- IPC 323: voluntarily causing hurt (non-grievous)
- IPC 325: voluntarily causing grievous hurt (long-bone fractures qualify as 'fracture' under Section 320 definition)
- IPC 304: culpable homicide not amounting to murder (if the child dies)
- IPC 302: murder (if intent to kill is established)
Preparing the medicolegal report in a child abuse case must include:
- Identity and demographics of the child
- Date, time, and place of examination
- Informant details (who gave the history, their relationship to the child)
- Summary of history with exact quotations from caregivers
- General physical examination findings
- All injuries with precise description, body diagram annotation
- Fundoscopic findings
- Radiological and laboratory findings (with dates)
- Opinion section: forensic assessment of whether the injuries are consistent with the stated history; whether the pattern raises suspicion of non-accidental injury; differential diagnoses considered and excluded
- Mandatory report filed under (Section 19 POCSO / Section 34 JJ Act) — reference number and authority notified
Differential diagnoses that must be formally excluded before concluding non-accidental injury:
- Osteogenesis imperfecta (OI): brittle bone disease — family history, blue sclerae, dentinogenesis imperfecta, hearing loss; bone densitometry and collagen mutation testing
- Bleeding disorders: haemophilia, von Willebrand disease, ITP — bruising without external force; coagulation screen and platelet count
- Metabolic bone disease: rickets (Vitamin D deficiency) — fractures with low bone density; X-ray shows metaphyseal cupping/fraying
- Leukaemia: periosteal reaction + bruising mimicking abuse; blood film and bone marrow
- Mongolian spots: blue-grey birthmarks over sacrum/buttocks, common in Indian children — must not be recorded as bruises
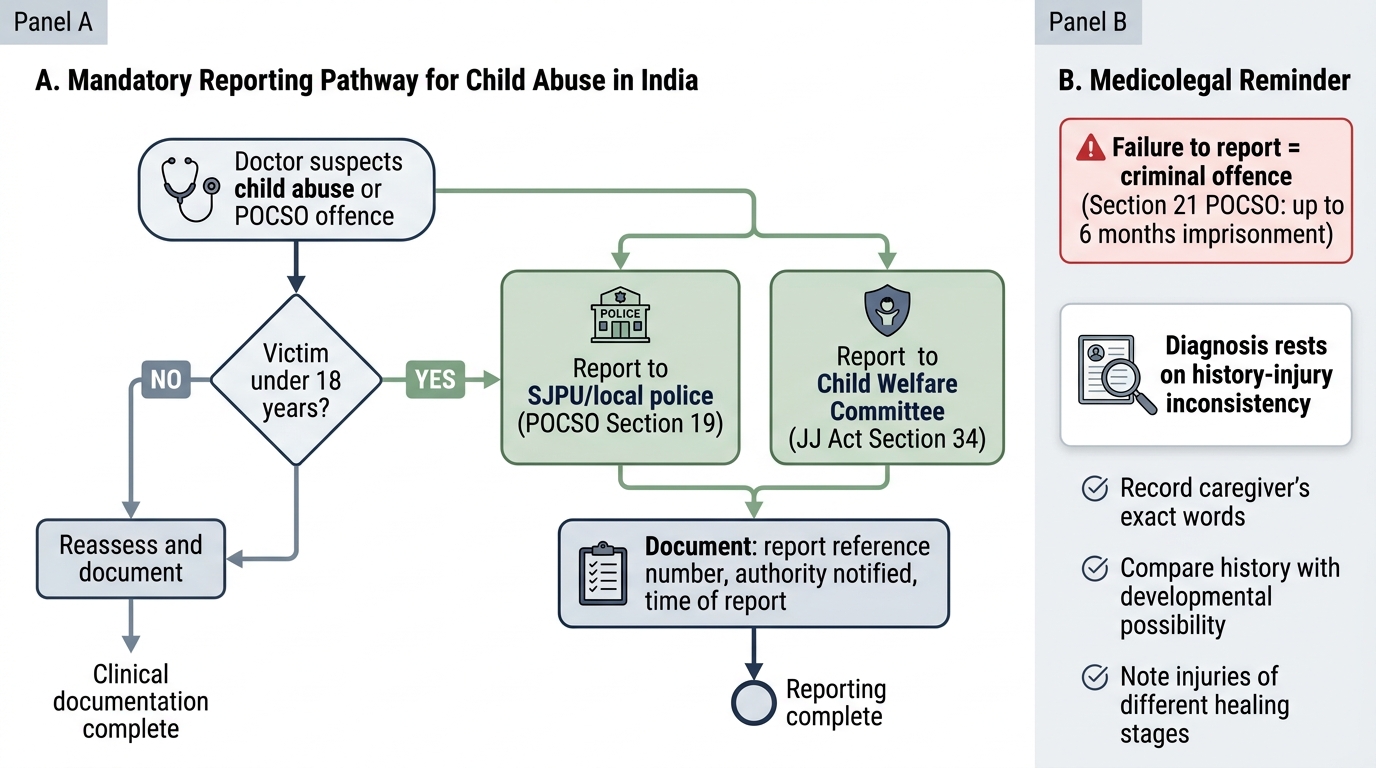
Mandatory Reporting Pathway for Child Abuse in India
CLINICAL PEARL
The forensic pathologist's dictum: 'The diagnosis of child abuse is made by the history, not the injury.' Any single injury in isolation can usually be explained away. It is the inconsistency between the stated history and the physical findings — the developmental impossibility, the multiplicity of healing stages, the anatomically atypical distribution — that establishes the medicolegal case. Document the exact words of the caregiver; they often provide the most powerful evidence of inconsistency when placed alongside the objective clinical findings.
SELF-CHECK
Under POCSO Act 2012, what is the age threshold below which a child is protected, and what is the consequence for a doctor who fails to report a suspected offence?
A. Under 16 years; no criminal consequence for doctors
