Page 6 of 14
FM1.8-9 | Medico-legal Documentation & Certificates — SDL Guide
Learning Objectives
- Describe the foundational principles of medicolegal documentation, including the legal consequences of inadequate documentation
- Describe the wound certificate, drunkenness certificate, and sickness/fitness certificate — their format, required content, and the applicable legal standards
- Describe the Medical Certificate of Cause of Death (MCCD), distinguishing Form 4 from Form 4A, and explain the correct causal sequence format for death certification
- Describe the age estimation certificate and explain the doctor's obligation to remain current with NMC notifications, state health directives, and BNSS standing orders relevant to medicolegal documentation
INSTRUCTIONS
A doctor's signature on a medicolegal document carries the full weight of professional, civil, and criminal accountability. A wound certificate that inaccurately describes an injury can set a murderer free or convict an innocent person. A death certificate with a poorly stated cause of death corrupts national mortality statistics and may trigger a police investigation for an unnatural death that was in fact natural. This module builds the practical skills of medicolegal documentation — starting from general principles and working through each certificate type in detail.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old construction worker is brought to casualty after an altercation at a worksite. He has three lacerations on his scalp and a fracture of his right radius, confirmed on X-ray. The police requisition asks you to examine and certify injuries. You write in the wound certificate: 'Head injury and fracture.' One week later, the defence lawyer argues in court that 'head injury' is a diagnosis, not a description — and that the certificate does not specify whether the lacerations were blunt or sharp, how deep they were, or whether they were consistent with the weapon the police claim was used. The case stalls. In a separate ward, a 67-year-old woman with a known history of hypertension and ischemic heart disease dies overnight. The duty doctor fills in the death certificate and writes 'cardiac arrest' as the cause of death. Her death is flagged by the registrar as an unnatural death requiring investigation, because 'cardiac arrest' is a mode of dying, not a cause. The family is put through a distressing police inquiry for 10 days before a specialist confirms the correct cause was hypertensive heart disease. Both situations — and the professional, legal, and human consequences they entailed — arose from documentation failures that proper training could have prevented.
WHY THIS MATTERS
Documentation is the interface between clinical medicine and the legal system. Unlike clinical notes, which serve primarily to communicate information within the treating team, medicolegal documents are legal instruments — they have evidentiary weight, they are produced in court proceedings, and they are scrutinised by lawyers and judges who are trained to find ambiguity and exploit it. The quality of India's civil registration and death statistics depends on accurate death certification. The efficacy of the criminal justice system depends on accurate wound documentation. And the doctor's professional standing depends on documentation that is internally consistent, factually defensible, and compliant with current statutory requirements. This module equips you with the specific skills to produce each category of medicolegal document to the required standard.
RECALL
From your previous SDLs, recall that the Bharatiya Sakshya Adhiniyam (BSA) 2023 governs what evidence is admissible in court, and that a document that does not meet its evidentiary standards may be excluded. From your community medicine training, recall the Vital Statistics system — birth and death registration under the Registration of Births and Deaths Act — because the death certificate is the primary data input for that system. From your clinical training, recall how you document injuries in clinical notes — the medicolegal wound certificate requires the same description but with additional specificity and a formal structure that can withstand courtroom scrutiny. And from the previous SDL on court conduct, recall that certifying a false document is perjury under BNS 2023, punishable with imprisonment up to seven years.
Principles of Medico-legal Documentation
All medicolegal documents share a set of foundational principles that determine their legal validity. A document that violates any of these principles — however factually accurate — may be challenged in court, rendered inadmissible, or used as grounds for a professional misconduct complaint against the doctor. These principles are therefore non-negotiable and apply uniformly to wound certificates, death certificates, fitness certificates, and every other medicolegal document the doctor signs.
Contemporaneous recording is the most important principle. A medicolegal document must be created at the time of or immediately after the examination — not hours or days later. A wound certificate written from memory the following morning is legally vulnerable because the defence will argue (often successfully) that the description was retrospectively crafted to support a particular version of events. The date and time of the examination must appear on the document. If there is any gap between the examination and the recording, that gap must be explained in the document itself.
Descriptive, not conclusory language is the second principle. The doctor's role in most medicolegal certificates is to describe objective findings — not to provide legal conclusions. In a wound certificate, the doctor writes: '2 × 0.5 cm laceration on the right parietal region of the scalp with irregular margins, tissue bridges present, 1 cm deep, exposing the galea.' The doctor does NOT write: 'injury caused by a blunt weapon' (unless this is directly inferable from the wound characteristics — in which case it should be stated as an opinion, not a finding). The legal classification of the injury — whether it constitutes 'simple hurt' or 'grievous hurt' under the BNS — is for the court to determine on the basis of the doctor's objective description. The doctor provides the raw data; the court provides the legal conclusion.
Original documents must be preserved and produced. A medicolegal document carries its full legal weight only in original form. If the doctor has issued multiple copies (for the police, the hospital record, and the patient), the court will typically ask for the original. The doctor must maintain a register of all medicolegal certificates issued, with date, patient name, certificate type, and serial number — this is the medicolegal register, which is an official hospital record.
Amendments and corrections must be made transparently. If an error is discovered in a medicolegal document, the correction must be made by striking through the incorrect text with a single line (so that the original text remains legible), writing the correct text above or beside it, and initialling and dating the correction. White-out or opaque correction fluid is absolutely prohibited in medicolegal documents — an obliterated entry implies deliberate concealment.
