Page 1 of 23
FM10.1 | Medical Ethics: History & Emergence — SDL Guide
Learning Objectives
- Describe the nature and scope of medical ethics as a discipline
- Trace the historical emergence of medical ethics from ancient traditions to contemporary frameworks
- Identify the key milestones: Hippocratic tradition, Nuremberg Code, Declaration of Helsinki, Belmont Report, and Declaration of Geneva
- Explain the relevance of historical ethical milestones to current Indian medical practice under the NMC framework
INSTRUCTIONS
Medical ethics is not a modern invention — it is as old as the healing relationship itself. Every time a doctor decides how much to tell a patient, whether to prioritise one patient over another, or how to navigate a conflict between a patient's wishes and their wellbeing, they are engaging with questions that physicians have grappled with across millennia and across cultures. Understanding where medical ethics came from — why it was formalised, what crises drove its development, and how it reached its current form — is essential for any doctor who intends to practise with integrity rather than mere compliance.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 1946. In the ruins of post-war Germany, a courtroom in Nuremberg is hearing testimony that will change medicine forever. Twenty-three Nazi physicians stand trial for crimes committed in the name of medical science — hypothermia experiments on prisoners, high-altitude pressure trials, deliberate infection with tuberculosis. The defendants argue that the experiments were scientifically valuable and that the distinction between prisoners and soldiers is merely political. The judges are unmoved. Their verdict — and the ten principles they articulate afterward in what becomes the Nuremberg Code — establishes for the first time in modern law that no medical experiment may be conducted without the voluntary consent of the subject. Medicine, it turns out, had needed to learn this lesson the hard way. But how did we reach a world where doctors could believe such conduct was acceptable? And how do the frameworks that arose in response to these atrocities connect to the oath you will take at your own graduation? This module traces that history.
WHY THIS MATTERS
For a medical student in India in 2026, medical ethics might seem like a theoretical subject — a box to tick before the clinical years. But every ethical framework you will encounter in your career — informed consent, confidentiality, research ethics, end-of-life decisions — has a specific historical origin. Understanding those origins tells you not just what the rules are, but why they exist and why they matter. The NMC Code of Medical Ethics 2002, which governs your practice under the NMC Act 2020, did not appear from nowhere. It inherits from centuries of ethical thinking that began with the Hippocratic tradition, was tested by 20th-century atrocities, and was codified through international consensus documents that Indian medical regulators explicitly adopted. A doctor who understands this history is far better equipped to apply these principles thoughtfully than one who merely memorises the rules.
RECALL
Before we begin, take a moment to recall what you know:
- What is the difference between ethics (principles of right and wrong) and law (enforceable rules)? Can something be legal but unethical? Can something be illegal but ethical? Give one example of each.
- You have heard of the 'Hippocratic Oath' — what do you actually know about its content? What does a doctor swear to, and when was it written?
- Think about a situation in medicine where a doctor's interests (in knowledge, in efficiency, in convenience) might conflict with the patient's interests. How has society addressed this tension historically?
Legal and Professional Context: Why Medical Ethics Exists
Medical ethics exists because the healing relationship is fundamentally asymmetric. A patient in distress, often in pain or fear, approaches a practitioner who possesses specialised knowledge, technical skill, and institutional authority that the patient does not have. This asymmetry creates the possibility of exploitation — whether through dishonesty, indifference, financial manipulation, or outright harm. The history of medicine is, in part, a history of that asymmetry being exploited, and a corresponding history of the frameworks that arose to prevent or redress that exploitation.
The relationship between medicine and ethics is not simply that ethics constrains what doctors can do. It is deeper than that: the very concept of a profession — as opposed to a trade or a craft — rests on an ethical commitment. A profession makes a social contract with the public: in exchange for autonomy, status, and economic privilege, the profession commits to prioritising the interests of those it serves above its own. Medical professionalism is, at its core, the expression of that ethical commitment in day-to-day clinical practice.
From a legal perspective, this ethical commitment is operationalised through regulatory bodies. In India, the National Medical Commission (NMC) under the NMC Act 2020 has the authority to set the standards of professional conduct and to discipline practitioners who breach them. But the NMC Code of Medical Ethics is not merely a legal instrument — it codifies ethical standards that predate any statute and that derive their authority from their intrinsic reasonableness, not merely from legislative mandate.
