Page 6 of 20
FM6.2,FM14.11 | Firearm & Blast Wound Ballistics — SDL Guide (Part 2)
Blast Injuries: Mechanisms and Classification
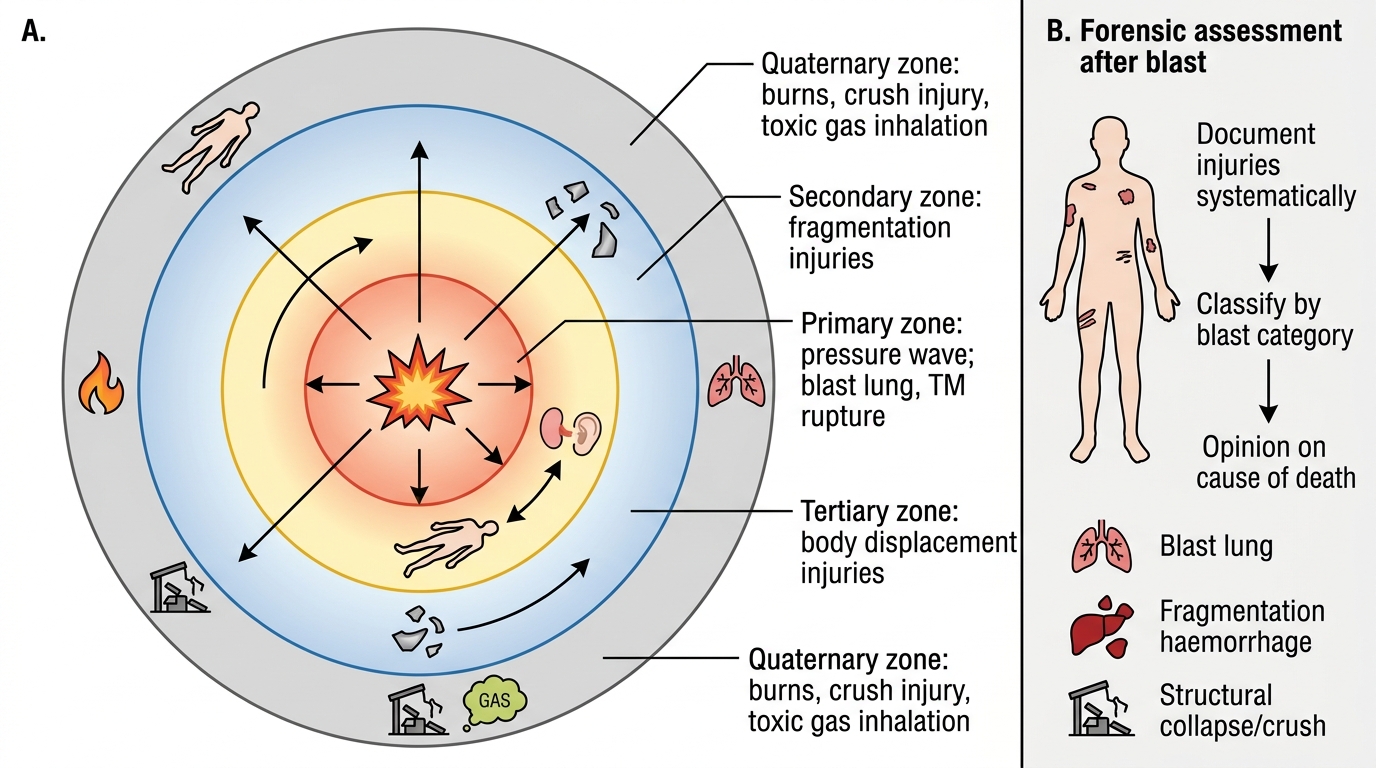
Blast injuries are distinct from gunshot wounds in their mechanism: they result from the detonation of an explosive device, which releases energy as a pressure wave, heat, and fragmentation simultaneously. The classification of blast injuries into four categories is essential both for forensic investigation (determining which injuries were caused by the explosion itself versus secondary collapse or rescue) and for clinical triage at mass casualty incidents. The four categories are mechanistically distinct and must not be conflated.