Chain of custody is especially important for forensic samples collected at the time of examination. Every specimen — blood, swabs, clothing, foreign material — must be labelled, sealed, signed across the seal by the doctor, and handed to the police officer with a receipt. If the chain of custody is broken at any point, the forensic value of the sample is compromised, and the defence may challenge its admissibility.
Latest NMC notifications and state directives must be incorporated. The National Medical Commission (NMC) and individual state health departments periodically issue circulars, standing orders, and notifications that modify documentation requirements — for example, specifying the format of wound certificates for sexual assault victims under POCSO protocols, or mandating specific reporting formats for deaths in custody. Doctors have a professional obligation to remain aware of and compliant with these notifications. Ignorance of a current notification is not a legal defence.
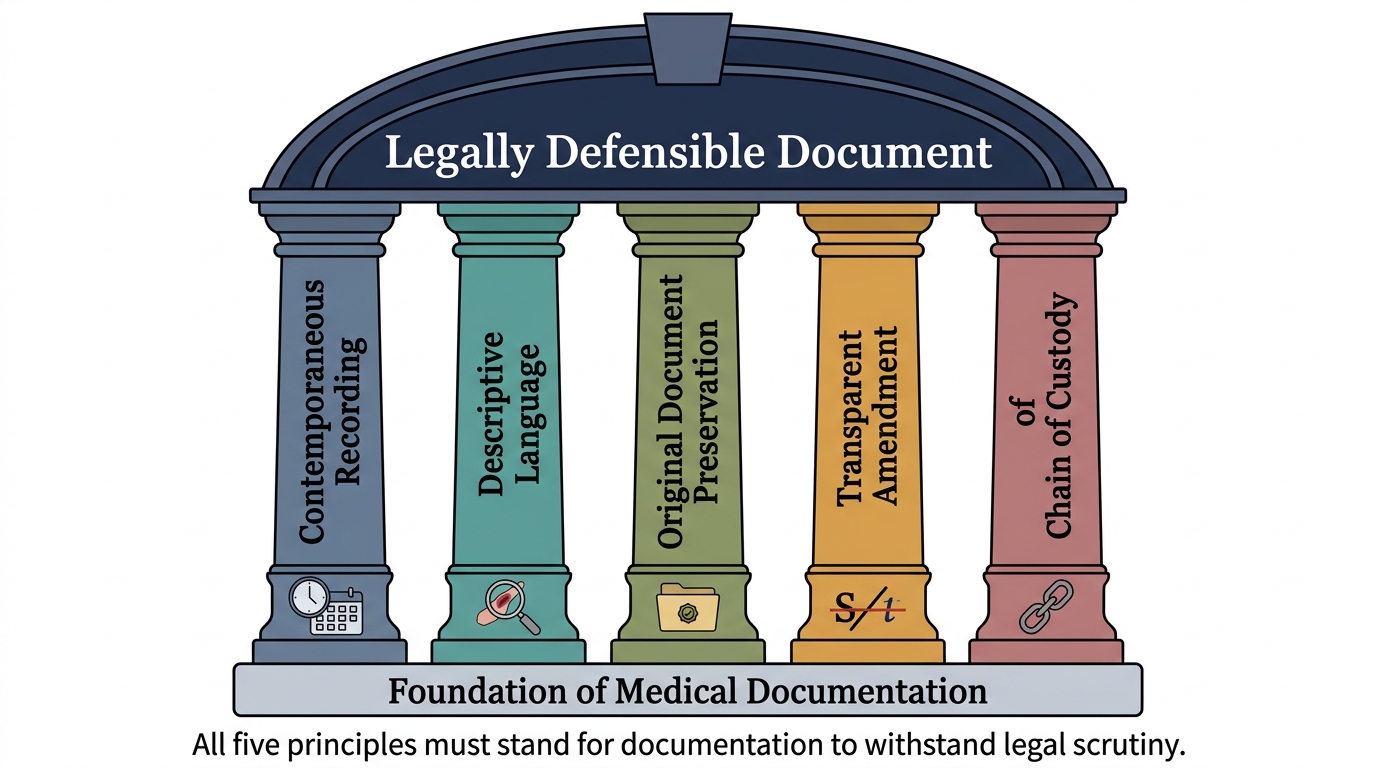
The Five Pillars of Legally Defensible Medicolegal Documentation
SELF-CHECK
A doctor issuing a wound certificate writes that the injury was 'definitely caused by a knife.' The defence lawyer challenges this statement in court. Which principle of medicolegal documentation has the doctor violated?
A. Contemporaneous recording — the statement implies it was written from memory
B. Descriptive language — stating a conclusion about the weapon rather than describing the wound's objective characteristics
C. Chain of custody — the weapon should have been seized and documented
D. Original document preservation — a copy was used in court instead of the original
Reveal Answer
Answer: B. Descriptive language — stating a conclusion about the weapon rather than describing the wound's objective characteristics
The principle violated is 'descriptive, not conclusory language.' The wound certificate must describe objective wound characteristics (shape, margins, dimensions, depth, tissue bridges, foreign material). The inference that a knife was used — rather than any other sharp-edged object — is a legal conclusion that may exceed the doctor's evidentiary scope unless the wound characteristics specifically support that particular weapon. The correct phrasing is: 'wound characteristics consistent with a sharp-edged weapon' or more specifically, if warranted: 'clean-edged incised wound with no tissue bridges, consistent with a sharp cutting edge.'