Key distinctions to hold:
- Ethics = the principles of right and wrong that guide conduct; may or may not be enforced by law
- Medical law = legally enforceable rules governing medical practice; violation carries legal consequences
- Medical jurisprudence = the application of law to medicine; the discipline that bridges these two domains
- Bioethics = the systematic study of ethical questions raised by biology, medicine, and healthcare
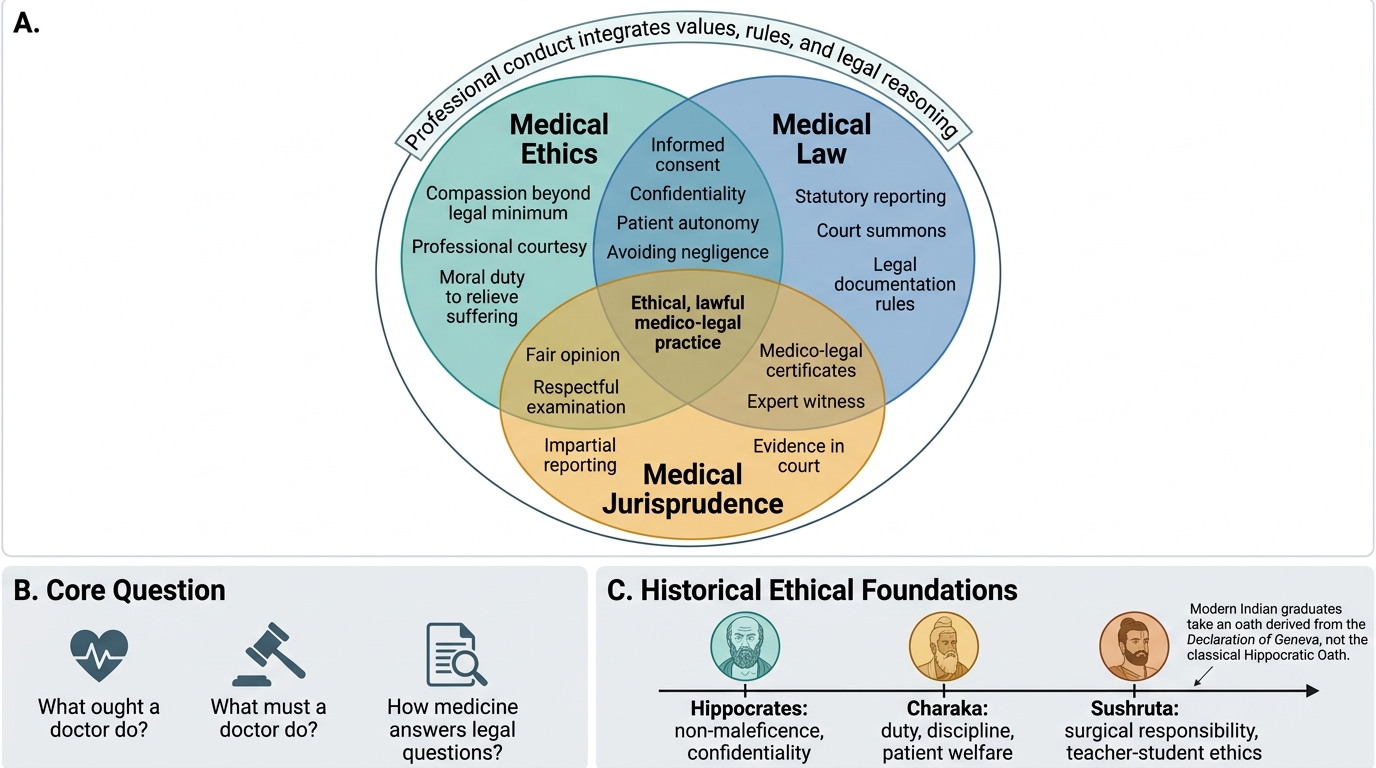
Medical Ethics, Law, and Jurisprudence
Ancient Medical Ethics: Hippocrates, Charaka, and Sushruta
The idea that medicine carries special ethical obligations is ancient. Across cultures and millennia, healers recognised that their special access to the suffering body created duties that went beyond technical skill. Three traditions stand out as foundational: the Greek Hippocratic tradition, and the Indian traditions represented by the Charaka and Sushruta Samhitas.
