Page 9 of 23
FM10.{4-5,28} | Code of Medical Ethics & Professional Misconduct — SDL Guide (Part 2)
The Disciplinary Mechanism: Warning, Erasure and Restoration
When a complaint of professional misconduct is made against a registered practitioner, the disciplinary process follows a defined pathway. Understanding this pathway — and the precise distinction between a warning notice and penal erasure — is essential for the examination.
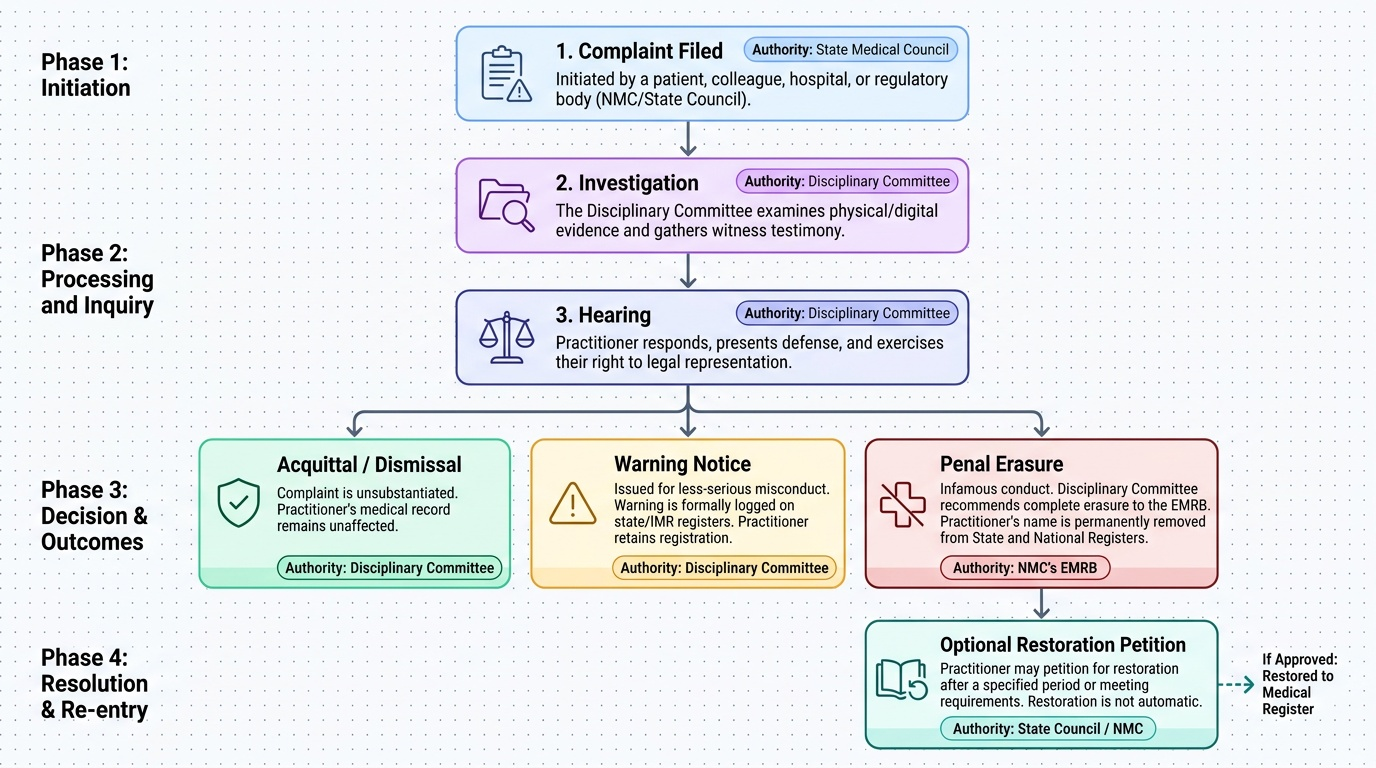
Initiation of disciplinary proceedings: A complaint may be made by a patient, a colleague, a hospital, or the regulatory body itself (NMC or State Medical Council). The complaint is received by the State Medical Council in whose jurisdiction the practitioner is registered. The Council's Disciplinary Committee investigates the complaint.
Investigation by the Disciplinary Committee: The Committee examines evidence, may call witnesses, and hears the practitioner's response. The practitioner has the right to be represented and to present their defence. The Committee's proceedings are quasi-judicial.
Possible outcomes of disciplinary proceedings:
1. Acquittal / Dismissal: The complaint is found to be unsubstantiated or the conduct is found not to amount to professional misconduct. The practitioner's record is unaffected.