Wound Certificate, Drunkenness Certificate, and Sickness/Fitness Certificate
Three of the most commonly issued medicolegal certificates in general clinical practice are the wound certificate, the drunkenness certificate, and the sickness or fitness certificate. Each has a specific format, required content, and legal context. The doctor who issues these documents must understand what each is for and what it must — and must not — contain.
Provided image
Wound Certificate (Injury Certificate)
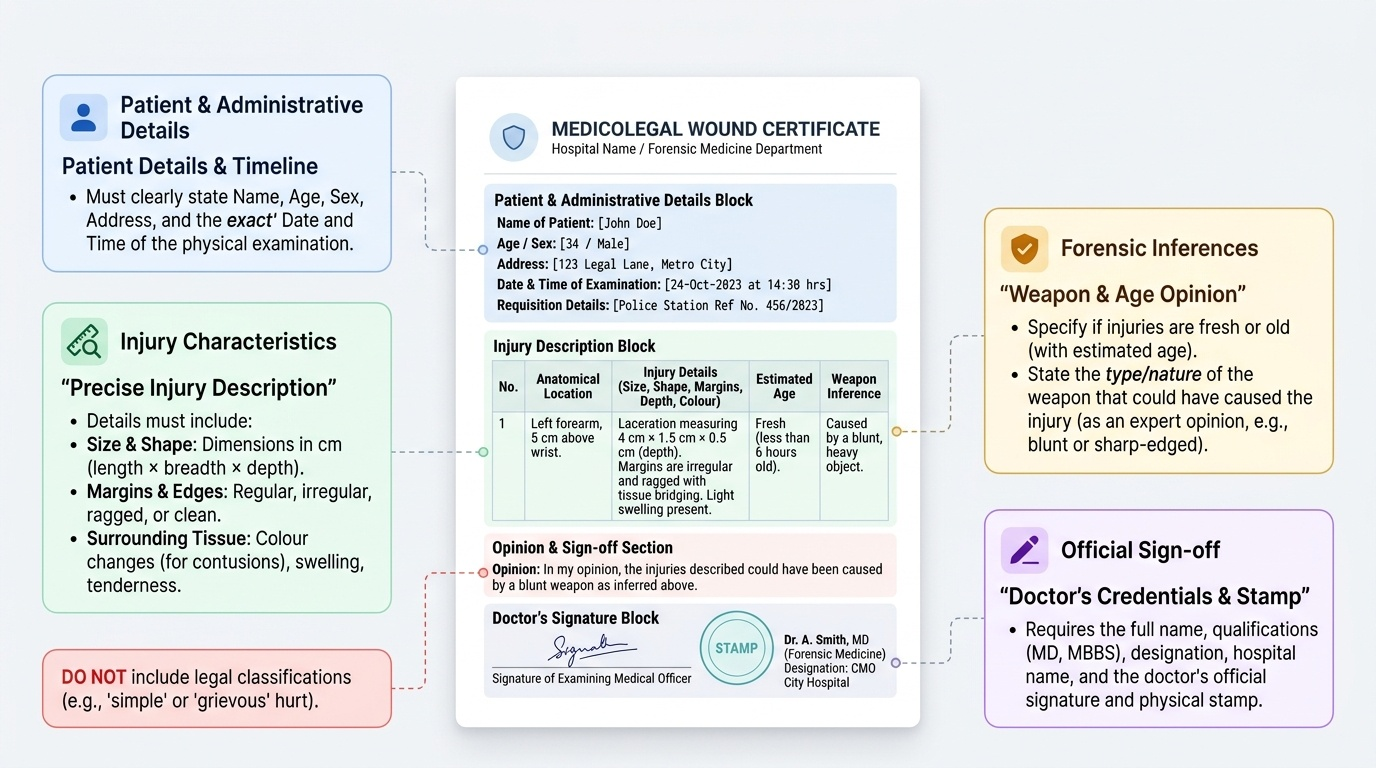
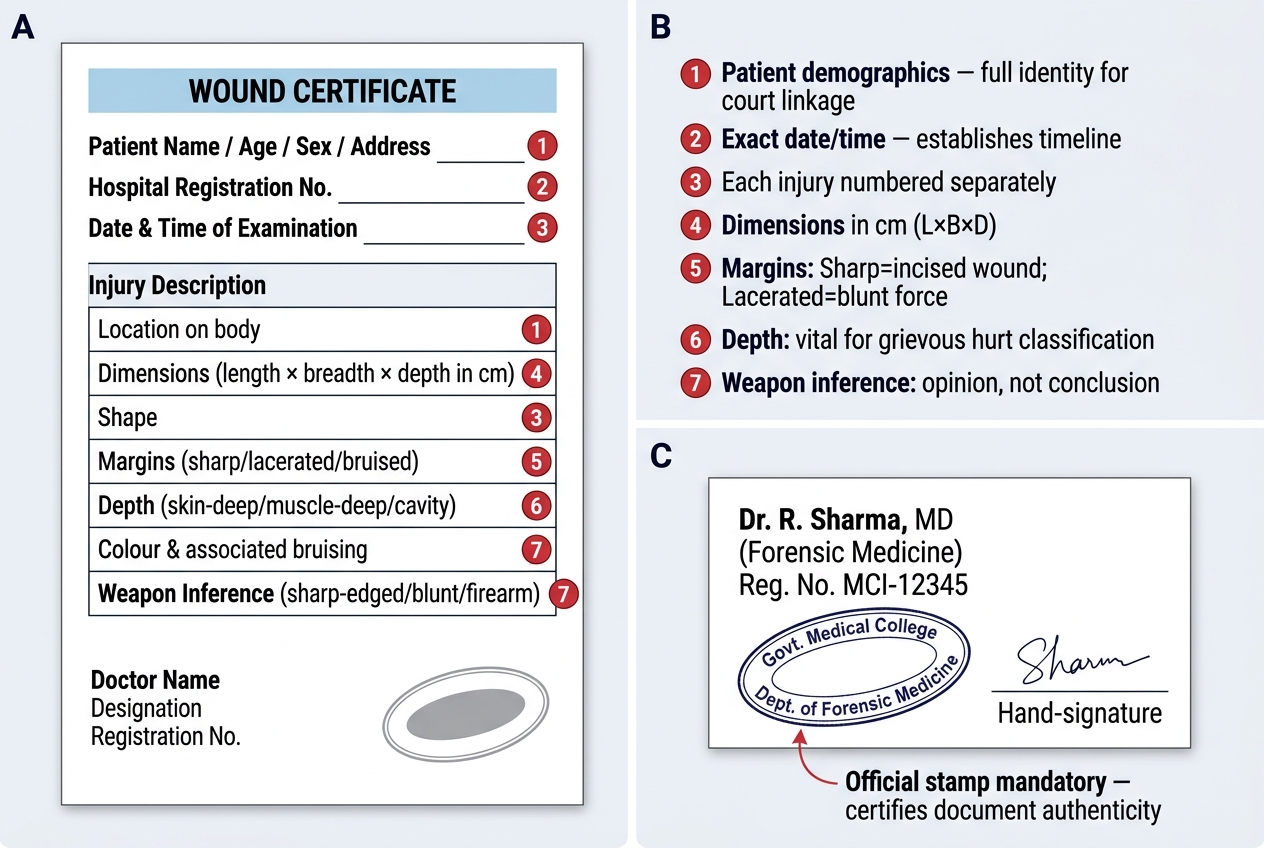
A wound certificate is issued following the medicolegal examination of a living person with injuries. It is the primary forensic document in cases of assault, road traffic accidents, and any other trauma with potential legal implications. The wound certificate is not a treatment record — it is a legal document produced in response to a police requisition or a direct patient request for a certificate to be used in legal proceedings.
The required content of a wound certificate includes:
- Patient's name, age, sex, address, and date/time of examination
- Examining doctor's name, qualification, designation, and hospital
- For each injury: precise location on the body (using anatomical landmarks), dimensions (length × breadth in centimetres), shape (round, oval, linear, irregular), nature (abrasion, contusion, laceration, incised wound — precisely classified), colour of surrounding tissue (for contusions), depth (superficial, deep, to bone), margins (regular or irregular), edges (clean or ragged), any tissue bridges (present or absent), any foreign material, and any associated findings (swelling, tenderness, bony tenderness)
- Whether the injury is fresh or old (with estimated age of injury if old)
- The nature and type of weapon that could have caused the injury, stated as an opinion
- Any medically significant associated findings (nerve damage, vascular injury, etc.)
- Whether the injuries could have been self-inflicted (opinion only, if asked)
