Page 7 of 14
FM2.1-2,FM14.5 | Cause-of-Death Certification: MCCD & ICD-11 — SDL Guide (Part 2)
Completing the MCCD: Worked Examples and Common Errors
The best way to learn MCCD completion is through worked examples that reflect real clinical situations. Three scenarios are presented below with step-by-step reasoning.
Worked Example 1: Lung cancer with pneumonia
Clinical story: A 62-year-old smoker, known case of right lower lobe squamous cell carcinoma of the lung, developed aspiration pneumonia 3 weeks before death. He deteriorated and died from hypoxic respiratory failure.
MCCD completion:
- Part I Ia: Hypoxic respiratory failure
- Part I Ib: Aspiration pneumonia
- Part I Ic: Squamous cell carcinoma of the right lower lobe, lung
- Part II: (blank in this case — no independent contributing conditions)
ICD-11 code for underlying cause (Ic): Search 'squamous cell carcinoma lung' → appropriate code under Chapter 2 (Neoplasms)
Worked Example 2: Diabetic with coronary artery disease
Clinical story: A 70-year-old man with type 2 diabetes and hypertension for 15 years had a massive anterior myocardial infarction and died 12 hours after onset of chest pain.
MCCD completion:
- Part I Ia: Acute anterior ST-elevation myocardial infarction
- Part I Ib: (blank — the underlying disease directly caused the MI)
- Part I Ic: Atherosclerotic coronary artery disease
- Part II: Type 2 diabetes mellitus; Hypertension
ICD-11 code for underlying cause (Ic): BA80.0 (atherosclerotic coronary artery disease)
Note: Diabetes and hypertension are risk factors — they go in Part II, not Ic, because they are contributing conditions, not the direct underlying disease.
Worked Example 3: Postoperative death
Clinical story: A 58-year-old woman underwent laparotomy for intestinal obstruction secondary to colorectal carcinoma. She developed post-operative pulmonary embolism on day 5 and died.
MCCD completion:
- Part I Ia: Pulmonary embolism
- Part I Ib: Post-operative venous thromboembolism
- Part I Ic: Colorectal carcinoma (underlying condition that necessitated the surgery)
- Part II: (blank)
Note: This death must be assessed for whether it meets the criteria for a medico-legal case (death within 24h of an operation, or in certain states any peri-operative death). If it does, a forensic autopsy may be required and the MCCD cannot be issued by the operating surgeon without that process.
Top 5 MCCD errors to avoid:
1. Writing 'cardiac arrest' or 'cardiorespiratory arrest' in Ia — non-informative; write the disease
2. Leaving Part I as only one row when a causal chain exists — always trace back to the underlying condition
3. Putting comorbidities (diabetes, hypertension) in Part I Ic when they are contributing, not causally direct
4. Reversing the chain direction (putting the underlying cause in Ia)
5. Issuing the MCCD for a death that should have been referred for forensic autopsy — particularly peri-operative deaths and deaths with uncertain cause
SELF-CHECK
A 45-year-old HIV-positive man died from miliary tuberculosis. He had no other significant comorbidities. Which of the following MCCD Part I completions is MOST correct?
A. Ia: Cardiorespiratory arrest; Ib: HIV/AIDS; Ic: Tuberculosis
B. Ia: Miliary tuberculosis; Ib: blank; Ic: blank — with HIV in Part II
C. Ia: Respiratory failure; Ib: Miliary tuberculosis; Ic: blank — with HIV in Part II
D. Ia: Respiratory failure; Ib: Miliary tuberculosis; Ic: blank — with no Part II
Reveal Answer
Answer: B. Ia: Miliary tuberculosis; Ib: blank; Ic: blank — with HIV in Part II
Miliary tuberculosis is the underlying disease that directly caused death — it should be the sole occupant of Part I if no intermediate steps are documented. HIV is a significant contributing condition (it predisposed to tuberculosis) but was not the direct cause of death; it belongs in Part II. Option A incorrectly uses 'cardiorespiratory arrest' as a cause (non-informative) and reverses the chain. Option C is acceptable only if a specific respiratory complication was the immediate step; however, if the terminal event was directly from miliary TB without a distinct separate complication, a one-row Part I is appropriate. Option D omits the HIV contribution in Part II — which should be documented since it is clinically relevant.
CLINICAL PEARL
'Cardiac arrest' is NOT a cause of death. This is the single most important lesson in death certification. Writing 'cardiac arrest' or 'cardiorespiratory arrest' in Box Ia of the MCCD adds no diagnostic information — every person who dies experiences cardiac arrest as the terminal event. It is the mode (mechanism) of death, not the cause. The WHO ICD-11 mortality coding guidelines explicitly flag this as an error and have rules to recode it. When you see 'cardiac arrest' on an MCCD, the proper response is to ask: caused by WHAT disease? The answer — ischaemic heart disease, hypertensive cardiomyopathy, aortic dissection, drug toxicity — is the meaningful medical information. If you genuinely cannot identify any disease, the appropriate response is not 'cardiac arrest' but to review whether the death needs forensic investigation.
Applied Practice and Medicolegal Boundaries
Knowing how to complete the MCCD correctly is one skill; knowing the boundaries of when you can (and cannot) certify is equally essential. The medical and legal framework for death certification in India identifies specific categories of death that require the medicolegal pathway rather than direct MCCD certification.