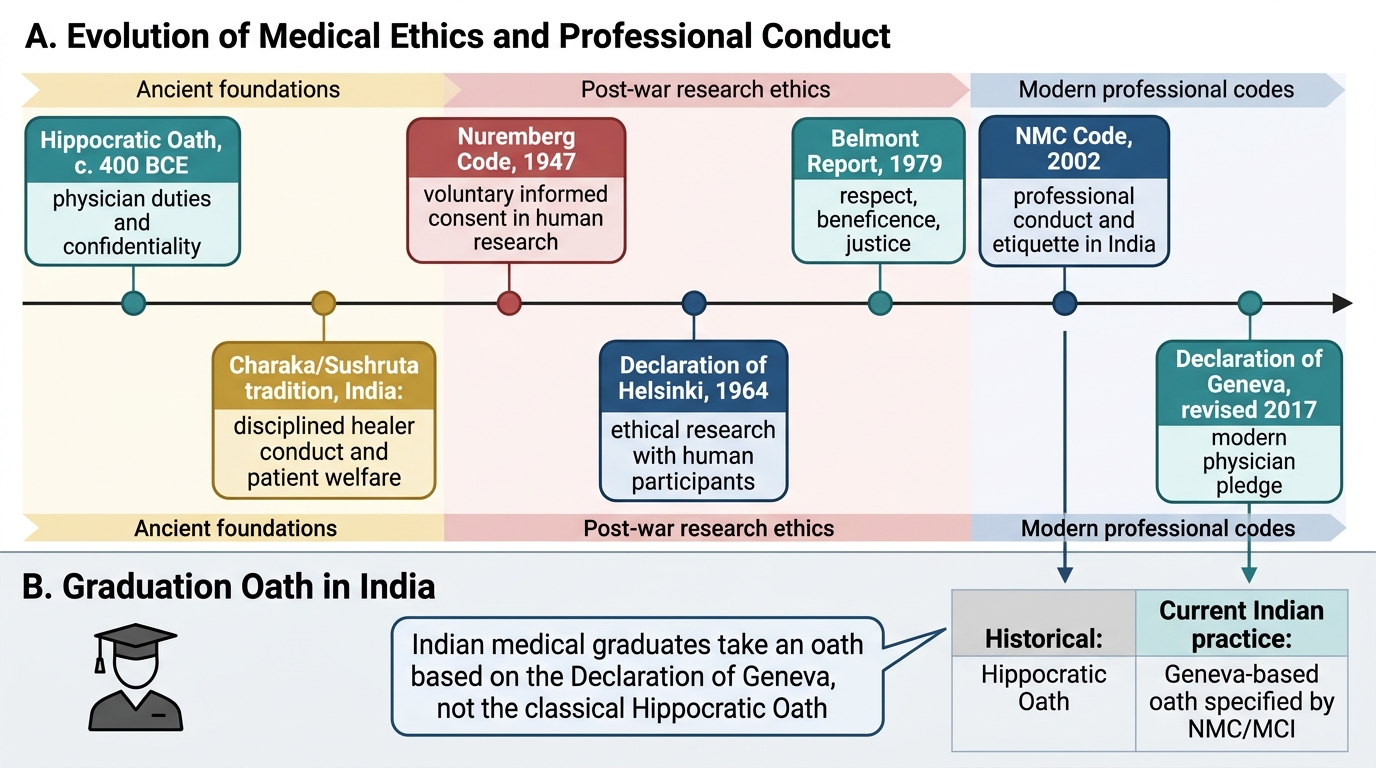
The Hippocratic Oath, attributed to Hippocrates of Cos (~460–370 BCE), is the most famous medical ethical text in Western history. In its classical form, the oath invokes Greek gods, establishes a duty of care to patients, prohibits causing harm (the primum non nocere principle), requires confidentiality, and prohibits sexual relations with patients and their households. It also famously forbids giving a 'deadly drug' or performing abortions — provisions that reflect the specific moral universe of ancient Greece rather than universal principles. The Hippocratic Oath was NOT a uniform requirement in ancient Greece; it was one school's ethical commitment. Crucially, modern Indian medical graduates do NOT take the Hippocratic Oath — they take an oath derived from the Declaration of Geneva (discussed below). The Hippocratic tradition is historically significant but must not be confused with current practice.