Primary blast injury results directly from the overpressure wave (blast wave or shock wave) that radiates outward from the explosion at supersonic velocity. This wave is a sudden, brief spike in atmospheric pressure followed by a negative pressure phase. It causes damage at air-tissue interfaces — wherever compressible air-filled spaces exist next to incompressible fluid or solid tissue. Organs particularly vulnerable to primary blast injury include: the lungs (blast lung — alveolar haemorrhage, pneumothorax, air embolism — the most lethal primary injury), the tympanic membranes (rupture, often the earliest and most sensitive indicator of blast exposure), and the bowel (particularly the gas-containing colon and small bowel — perforation, haemorrhage). Primary blast injury produces no external marks — the victim may appear externally uninjured while experiencing life-threatening internal injuries, which is its most dangerous characteristic.
Secondary blast injury results from fragmentation — the fragments of the bomb casing, projectiles packed around the charge, or surrounding structural debris (nails, ball bearings, glass) that are propelled outward by the explosion. Secondary injuries are penetrating wounds, similar in character to gunshot wounds but produced by irregular, often asymmetric fragments at varying velocities. Multiple fragment wounds in a single victim are characteristic. Secondary injuries are often the most common cause of death in explosive attacks.
Tertiary blast injury occurs when the victim's body is thrown by the blast wind (the air current following the pressure wave) against a solid object — a wall, the ground, vehicle interior. The resulting injuries are blunt force injuries: head injuries, fractures, abrasions, and lacerations, similar to those seen in vehicular deceleration. The pattern depends on what the victim struck and with what velocity.
Quaternary blast injury encompasses all other injuries not covered by the first three categories: burns (flash burns from the fireball, flame burns from secondary fires), crush injuries from building collapse, toxic inhalation (carbon monoxide, cyanide from combustion products, chemical agents if a dirty device), and psychological trauma.
Blast Injury Zones and Forensic Assessment
In forensic investigation of a bomb blast, the physician's role includes: documenting all injuries systematically for each body, classifying them by blast category, and providing an opinion on the cause of death (e.g., blast lung vs fragmentation haemorrhage vs structural collapse). This informs both the criminal investigation and the inquest.
CLINICAL PEARL
The absence of blackening or tattooing does NOT rule out close-range firing in every situation. Intermediate surfaces — clothing layers, body armour — absorb blackening and tattooing completely. A bullet fired at close range through thick clothing may produce a 'distant-range-appearing' wound on the underlying skin, even though the weapon was within 15 cm. The forensic physician must always examine the victim's clothing for the residue that is missing from the skin. Similarly, in contact wounds over the skull, the gas may track subdermally rather than blowing back, producing minimal external soiling — the skull itself and the internal wound margins carry the evidence. The experienced physician examines both surfaces of every clothing layer and the wound at multiple planes, never stopping at the superficial skin examination.