The wound certificate does NOT include the legal classification of injury (that is for the court under BNS). It should NOT conclude 'grievous hurt' or 'simple hurt' — those are legal determinations. The doctor classifies wounds medically, and the court classifies them legally.
Drunkenness Certificate
A drunkenness certificate is issued when police request a medical officer to examine a person who is alleged to be under the influence of alcohol or drugs — typically in connection with offences under the Motor Vehicles Act or public order provisions. The doctor must assess and record: the general state of consciousness, speech, gait, coordination, breath (odour of alcohol), pupillary reactions, reflexes, and blood alcohol concentration if a blood sample is taken and tested. The doctor gives a clinical opinion on whether the person is, at the time of examination, 'under the influence' of alcohol or a substance.
A critical fact: India's Motor Vehicles Act threshold for blood alcohol concentration is 30 mg per 100 mL (0.03%) — NOT the 0.08% (80 mg/100 mL) figure used in the United States and United Kingdom. Stating the wrong threshold in a report is a significant factual error. A person is considered to be driving under the influence in India if the blood alcohol level exceeds 30 mg/100 mL. The doctor's certificate should state the measured value and compare it to this statutory threshold.
Sickness and Fitness Certificate
A sickness certificate certifies that a person is suffering from a specified condition that prevents them from attending work, court proceedings, or a specified function. A fitness certificate certifies that a person is medically fit for a specified purpose — return to work, resumption of driving, fitness to stand trial, fitness for marriage. These certificates are legally significant because they can affect employment decisions, court proceedings, and insurance claims. The doctor must have personally examined the patient before issuing either certificate; certificates issued without examination ('blank certificates') constitute professional misconduct under the NMC regulations and may constitute fraud.