The Charaka Samhita (~200 BCE), one of the foundational texts of Ayurveda, contains a detailed ethical code for physicians. The initiation ceremony described in the Charaka Samhita includes an oath to devote oneself to the welfare of patients, to avoid harm, to maintain confidentiality, and to treat all patients regardless of their status. These principles are strikingly parallel to Hippocratic ethics, suggesting that the ethical demands of the healing relationship generate similar responses across independent traditions.
Sushruta, the ancient Indian surgeon whose Sushruta Samhita describes surgical techniques of remarkable sophistication for their era, also articulated ethical guidelines for surgeons, emphasising purity of motive, patient welfare, and the primacy of the patient's interests over the practitioner's convenience or gain.
These ancient traditions share several core themes:
- The duty to prioritise patient welfare
- The obligation of confidentiality
- The prohibition on causing harm
- The importance of professional humility and continued learning
Evolution of Medical Ethics and the Indian Medical Oath
SELF-CHECK
A student states: 'Indian medical graduates take the Hippocratic Oath at their graduation ceremony.' Is this statement correct?
A. Yes — the Hippocratic Oath is the universal medical oath administered worldwide
B. No — Indian graduates take an oath based on the Declaration of Geneva
C. No — Indian graduates take the Charaka Samhita oath as it is the Indian tradition
D. Yes — the Hippocratic Oath was adopted by the IMC (now NMC) for Indian graduates
Reveal Answer
Answer: B. No — Indian graduates take an oath based on the Declaration of Geneva
Indian medical graduates take an oath derived from the Declaration of Geneva (WMA, 1948; revised 2017), not the Hippocratic Oath. The Hippocratic Oath is historically significant but contains references to Greek pagan gods and specific prohibitions (e.g. against surgery) that make it unsuitable as a modern medical pledge. The NMC (formerly MCI) specifies a Declaration of Geneva-based oath for graduation ceremonies.
Modern Formalisations: Nuremberg to Helsinki
The 20th century brought medicine's ethical foundations under severe stress. The most catastrophic breach came in Nazi Germany, where physicians — including some of considerable professional standing — conducted experiments on concentration camp prisoners without consent, causing suffering and death in the name of scientific advancement. The Nuremberg Doctors' Trial (1946–1947) prosecuted twenty-three of these physicians; sixteen were convicted, and seven were executed. The judgment articulated what became known as the Nuremberg Code (1947) — ten principles that established the ethical basis for human experimentation.
The Nuremberg Code's first and most fundamental principle is that the voluntary consent of the human subject is absolutely essential. This single requirement — voluntary, informed, competent consent — had not previously been codified in international law, and its articulation in the Nuremberg Code marks one of the most important moments in the history of medical ethics. The Code also requires that research must be scientifically sound, that unnecessary suffering must be avoided, that risk must not exceed humanitarian benefit, and that subjects must be free to withdraw at any time.
Despite the Nuremberg Code, unethical research continued. The Declaration of Helsinki (1964), adopted by the World Medical Association (WMA), extended and refined the Nuremberg Code's principles specifically for clinical research. It distinguished between therapeutic and non-therapeutic research, emphasised the responsibility of the investigator, and required review by an independent ethics committee. The Declaration of Helsinki has been revised multiple times (most recently 2013) and remains the foundational international document for research ethics.
In the United States, the revelation of the Tuskegee Syphilis Study (1932–1972) — in which African-American men with syphilis were deliberately denied treatment even after penicillin became available, so that researchers could observe disease progression — shocked the public and led to the Belmont Report (1979). The Belmont Report, produced by the US National Commission for the Protection of Human Subjects, articulated three fundamental ethical principles: respect for persons (autonomy + informed consent), beneficence (maximise benefits, minimise harms), and justice (fair distribution of research burdens and benefits). These three principles from the Belmont Report are the direct predecessors of the four-principle framework developed by Beauchamp and Childress, which forms the basis of contemporary bioethics.