Clinical Examination and Wound Documentation
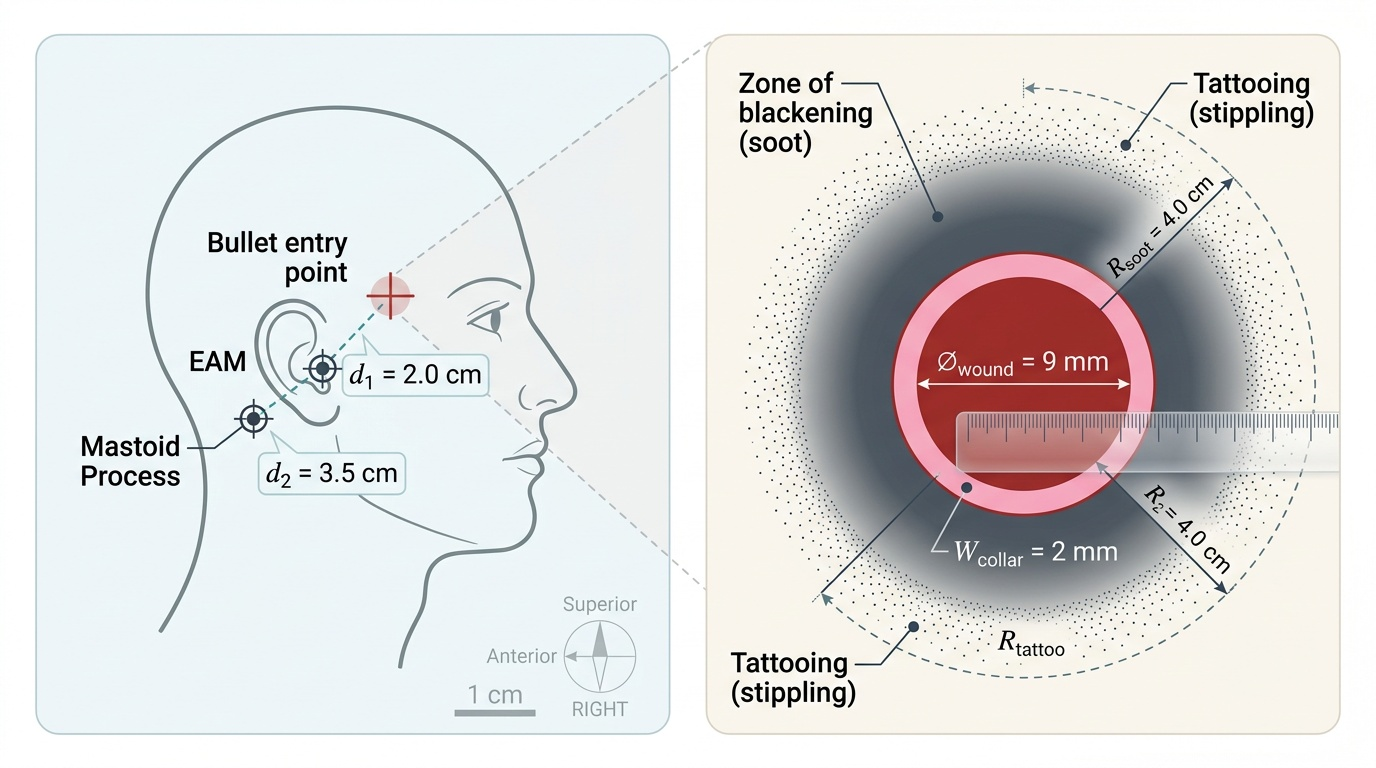
A systematic, reproducible wound examination protocol is the foundation of a court-credible forensic report. The examination findings must be recorded with sufficient precision that any other competent physician could reconstruct the wound from the description alone. Vague descriptions ('circular wound with some blackening') are legally useless; precise measurements, locations, and characterisations ('9 mm circular punched-out wound, 2 cm anterior to the right external auditory meatus, with a 2 mm abrasion collar and 4 cm radius of sooty blackening on the surrounding skin, no tattooing') provide the basis for range and direction opinion.
The head-to-toe systematic examination should document for each wound: anatomical location (region, distance from bony landmarks, laterality), dimensions (length × width for elongated wounds; diameter for circular wounds), shape (circular, oval, irregular, stellate), margins (inverted/everted, clean/ragged, abraded), depth (accessible or penetrating), colour and condition of wound margins, presence of abrasion collar (width and regularity), zone of blackening (radius, distribution, whether on external skin or within wound margins), tattooing (distribution, particle size visible on magnification), singeing of hair (radius), and any foreign material visible in the wound.
