Page 15 of 23
FM10.20 | Therapeutic Privilege, Misadventure & Professional Secrecy — SDL Guide (Part 2)
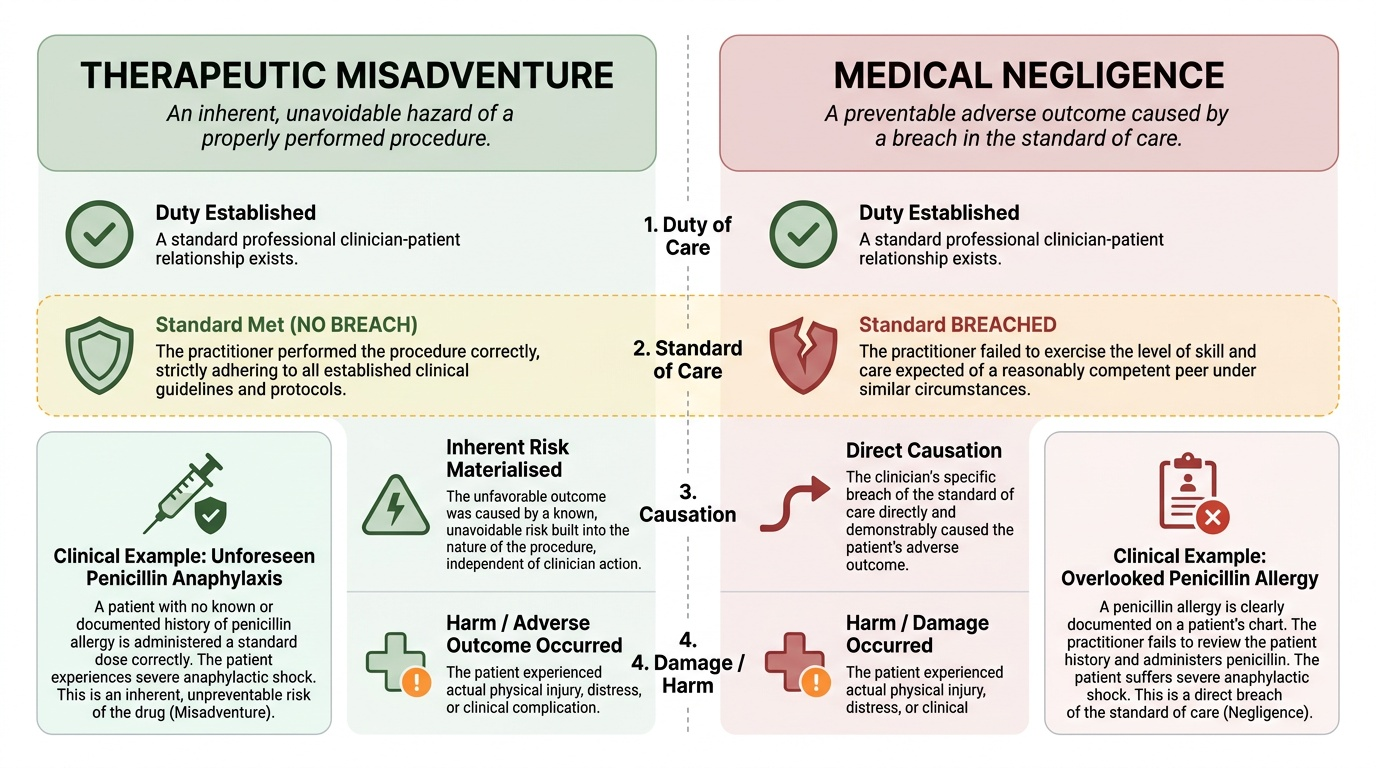
Therapeutic Misadventure: Definition and Distinction from Negligence
Therapeutic misadventure (also called therapeutic accident) is an unexpected, unintended adverse outcome from a medical treatment or procedure that was correctly performed — one where the adverse outcome results from an inherent hazard of the procedure or treatment, not from any error, omission, or breach of the standard of care by the practitioner. The key elements are:
- The procedure was performed correctly and in accordance with the applicable standard of care
- The adverse outcome was inherent to the procedure — a known risk that materialised, not a consequence of error
- There was no negligence on the part of the practitioner
Examples of therapeutic misadventure:
- Anaphylactic shock from a properly administered penicillin injection (where the allergy was not previously known)
- Post-operative haemorrhage in a patient with an undetected clotting disorder, despite technically correct surgery
- Cardiac arrest during anaesthesia in a patient with no pre-operative indication of cardiac vulnerability, despite proper anaesthetic technique
Therapeutic misadventure is NOT medical negligence. Medical negligence requires:
1. A duty of care (exists in the doctor-patient relationship)
2. A breach of the standard of care — the doctor failed to do what a reasonably skilled practitioner would have done (or did what a reasonably skilled practitioner would not have done)
3. Causation — the breach caused the adverse outcome
4. Damage — actual harm resulted
In therapeutic misadventure, element 2 is absent — there was no breach of the standard of care. The practitioner did everything correctly; the adverse outcome was an inherent risk that materialised despite correct practice.