Wound Certificate — Template Structure and Required Fields
| Certificate | Purpose | Who Requests | Key Required Content |
|---|---|---|---|
| Wound Certificate | Describe injuries for criminal/civil proceedings | Police or patient | Each injury: location, dimensions, type, depth, margins, weapon opinion |
| Drunkenness Certificate | Certify intoxication status for MV Act/public order | Police | Clinical signs, BAC (compare to 30 mg/100 mL threshold), clinical opinion |
| Sickness Certificate | Certify inability to attend work/court | Employer, court, patient | Diagnosis, period of incapacity, prognosis |
| Fitness Certificate | Certify medical fitness for specified purpose | Employer, court, insurance | Specific fitness assessed, any limitations |
Death Certification: MCCD Form 4 and Form 4A
Provided image
Death certification is one of the most important and most frequently incorrectly performed documentation tasks in clinical medicine. An accurate death certificate is essential for three reasons: it is the primary legal document authorising disposal of the body; it is the principal data source for national mortality statistics used in public health planning; and it may trigger police investigation of a death if the stated cause is inadequate, inconsistent, or suggests unnatural death.
India uses the Medical Certificate of Cause of Death (MCCD), which is issued in two forms:
Form 4 is issued for deaths occurring outside a hospital — in the community, at home, or in a place other than a registered medical institution. It is completed by the attending physician who last cared for the deceased prior to death. In the absence of any doctor having attended the deceased, the certificate is issued by the primary health centre or family health centre physician responsible for that geographic area. Form 4 is the more common form in rural practice.
Form 4A is issued for deaths occurring inside a hospital — in an in-patient setting, an emergency department, or any registered healthcare facility. It is completed by the medical officer responsible for the patient's care at the time of death or immediately prior to it. Form 4A includes additional sections for hospital-specific data.
The Causal Sequence Structure
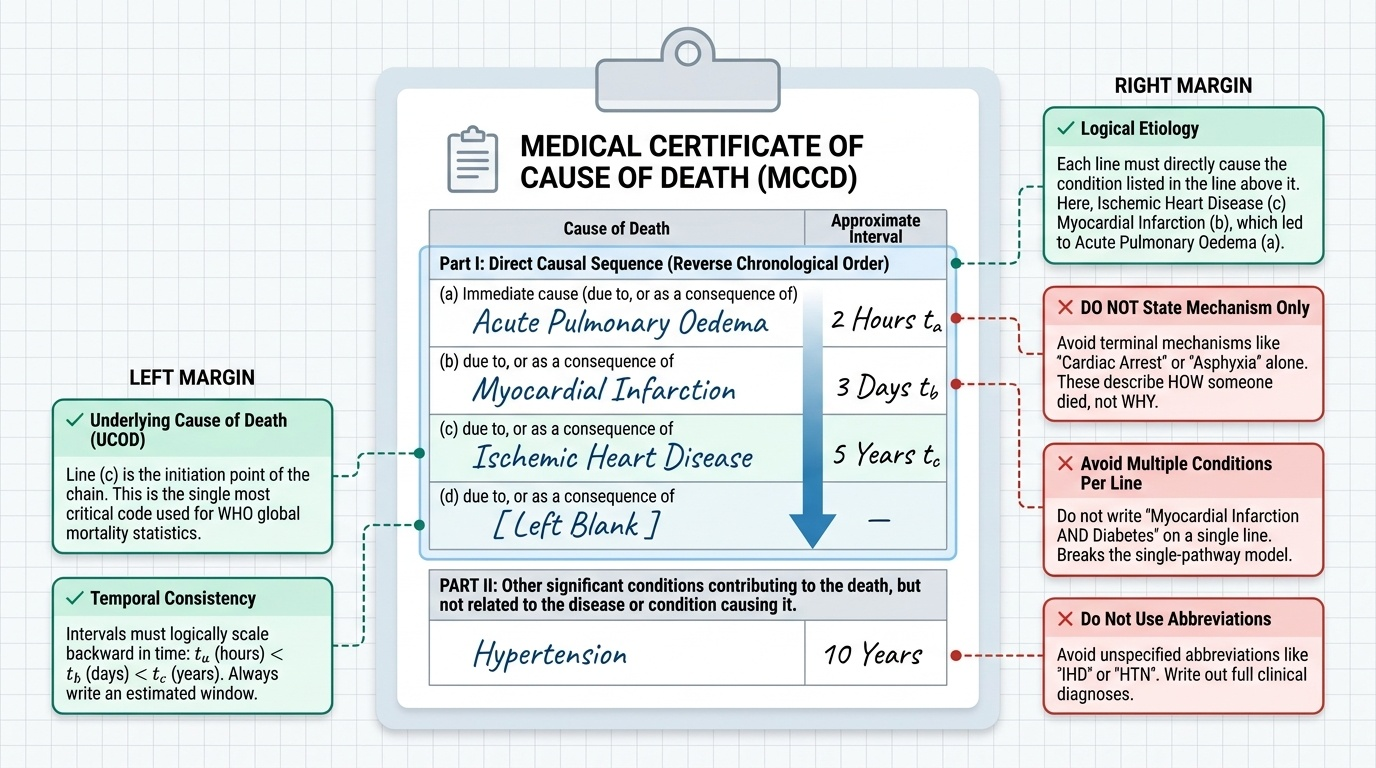
Both Form 4 and Form 4A follow the World Health Organization's standardised format for recording cause of death, which consists of two parts:
- Part I records the direct causal sequence leading to death, in reverse chronological order:
- Line (a): Immediate cause of death — the final pathological process that directly caused death
- Line (b): Antecedent cause — the condition that gave rise to (a)
- Line (c): Underlying cause — the fundamental condition that initiated the chain of events leading to (b) and ultimately to death
- Line (d): (If applicable) an even more remote underlying condition
- Part II records other significant conditions that contributed to death but were not part of the direct causal sequence
A correctly completed cause-of-death section for a patient with hypertension who developed ischemic heart disease, then had a myocardial infarction with fatal acute pulmonary oedema would be:
- Part I(a): Acute pulmonary oedema [immediate cause]
- Part I(b): Acute myocardial infarction [antecedent cause]
- Part I(c): Ischemic heart disease [antecedent cause]
- Part I(d): Hypertension [underlying/remote cause]
Common Errors That Trigger Investigation:
- Writing 'cardiac arrest' or 'respiratory failure' or 'shock' as the cause of death — these are modes of dying (the mechanism of the final event), not diagnoses. They answer 'how did the heart stop?' but not 'why did the heart stop?' Every death involves cardiac arrest at the end; writing it as a cause of death provides no information and triggers a registrar query or police investigation.