2. Warning Notice: If the conduct is found to constitute professional misconduct of a less serious nature — below the threshold of infamous conduct — the Committee may issue a warning notice. The warning is placed formally on the practitioner's record in the State Medical Register and the IMR. The practitioner retains their registration — they remain on the register — but the warning is a public record that the practitioner has been found to have breached professional standards. It may affect future disciplinary proceedings (repeated warnings can lead to escalated consequences).
3. Penal Erasure: If the misconduct is found to constitute infamous conduct in a professional respect, the Committee recommends penal erasure of the practitioner's name from the State Medical Register. The recommendation is referred to the NMC's EMRB for the national register. Penal erasure is:
- Removal from the medical register — the practitioner is no longer a registered medical practitioner
- Permanent unless restored — the practitioner may petition for restoration after a defined period or upon satisfying conditions; restoration is not automatic
- Public — the erasure is recorded and the practitioner cannot hold themselves out as a registered medical practitioner during the period of erasure
- Distinct from a warning notice — erasure and warning are NOT interchangeable; erasure removes registration, warning maintains it
4. Restoration: A practitioner who has been erased may apply for restoration to the register. The Disciplinary Committee considers the application and may restore the name if satisfied that the conditions (if any) have been met and the practitioner is fit to resume practice.
Provided image
SELF-CHECK
Dr. P is found by the State Medical Council's Disciplinary Committee to have committed professional misconduct by issuing false fitness certificates for payment. The Committee recommends penal erasure. Which of the following correctly describes the effect of penal erasure?
A. Dr. P receives a formal warning on his record but retains his registration
B. Dr. P is suspended from practice for one year and then automatically reinstated
C. Dr. P's name is removed from the medical register; he cannot practise until and unless restored by application
D. Dr. P loses his MBBS degree and must re-qualify to practise
Reveal Answer
Answer: C. Dr. P's name is removed from the medical register; he cannot practise until and unless restored by application
Penal erasure removes the practitioner's name from the medical register — the State Medical Register and the Indian Medical Register. The practitioner may not practise medicine during the period of erasure. Restoration is possible by application but is not automatic. Penal erasure does NOT cancel the degree — it cancels the registration. A warning notice (option A) is a different, less severe outcome where registration is retained but a warning is placed on record.
Applied Practice: Recognising and Responding to Ethical Violations
Understanding the Code is not just about avoiding personal violations — it is about recognising and responding appropriately when ethical violations occur in your working environment. Medical practice occurs in institutional contexts — hospitals, clinics, academic departments — where informal norms can diverge from the Code's requirements, and where the normalisation of violations ('everyone does it') creates moral hazard.
Practical compliance with the Code requires:
At the individual practice level:
- Never accept referral fees or commissions from diagnostic centres, pharmaceutical representatives (beyond items of nominal value), or other practitioners