| Document | Year | Trigger | Key Contribution | Status |
|---|---|---|---|---|
| Nuremberg Code | 1947 | Nazi Doctors' Trial | Voluntary consent as absolute requirement | Foundational document, not legally binding per se |
| Declaration of Helsinki | 1964 (rev. 2013) | Ongoing research abuses | Ethics committee review; distinction therapeutic/non-therapeutic | Current WMA standard for research |
| Belmont Report | 1979 | Tuskegee Syphilis Study | Three principles: respect for persons, beneficence, justice | Basis for US federal research regulations; conceptually foundational |
| Declaration of Geneva | 1948 (rev. 2017) | Post-war physician pledge | Modern medical oath replacing Hippocratic Oath | Current WMA standard; used at Indian graduations |
CLINICAL PEARL
The Nuremberg Code was written by judges, not doctors — a detail that reveals something important about medical ethics. The judges who wrote the Code were responding to doctors' own failure to protect their patients. This is why medical ethics cannot be left entirely to the medical profession to define and police without external scrutiny. The inclusion of independent ethics committees (later formalised in the Declaration of Helsinki and Indian regulations) reflects this same lesson: that medical expertise does not confer moral authority, and that the interests of research subjects require independent protection.
Contemporary Ethics: Declaration of Geneva and Indian Framework
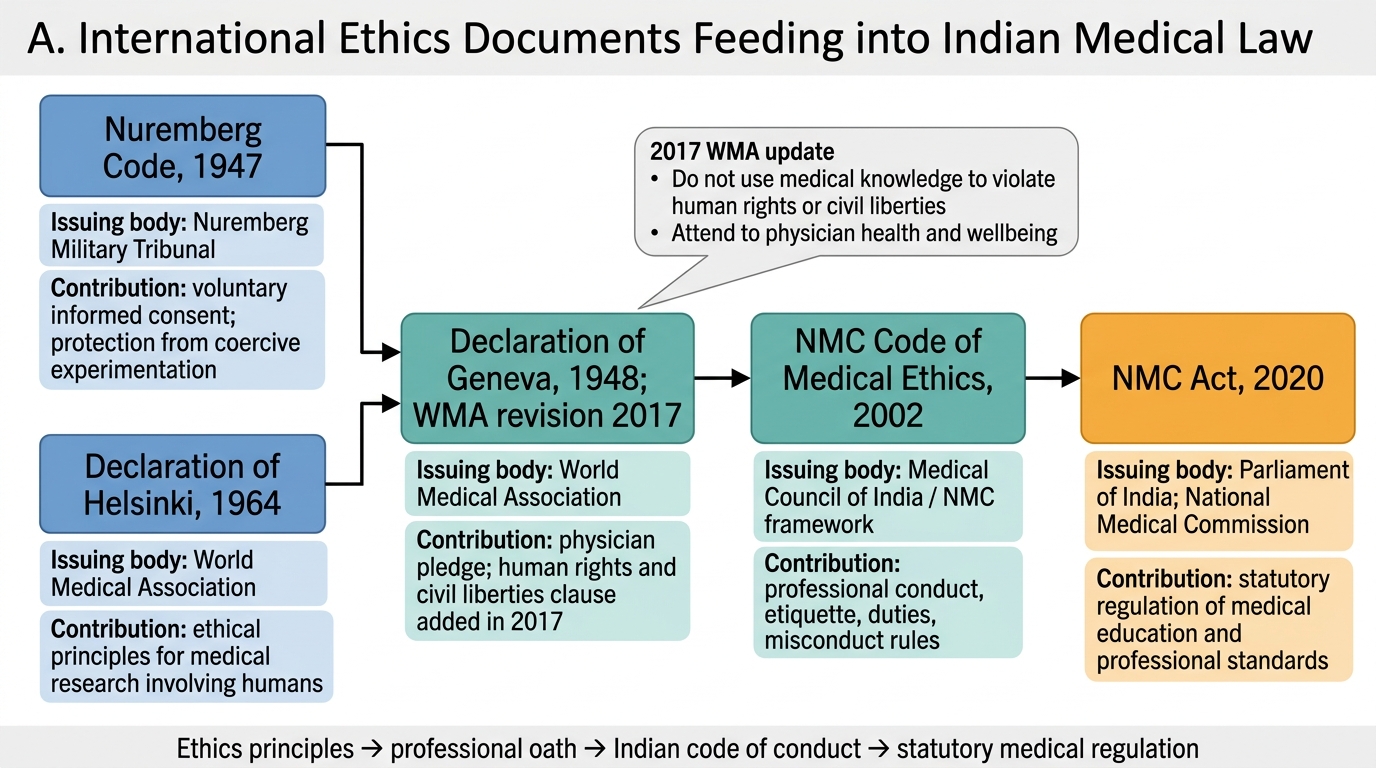
The contemporary ethical framework that Indian doctors operate within rests on two main pillars: the Declaration of Geneva as the international expression of medical professional commitment, and the NMC Code of Medical Ethics Regulations 2002 as the operative Indian regulatory standard.