B. Under 18 years; criminal liability including imprisonment up to 6 months under Section 21
C. Under 14 years; suspension of medical licence
D. Under 18 years; civil liability only
Reveal Answer
Answer: B. Under 18 years; criminal liability including imprisonment up to 6 months under Section 21
POCSO Act 2012 applies to all children below 18 years of age — no exceptions. Section 19 imposes mandatory reporting on every person including doctors. Section 21 makes failure to report a criminal offence punishable with imprisonment up to 6 months and/or fine. The law creates no exemption based on professional discretion.
KEY TAKEAWAYS
Child Abuse & Battered Baby Syndrome — Key Points:
- Battered Baby Syndrome (Caffey's syndrome): non-accidental injury characterised by the classic triad of (1) subdural haematoma, (2) retinal haemorrhage (bilateral, peripheral, multi-layered), and (3) metaphyseal corner fractures and/or posterior rib fractures — all three components are diagnostically important.
- Mechanism: violent shaking (Shaken Baby Syndrome) generates rotational acceleration-deceleration forces 5–10× greater than accidental falls, tearing bridging veins (subdural haematoma) and causing simultaneous retinal and skeletal injuries.
- Clinical recognition: inconsistent history is the cornerstone; injuries in unusual anatomical locations, multiple fractures at different healing stages, and the triad above are the key red flags.
- Mandatory reporting — POCSO Act 2012: every person including doctors must report under Section 19 to SJPU/police; failure is a criminal offence (Section 21 — up to 6 months imprisonment); age threshold is <18 years, absolutely.
- JJ Act 2015: parallel obligation to report to Child Welfare Committee; Child Protection Officer coordinates response.
- Documentation: full skeletal survey, fundoscopy, precise wound description with body diagram, caregiver's exact words — all must be recorded contemporaneously.
- Differential diagnoses to formally exclude: osteogenesis imperfecta, bleeding disorders, rickets, leukaemia, Mongolian spots.
REFLECT
Consider this scenario: You examine a 2-year-old brought in with a spiral femur fracture. The father says 'he tripped and fell.' Your clinical assessment raises concern for non-accidental injury, but the family are distressed and the child appears well-nourished and cared-for. Reflect on the tension between your clinical suspicion, your legal obligations under POCSO and the JJ Act, your duty of confidentiality to the family, and your primary responsibility to the child. What would you do, and how would you communicate your concerns to the family while fulfilling your mandatory reporting obligations?