- Never advertise your services in a commercially promotional way — factual information about your practice location and qualifications is permissible
- Never sign prescriptions, certificates, or other documents on behalf of an unregistered person
- Ensure that any certificate you sign is medically accurate — false certificates can result in erasure and criminal prosecution
- Decline requests from pharmaceutical companies for endorsements of specific products
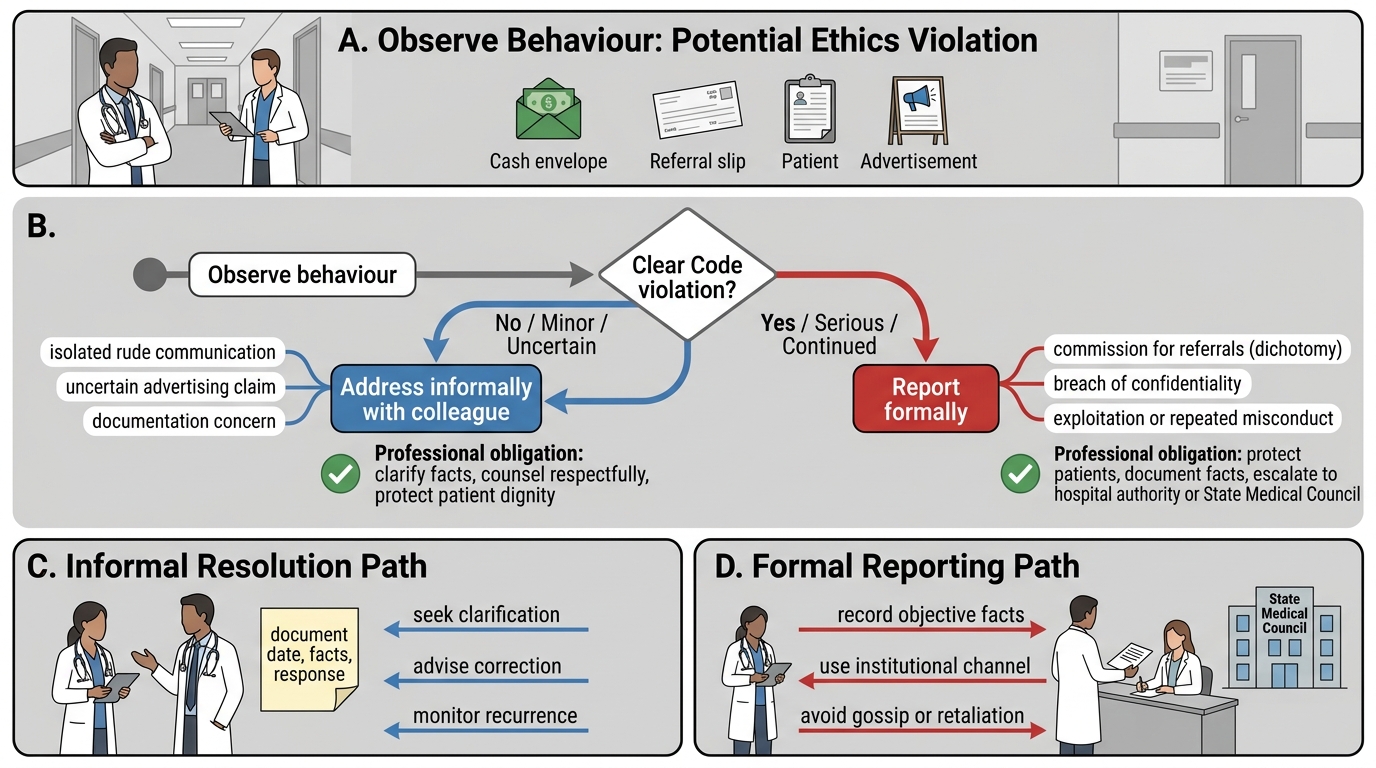
When you encounter violations by colleagues:
The NMC Code creates an implicit professional obligation to address violations within the profession rather than enabling them through silence. You are not legally required to report a colleague's misconduct in all circumstances, but:
- You must not actively conceal or enable a colleague's misconduct
- You should initially attempt to address concerns informally with the colleague (for minor violations)
- Serious violations (patient harm, continued misconduct despite warning, criminal conduct) should be reported to the State Medical Council or hospital authorities
- Whistleblowing is professionally legitimate and should not be conflated with disloyalty to the profession
Documentation as ethical practice:
The Code implicitly requires adequate clinical documentation. Accurate records protect both the patient and the practitioner — they are the primary evidence in any disciplinary or legal proceeding. An undocumented consent, an undocumented clinical decision, or an incomplete record is not merely a professional failing; it removes the evidence that would demonstrate the practitioner acted appropriately.
Responding to a Colleague's Ethics Violation
SELF-CHECK
Under the NMC Code of Medical Ethics 2002, a registered medical practitioner may NOT:
A. Inform a patient about their right to seek a second opinion
B. Receive a commission payment from a diagnostic imaging centre for referring patients
C. Display a factual notice outside their clinic stating their name, qualifications, and specialty
D. Refuse to treat a non-emergency patient who cannot pay
Reveal Answer
Answer: B. Receive a commission payment from a diagnostic imaging centre for referring patients
Receiving a commission for patient referrals is dichotomy — specifically prohibited under the Code as professional misconduct. The other options are either permissible or in some cases required: informing patients of their right to a second opinion is good practice; displaying factual information about one's qualifications is permitted (commercial advertising is not); and while there is a duty to provide emergency treatment regardless of ability to pay, refusal to treat non-emergency patients who cannot pay in advance is not itself a prohibited act under the Code (though hospital policies vary).
CLINICAL PEARL
The 'everyone does it' rationalisation is the most common precursor to a disciplinary finding. Fee-splitting and dichotomy have become normalised in segments of Indian private healthcare — which is precisely why the NMC Code's prohibition is not an archaic formality but an active regulatory concern. When a senior colleague tells you that a particular arrangement is 'standard practice,' the correct response is to verify whether it is consistent with the Code before participating. Participation in an arrangement does not become ethical because the arrangement is widespread. The disciplinary committee's standard is not 'what everyone does' but 'what a registered medical practitioner with integrity would do.'