Why the distinction matters legally:
- A family that files a complaint alleging negligence when the adverse outcome was a genuine misadventure will have difficulty sustaining the complaint if the documentation shows correct procedure and pre-operative consent included disclosure of the risk
- A practitioner who labels a genuine negligence case as 'misadventure' to avoid legal consequences is compounding a professional breach
- Proper contemporaneous documentation of the procedure, the risk disclosure in the consent process, and the post-event management is the practitioner's primary protection
Documentation requirements when an adverse outcome occurs:
- Contemporaneous note of the procedure performed and the steps taken
- Note of pre-operative/pre-procedure consent including disclosure of known risks
- Note of the adverse event — exact time, nature, immediate response, outcome
- If the outcome results in death, a death certificate citing the cause of death accurately
- In hospital deaths, notification to the appropriate authorities if required by hospital policy
Provided image
Professional Secrecy Revisited and Human Experimentation Ethics
Professional secrecy in the context of FM10.20 is reviewed from the perspective of specific clinical situations where the obligation is most complex (the full framework was covered in me5). The key principle remains: professional secrecy is a strong default obligation, with bounded, specific exceptions.
The exceptions most relevant to the complex situations in FM10.20 include:
- Medicolegal contexts: When a doctor conducts a medicolegal examination at the request of a court or police (in their professional capacity as a forensic examiner), the report is prepared for that official purpose — the duty of secrecy to the individual does not prevent the forensic examiner from submitting the report to the requesting authority
- Research: Patient information may be used in research only with adequate consent or under anonymisation that removes patient identifiability; this is governed by the ICMR guidelines for Biomedical Research on Human Participants
- HIV-specific: The HIV and AIDS (Prevention and Control) Act 2017 creates specific provisions governing disclosure of HIV status, including protections for the patient and limited exceptions for healthcare workers at risk
Human experimentation ethics refers to the ethical framework governing research involving human subjects. The foundational documents — Nuremberg Code (1947), Declaration of Helsinki (1964, revised 2013) — were discussed in me1. The operative Indian framework for human experimentation is:
- ICMR National Ethical Guidelines for Biomedical and Health Research Involving Human Participants (2017): The primary Indian regulatory framework for research ethics; requires institutional ethics committee (IEC) review for all human research
- Schedule Y of the Drugs and Cosmetics Act 1940 (and New Drugs and Clinical Trial Rules 2019): Governs clinical trials of drugs in India; requires registration with CDSCO, ethics committee approval, and monitoring
Core principles for human experimentation (applicable to every research context):
1. Voluntary informed consent — the absolute requirement; consent must be free of coercion, given after adequate disclosure, by a competent person
2. Scientific validity — the experiment must have scientific merit; no ethical framework permits worthless experiments on human subjects
3. Favourable risk-benefit ratio — potential benefits must outweigh risks; if the risk-benefit assessment changes during the study, the study must be stopped
4. Independent ethics committee review — an Institutional Ethics Committee (IEC) must review and approve all human research protocols
5. Voluntary withdrawal — subjects must be able to withdraw at any time without penalty
6. Special protection for vulnerable populations — children, prisoners, pregnant women, persons with mental illness — additional safeguards required
SELF-CHECK
A 35-year-old man presents with sudden onset complete paralysis of his right arm following a domestic argument. On examination, the paralysis is inconsistent with any known neurological pattern; power returns completely when the examiner asks him to resist opposing pressure in a different test position. There is no organic neurological disease on investigation. This presentation is MOST consistent with:
A. Malingering — the patient is consciously exaggerating symptoms for compensation
B. Factitious disorder — the patient wants to be in the sick role
C. Conversion disorder — the patient has unconscious, functional neurological symptoms
D. Therapeutic misadventure — an adverse outcome of prior medical treatment
Reveal Answer
Answer: C. Conversion disorder — the patient has unconscious, functional neurological symptoms
Conversion disorder (Functional Neurological Symptom Disorder) presents with genuine neurological symptoms that cannot be explained by organic neurological disease. The symptoms are unconscious — the patient is not deliberately fabricating. Characteristic findings include inconsistency with known neurological patterns, and tests that reveal preserved function under different conditions (like the power return on different positioning) — these reflect neurological inconsistency, not voluntary deception. Malingering requires conscious fabrication with external gain motivation; factitious disorder requires conscious motivation for the sick role. Neither the scenario description nor the typical presentation supports those diagnoses here.