The wound track direction is determined at autopsy by probing the wound channel: the track's orientation gives the angle of bullet entry — vertical, angled, or horizontal — which in turn constrains the position of the shooter relative to the victim. A wound entering at the right temple and exiting the left parietal region describes a horizontal track, consistent with a shot fired level with the head. A wound entering the top of the skull and exiting the cervical region describes a downward track — the shooter was above the victim, which is inconsistent with most self-inflicted scenarios.
Examination of clothing is mandatory and should precede examination of the wound surface where possible, because clothing may carry residue that is absent from the skin (absorbed by fabric) and may show the bullet entry point's direction from the fibre displacement around the hole (fibres push inward at entrance, push outward at exit — a subtle but court-admissible finding). All items should be individually packaged and forwarded to the forensic science laboratory.
Provided image
Trace Evidence: Preservation and Dispatch for Forensic Analysis
Trace evidence from firearm scenes and bodies falls into three main categories: gunshot residue (GSR), bullet and cartridge case, and biological material (blood spatter, skin/tissue fragments). Each requires specific collection and preservation protocols to remain admissible and interpretable.
GSR collection must occur before the body is washed, before the scene is disturbed, and before the suspect's hands are allowed contact with any surface. From the deceased: swab the wound margins (anterior and posterior), the hands (dorsal surface, web space between thumb and index finger of both hands — the primary deposition zone for the shooter), and the face. From the suspect: the same hand and face swabs, plus clothing if still wearing the garments present during the shooting. Use pre-moistened cotton swabs in sealed, labelled, sequential containers (separate swab per site). Do not place GSR swabs in plastic bags — moisture accelerates oxidation of lead particles. Paper bags or cardboard tubes are preferred. Deliver promptly; GSR is transferred and degraded with time.
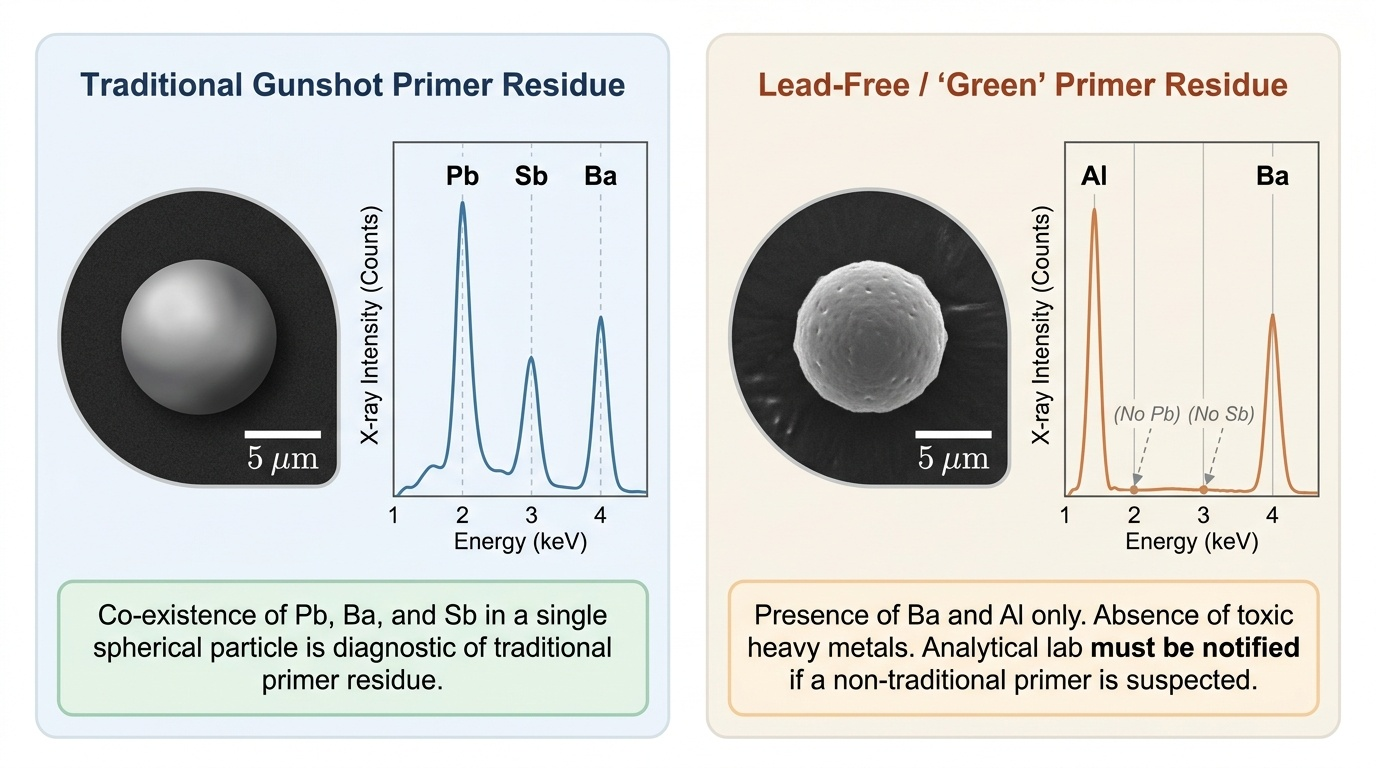
The laboratory test for GSR is scanning electron microscopy with energy-dispersive X-ray spectroscopy (SEM-EDX), which identifies individual particles (spherical morphology from condensed melt droplets) with characteristic elemental composition: traditional primers contain lead (Pb), barium (Ba), and antimony (Sb) in combination — the presence of all three in a single particle is diagnostic of gunshot primer residue. Modern 'green' or lead-free primers have different elemental signatures (Ba+Al, Bi+Sn, etc.) — the laboratory must be informed if a non-traditional primer is suspected. The Dermal Nitrate (paraffin) test is historically described but is no longer accepted as specific for GSR and should not be reported as confirmatory.