- Leaving lines blank in Part I — if only one underlying cause is known, it goes on line (c); lines (a) and (b) describe the pathological progression from that cause.
- Writing abbreviations — IHD, AMI, COPD — without confirming the registrar uses the same conventions; use full International Classification of Diseases (ICD) terms.
- Failing to complete Part II — a patient with both ischemic heart disease and diabetes who dies of hypertensive encephalopathy has diabetes as a Part II contributing condition; omitting it distorts mortality statistics.
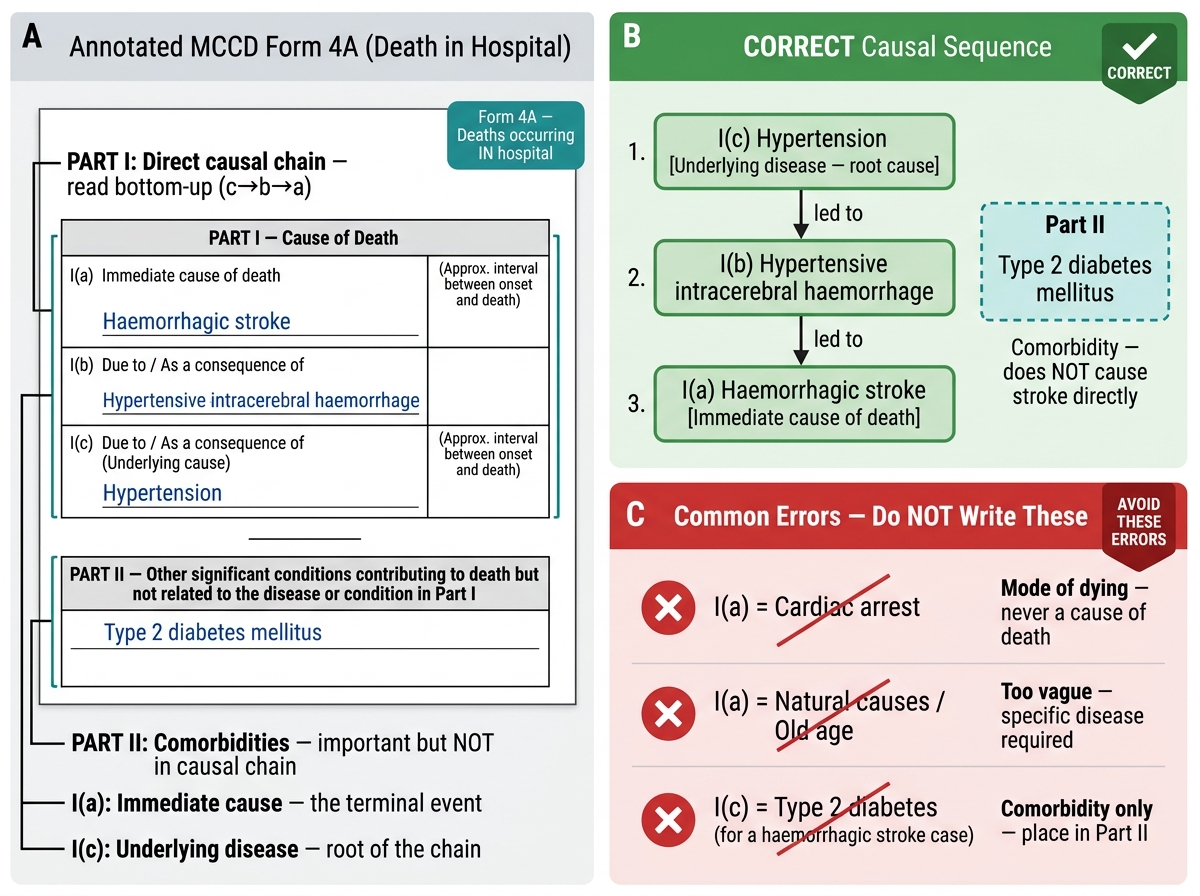
MCCD Death Certificate: Annotated Layout, Correct Causal Sequence, and Common Errors
SELF-CHECK
A 58-year-old male patient with known type 2 diabetes and hypertension dies in hospital from a haemorrhagic stroke. Which MCCD form is used, and what is the MOST appropriate entry for Part I(c) in the causal sequence?