CLINICAL PEARL
The words you use in a medicolegal report about adverse outcomes or symptom inconsistency have legal consequences. 'The patient died due to therapeutic misadventure' is a specific, legally meaningful statement — make it only if you are certain all elements are met (correct procedure, inherent risk, no negligence). Similarly, 'the claimant appears to be malingering' is an accusation with potential defamation implications if made without adequate evidence. The preferred forensic language for symptom inconsistency is: 'The objective clinical findings are inconsistent with the reported degree of disability' — this is factually accurate and does not attribute intent. Reserve the label 'malingering' for contexts where conscious fabrication and external gain are clearly established.
Applied Practice: Documenting and Reasoning Through Each Scenario
The five concepts in FM10.20 require not just conceptual clarity but practical documentation and reasoning skills. The following approach applies across all five scenarios:
Applying the concepts in practice:
Therapeutic privilege — in clinical consultation:
- Default to disclosure; document the consent conversation
- If genuinely concerned about psychological decompensation, consult a psychiatric colleague
- Document the reasons for any deferral — make explicit that it is a time-limited deferral, not permanent withholding
- Never defer because the family requests it — the duty runs to the patient
Malingering — in medicolegal assessment:
- Conduct a thorough, objective physical and mental status examination
- Document objective findings precisely; note every inconsistency explicitly and neutrally
- Apply validated clinical tests (Waddell signs, Hoover sign, etc.) and document the results
- In the report: state the clinical findings, note the inconsistencies, and express opinion only if adequately supported — 'the findings are inconsistent with genuine [condition]' rather than 'the claimant is malingering'
Therapeutic misadventure — following an adverse outcome:
- Ensure the death certificate or adverse outcome report accurately states the cause: 'cardiac arrest following general anaesthesia, therapeutic misadventure' — if that is accurate
- Do NOT label as misadventure if there is any doubt about procedural compliance — seek peer review
- The consent documentation showing risk disclosure is the primary protection
Professional secrecy — before any disclosure:
- Apply the exceptions checklist (court order? notifiable disease? immediate public safety? patient consent?) before any disclosure
- If no exception clearly applies, do not disclose
- Document the rationale for any disclosure decision
Human experimentation — at the research planning stage:
- No human research begins without IEC approval and valid informed consent protocols
- Consent must be obtained by a member of the research team who is not in a position of authority over the participant
- All adverse events during a trial must be reported to the IEC and CDSCO (for drug trials)
SELF-CHECK
A patient undergoes a routine cholecystectomy performed by an experienced surgeon following all standard protocols. Post-operatively, the patient develops an acute myocardial infarction and dies. Pre-operative cardiac evaluation was normal. This outcome is BEST classified as:
A. Medical negligence — the surgeon should have performed a more thorough cardiac workup
B. Therapeutic misadventure — an unexpected adverse outcome from a correctly performed procedure
C. Infamous conduct — the outcome represents a breach of the duty of care
D. An adverse drug reaction — the anaesthetic caused the myocardial infarction
Reveal Answer
Answer: B. Therapeutic misadventure — an unexpected adverse outcome from a correctly performed procedure
This is therapeutic misadventure — an unexpected, adverse outcome from a procedure that was correctly performed. The surgery was conducted by an experienced surgeon following all standard protocols, and pre-operative cardiac evaluation was normal (no negligence in pre-operative assessment). The MI was an inherent risk of surgery/anaesthesia that materialised despite correct practice. Negligence requires a breach of the standard of care — there is none stated here. Infamous conduct refers to a professional misconduct category, not an outcome classification.