The Declaration of Geneva was first adopted by the World Medical Association in 1948, explicitly as a response to the atrocities committed by Nazi physicians — a reaffirmation that medicine's purpose is to serve humanity. The most recent and current revision is the 2017 WMA Declaration of Geneva, which introduced two significant additions to the pledge:
1. 'I will attend to my own health, wellbeing and abilities in order to provide care of the highest standard' — recognising that physician health is not merely personal but a professional responsibility.
2. 'I will not use my medical knowledge to violate human rights and civil liberties, even under threat' — a direct response to ongoing violations of human rights by medical professionals in conflict and authoritarian contexts.
Indian medical graduates take a Declaration of Geneva-based oath at their graduation ceremonies. This is not merely a ritual — it is the formal public expression of the professional commitment that distinguishes a licensed practitioner from a trained technician.
The NMC Code of Medical Ethics Regulations 2002 governs the day-to-day conduct of registered medical practitioners in India. Originally enacted under the Medical Council of India (MCI), it is now operative under the NMC Act 2020 (which replaced the IMC Act 1956 and dissolved the MCI, replacing it with the NMC). The Code addresses:
- Duties to patients (care, consent, confidentiality, referral)
- Professional conduct (advertising, fees, relationships with colleagues)
- Prohibited practices (fee-splitting, canvassing, issuing false certificates)
- Disciplinary mechanisms (warning, penal erasure from the register)
The journey from Hippocrates to the NMC Code is not a simple progression — it is a series of responses to crises, abuses, and new moral challenges. Each document reflects the ethical lessons of its era. Understanding this history is what transforms a list of rules into a coherent professional identity.
Ethics Documents to Indian Medical Law
SELF-CHECK
Which of the following was added to the Declaration of Geneva in the 2017 WMA revision, making it distinct from all earlier versions?
A. The requirement for voluntary informed consent before any medical procedure
B. The prohibition against using medical knowledge to violate human rights and civil liberties
C. The duty of confidentiality towards patients
D. The commitment to practise medicine with conscience and dignity
Reveal Answer
Answer: B. The prohibition against using medical knowledge to violate human rights and civil liberties
The 2017 WMA revision of the Declaration of Geneva added two new clauses not present in earlier versions: (1) the human rights clause — 'I will not use my medical knowledge to violate human rights and civil liberties, even under threat'; and (2) the physician health clause — 'I will attend to my own health, wellbeing and abilities in order to provide care of the highest standard.' The duty of confidentiality and the commitment to practise with conscience were present in earlier versions.
KEY TAKEAWAYS
Medical ethics has ancient roots in the healing traditions of multiple cultures — the Hippocratic tradition of Greece, the Charaka and Sushruta traditions of India — all of which independently arrived at core principles: patient welfare first, confidentiality, and the prohibition on harm. The 20th century tested these principles severely: the Nazi physicians' crimes led to the Nuremberg Code (1947) — the first formal codification of voluntary informed consent; continued abuses led to the Declaration of Helsinki (1964) for research ethics; the Tuskegee Syphilis Study led to the Belmont Report (1979) and its three-principle framework. The Declaration of Geneva (1948, revised 2017) replaced the Hippocratic Oath as the modern medical pledge and is what Indian graduates take at graduation. The NMC Code of Medical Ethics 2002, operative under the NMC Act 2020, translates these principles into the regulatory framework governing Indian medical practice today. Understanding this history reveals that ethics is not an external constraint on medicine but its constitutive commitment.
REFLECT
Consider this question: The Nazi physicians who conducted experiments on prisoners were, in many cases, highly trained professionals who believed they were advancing scientific knowledge. They clearly had professional competence but lacked ethical integrity. What does this tell you about the relationship between technical expertise and moral responsibility in medicine? How does the institutional framework of ethics committees, peer review, and regulatory oversight compensate for the possibility that individual practitioners may not recognise or may rationalise ethical violations? What personal safeguards — beyond compliance with rules — would you want to cultivate to ensure that your own medical practice remains genuinely ethical rather than merely compliant?