A. Form 4; Part I(c) = Cardiac arrest
B. Form 4A; Part I(c) = Hypertension
C. Form 4; Part I(c) = Hypertension
D. Form 4A; Part I(c) = Type 2 diabetes
Reveal Answer
Answer: B. Form 4A; Part I(c) = Hypertension
The patient died in hospital, so Form 4A is used (Form 4 is for deaths outside hospital). In the causal sequence for a haemorrhagic stroke: Part I(a) = haemorrhagic stroke (immediate cause); Part I(b) may be hypertensive intracerebral haemorrhage; Part I(c) = hypertension (the underlying disease driving the stroke risk). Type 2 diabetes would appear in Part II as a contributing condition (important comorbidity, but not in the direct causal chain for haemorrhagic stroke). 'Cardiac arrest' must never appear as a cause of death — it is a mode of dying.
Age Estimation Certificate and Latest Decisions/Notifications
Two components complete the medicolegal documentation framework for a Year-2 physician: the age estimation certificate — required in specific forensic contexts — and the ongoing obligation to stay current with notifications and circulars that modify documentation standards.
Age Estimation Certificate
An age estimation certificate is a formal medicolegal opinion on a person's chronological age, based on clinical and radiological examination, issued when documentary evidence of age (birth certificate, school certificate) is unavailable or disputed. The age estimation certificate is most commonly requested in two forensic contexts:
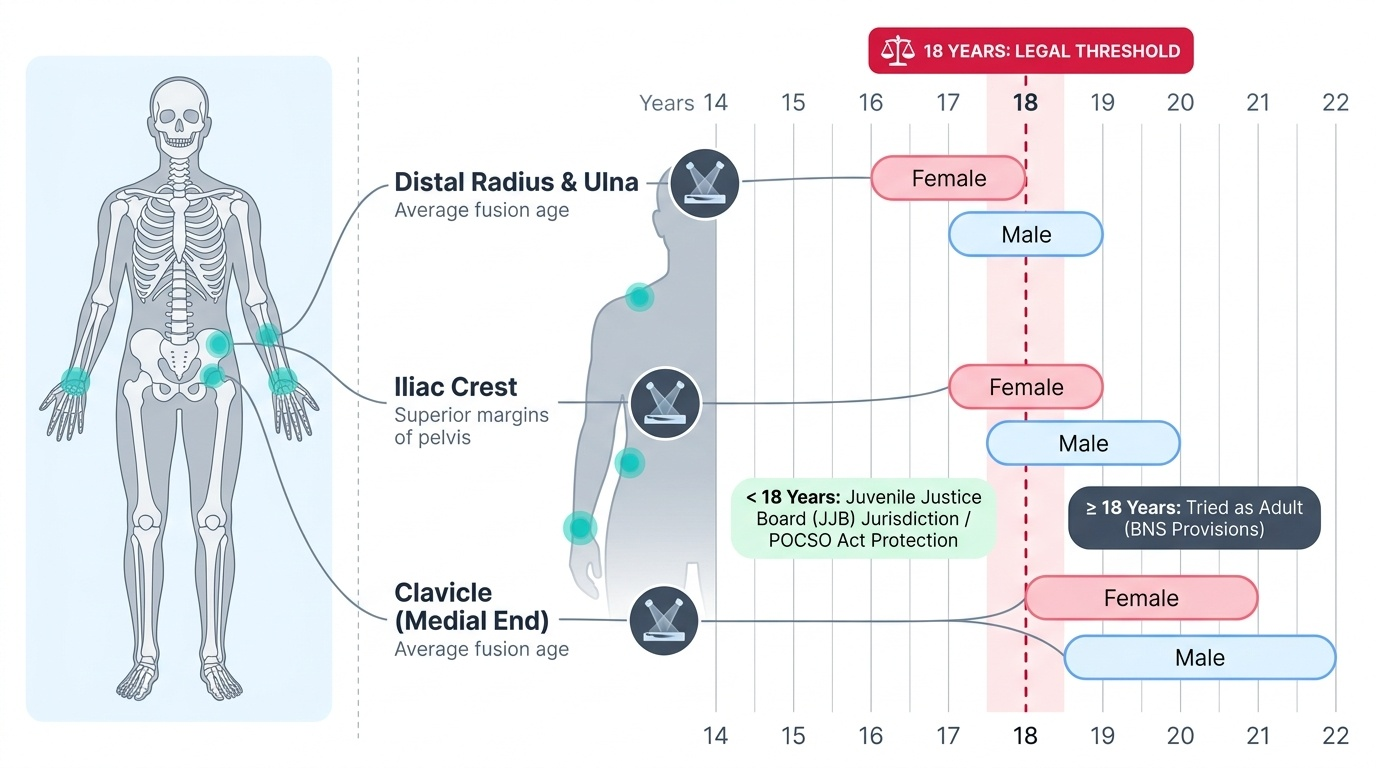
- Juvenile Justice Board proceedings: when the accused claims to be a juvenile (under 18 at time of alleged offence) but documentary proof is unavailable or disputed. The JJB may order an ossification test and clinical age estimation, and the forensic opinion determines whether the person is tried as a juvenile or an adult.
- POCSO and sexual offence cases: where the age of the victim determines the applicable statute and sentencing — offences against persons under 18 attract POCSO provisions, which are more stringent than BNS provisions for adults.