Recovered bullets and cartridge cases must be handled with forceps (not fingers — fingerprints on the bullet's surface can obscure rifling marks), wrapped individually in clean paper, placed in rigid containers (not plastic bags that allow movement and mark the bullet surface), and labelled with date, time, location of recovery, and name of the recovering officer. Bullets recovered at autopsy from tissue must have the tissue removed by gentle washing — forceps should grasp the bullet by its base, not its sides, to preserve lateral rifling striations. The recovered bullet, when forwarded to the forensic ballistic laboratory, will be compared with test bullets fired from the suspected weapon.
Chain of custody documentation for all exhibits includes a formal exhibit register: exhibit number, description, collecting officer/physician, date and time, condition at collection, and signature of each person who subsequently handled it. Any gap in the chain is a standard defence challenge.
Provided image
SELF-CHECK
At autopsy, the skin entrance wound shows heavy soot blackening on the deep (internal) surface of the wound margin only, with no external blackening. The wound edges are torn in a stellate pattern. What does this finding indicate?
A. Distant range firing; the bullet yawed before impact, producing the stellate tear
B. Contact wound; all discharge products entered beneath the skin through the bullet track with no external soot deposit, and gas caused the star-shaped skin tear
C. Intermediate range firing; tattooing is present below the visible skin surface
D. Exit wound; internal soiling is characteristic of exit wounds at close range
Reveal Answer
Answer: B. Contact wound; all discharge products entered beneath the skin through the bullet track with no external soot deposit, and gas caused the star-shaped skin tear
Internal (deep-surface) blackening without external sooting, combined with a stellate (star-shaped) skin tear, is the hallmark of a contact wound — particularly a hard contact wound over bone (e.g., skull). The muzzle is pressed against the skin, sealing it; all discharge products enter through the wound track into the subcutaneous tissue or beneath the scalp. The rapid expansion of hot gas under the inelastic skin overlying the rigid skull tears the skin centrifugally, producing the characteristic stellate laceration. This is highly significant: a hard-contact wound to the skull is the classic suicide shot pattern, though it can also occur in homicide (execution-style).