Practising MCCD completion in a supervised setting (FM14.5) means that Year-2 students are expected to correctly fill a simulated Form 4A given a clinical scenario, selecting the correct underlying cause and checking the causal chain for consistency. The skill examination will provide a case summary and require you to: (a) identify the cause-of-death chain, (b) complete Parts I and II correctly, (c) identify the ICD-11 underlying cause, and (d) state whether this death can be certified or must be referred for forensic process.
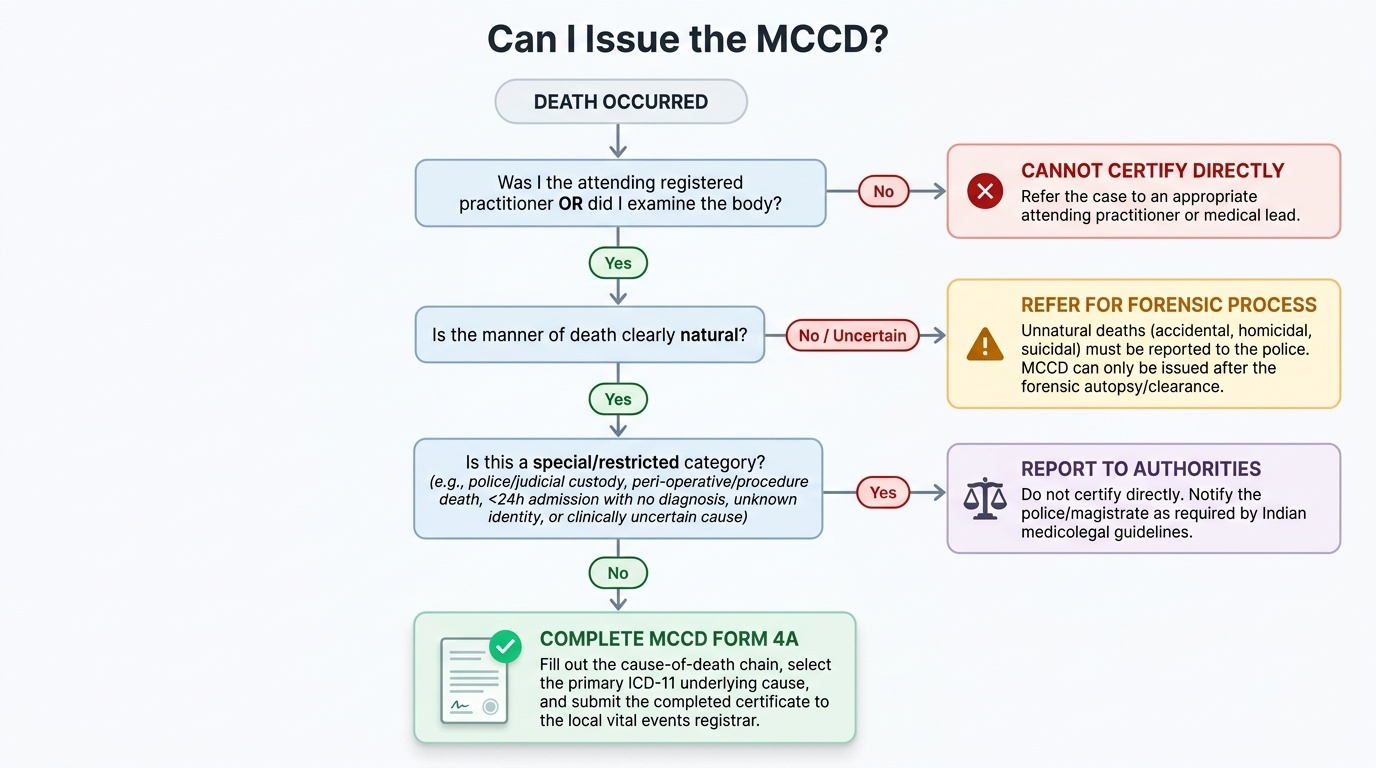
Deaths that CANNOT be certified directly on the MCCD by the treating physician (these require police/magistrate referral and potentially forensic autopsy before any certificate is issued):
- Unnatural deaths: accidental, homicidal, suicidal (manner uncertain or unnatural → forensic autopsy first)
- Deaths in persons admitted for less than 24 hours without an established diagnosis
- Deaths under medical/surgical procedures in circumstances that may involve negligence
- Deaths in police custody, judicial custody, or following police action
- Deaths of unknown identity
- Deaths where the cause is clinically uncertain despite attendance
Amended MCCD: If an error is discovered after the certificate has been issued, the certifying doctor must issue a corrected certificate through the official channel (contact the local vital events registrar); informal amendments to a previously issued certificate are not permissible.
Interaction with forensic autopsy: In cases where a forensic autopsy is performed, the forensic pathologist issues the autopsy report stating the anatomical cause of death. The attending physician (or forensic pathologist, depending on the jurisdiction) then completes the MCCD based on the autopsy findings. The MCCD issued after forensic autopsy must be consistent with the post-mortem report; discrepancies require formal reconciliation.
Provided image
- Doubt about manner → report to police, do not certify directly
- Consumer Protection Act 2019 (NOT 1986): correct year for current jurisdiction
- NMC Act 2020 (NOT IMC Act 1956): correct current regulatory framework for doctor registration
- Any correction to an issued MCCD must go through the official registrar channel