The clinical and radiological criteria used in age estimation include: dental eruption and development, secondary sexual characteristics, height and weight parameters, and most importantly ossification of specific epiphyses — the fusion of growth plate centres at predictable ages. Reddy's FM&T provides Indian reference values for the key epiphyseal fusion ages; these are the values that must be used in Indian forensic contexts, not Western atlas values. The final age opinion must be expressed as a range (e.g., 'between 16 and 20 years') — an exact age cannot be certified from biological markers; doing so implies false precision and is scientifically indefensible.
Provided image
Latest Decisions, Notifications, Resolutions, and Standing Orders
The doctor's medicolegal documentation obligations do not exist in a static regulatory environment. The National Medical Commission (NMC), formerly the Medical Council of India (MCI), periodically issues notifications that update documentation requirements. State governments issue health department circulars about reporting obligations for specific diseases, crimes, or circumstances. The BNSS 2023 itself introduced new provisions compared to the CrPC 1973. Courts — particularly the Supreme Court and High Courts — issue judgements that clarify or expand the standards doctors must meet.
Key examples of documented obligations arising from recent notifications and circulars:
- The NMC Act 2020 and associated regulations require that doctors maintain contemporaneous and complete medical records for all patients, with specific standards for retention periods and patient access rights.
- POCSO regulations and MCI/NMC circulars have specified examination protocols and documentation standards for child sexual assault victims, including the prohibition of the 'two-finger test' (vaginal laxity testing in sexual assault — declared unscientific and violating dignity by the Supreme Court and a Ministry of Health circular).
- The Supreme Court in Lillu alias Rajesh vs State of Haryana (2013) held that the two-finger test violates the right to privacy and dignity of the survivor; MHA circular thereafter prohibited it — the examining doctor must not perform this test.
- BNSS 2023 inquest standing orders from state police headquarters specify the documentation format for police inquest reports that involve medical officer involvement.
- State public health acts may require notification of specific injuries (e.g., burn injuries above a specified percentage BSA in some states) to the Collector or CMO.
The practical implication for the doctor is clear: subscribe to NMC communication channels, maintain awareness of state health department circulars, and periodically verify that institutional medicolegal documentation formats are consistent with current requirements. A format used by the hospital since 2015 may not meet 2023 BNSS or NMC requirements.
SELF-CHECK
A person alleged to have committed a rape is brought before the Juvenile Justice Board, claiming to be 16 years old. No birth certificate or school record is available. The JJB orders a forensic age estimation. Which of the following is the CORRECT way for the forensic physician to state the age opinion in the certificate?
A. 'The subject is exactly 17 years old based on ossification findings'
B. 'The subject is between 16 and 20 years of age based on clinical and ossification criteria'
C. 'The subject is a minor (under 18 years)' without specifying a range
D. 'Age estimation is not possible without documentary evidence'
Reveal Answer
Answer: B. 'The subject is between 16 and 20 years of age based on clinical and ossification criteria'
Age from biological markers must always be expressed as a range — e.g., 'between 16 and 20 years' — because biological age markers have inherent population variability and cannot give an exact chronological age. Stating an exact age implies false precision and is scientifically indefensible. Stating only 'minor' without a range is insufficient for the JJB to determine whether the person falls below the critical 18-year threshold. Age estimation from ossification is scientifically valid and should not be declined simply because documentary evidence is absent — that is precisely the circumstance for which it exists.
CLINICAL PEARL
The two most common and consequential errors in medicolegal documentation are: (1) writing 'cardiac arrest' as a cause of death on the MCCD — never do this; always state the underlying disease process; and (2) failing to certify the date and time of examination on wound certificates — this is the single most effective point of attack for a defence lawyer challenging whether the injuries were present at the time of the alleged offence. Train yourself to write the date, time, and your signature on every medicolegal document as the first act — before even beginning to describe the findings.
KEY TAKEAWAYS
All medicolegal documents share five foundational principles: contemporaneous recording, descriptive (not conclusory) language, original document preservation, transparent amendment, and chain of custody for forensic samples. Doctors must maintain a medicolegal register (official hospital record of all certificates issued).
The wound certificate describes injuries objectively — location, dimensions, type, depth, margins, weapon inference (as opinion) — without legal classification. The drunkenness certificate assesses clinical signs of intoxication and compares blood alcohol to India's Motor Vehicles Act threshold of 30 mg/100 mL. The sickness/fitness certificate certifies current health status for a specific purpose.
Death certification uses MCCD Form 4 (deaths outside hospital) and MCCD Form 4A (deaths in hospital). Both require a causal sequence: Part I (immediate → antecedent → underlying cause) and Part II (contributing conditions). 'Cardiac arrest' must never appear as a cause of death.
The age estimation certificate expresses age as a range based on ossification and clinical criteria (Indian reference values from Reddy's). Doctors must incorporate the latest NMC notifications, state circulars, BNSS standing orders, and Supreme Court directives (including prohibition of the two-finger test in sexual assault examinations) into their documentation practice.
REFLECT
Think of a death you may have witnessed during your clinical posting — or imagine one you are likely to encounter. What was (or would be) the immediate cause of death? What was the underlying disease? Could you correctly fill in the MCCD causal sequence right now? If you are uncertain, that uncertainty is the most productive starting point: go back to the causal sequence structure and practice it with three or four different disease trajectories until the format is automatic. Medicolegal documentation is a skill like any other — it requires deliberate practice. The cost of not practising is measured in corrupted statistics and flawed justice.