Page 5 of 20
FM5.2-3 | Medico-legal Classification of Injuries (BNS) — SDL Guide (Part 2)
Ante-mortem vs Post-mortem Injuries: Vital Reaction
One of the most critical questions in a homicide investigation is whether injuries on a body were inflicted before death (ante-mortem), around the time of death (perimortem), or after death (post-mortem). This question arises because perpetrators sometimes inflict injuries on a corpse to stage a crime scene, or because additional trauma occurs post-mortem (vehicular transport, animal activity). The forensic distinction relies on the presence or absence of vital reaction — the biological response of living tissue to injury.
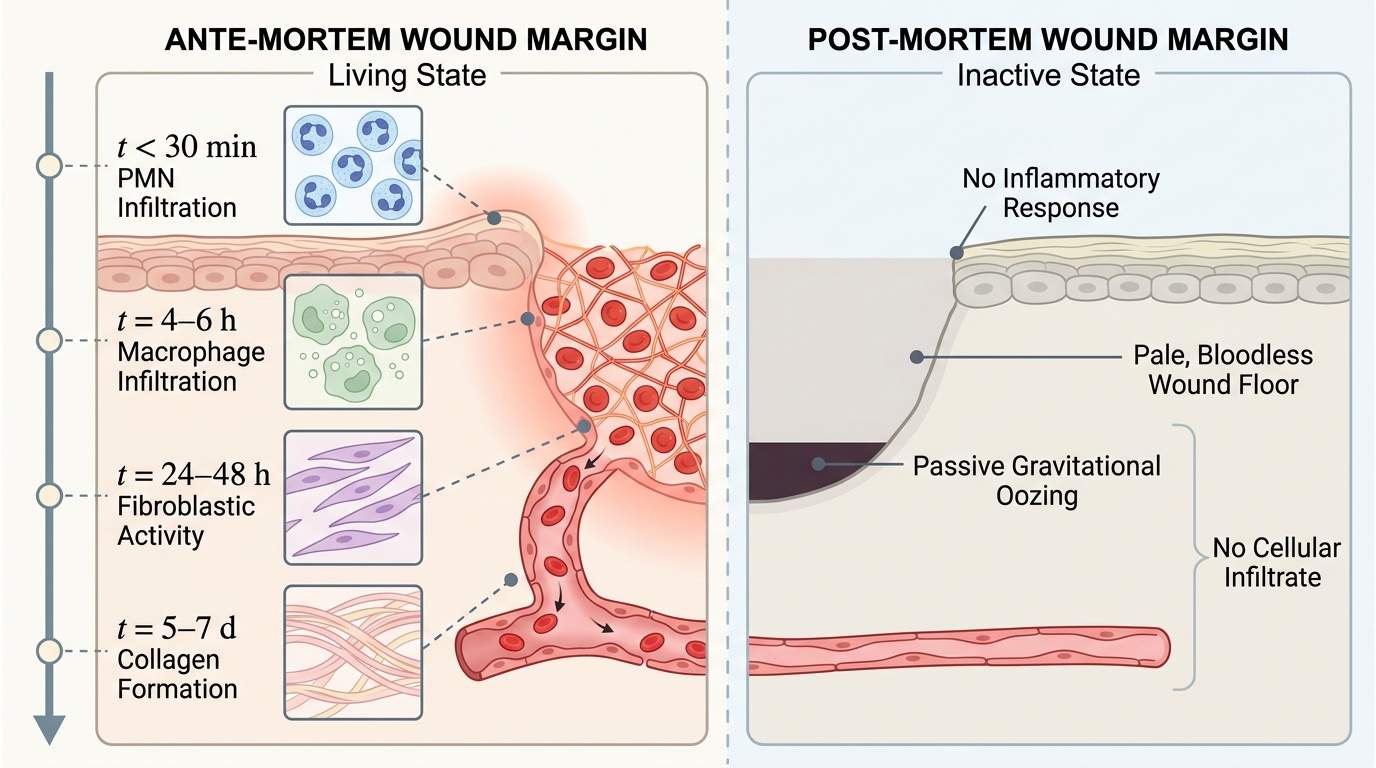
Vital reaction encompasses both macroscopic and histological features. Macroscopically, ante-mortem wounds show active bleeding from intact circulation, red-margin redness and swelling (the inflammatory response), and wound edges that show tissue reaction. Post-mortem wounds, by contrast, show no active bleeding (only gravity-dependent oozing from disrupted vessels), no surrounding inflammation, and a pale, bloodless wound floor. The colour difference between ante-mortem haemorrhage (bright red, clotted) and post-mortem gravitational staining (passive dark discolouration) is visible to the naked eye.
Histologically, the time sequence of vital reaction is well-established and medico-legally important. Within 30 minutes of an ante-mortem injury, polymorphonuclear neutrophils (PMNs) begin infiltrating the wound margins. By 4–6 hours, macrophage infiltration is visible. By 24–48 hours, macrophage and fibroblast activity is prominent. Collagen formation begins around 5–7 days. These histological milestones allow the forensic pathologist to estimate — within a range — when an injury was inflicted relative to death. Post-mortem wounds show none of these cellular responses because the circulation has ceased.
Provided image
A special category is the perimortem injury — inflicted at the time of death when the physiological response is transitional. Perimortem fractures (e.g. in hanging) show features intermediate between ante-mortem and post-mortem, which is an area requiring careful interpretation. The clinical rule is that histological examination is mandatory for ante-mortem vs post-mortem determination whenever the macroscopic findings are equivocal.
SELF-CHECK
At post-mortem examination, a wound is found on the deceased's right thigh. Histological examination shows no PMN infiltration, no macrophage activity, and the wound margins are pale with no inflammatory reaction. What does this indicate?
A. The wound was inflicted approximately 1-2 hours before death
B. The wound was inflicted more than 24 hours before death
C. The wound was inflicted post-mortem — no vital reaction is present
D. The wound cannot be timed because histology is inconclusive
Reveal Answer
Answer: C. The wound was inflicted post-mortem — no vital reaction is present
Complete absence of PMN infiltration, macrophage activity, and inflammatory reaction at the wound margins indicates a post-mortem wound. Ante-mortem wounds show PMN infiltration within 30 minutes of injury. The pale, bloodless wound floor with no cellular response confirms the wound was inflicted after circulatory function had ceased. This finding may indicate a staged crime scene or post-mortem trauma.
Medico-legal Opinion: Linking Findings to Statutory Categories
The medico-legal opinion is the concluding section of the MLC and represents the physician's professional judgement connecting factual clinical findings to statutory legal categories. It must be carefully phrased: stating established facts clearly, drawing inferences that the facts support, and refraining from stating legal conclusions that are for the court to decide.
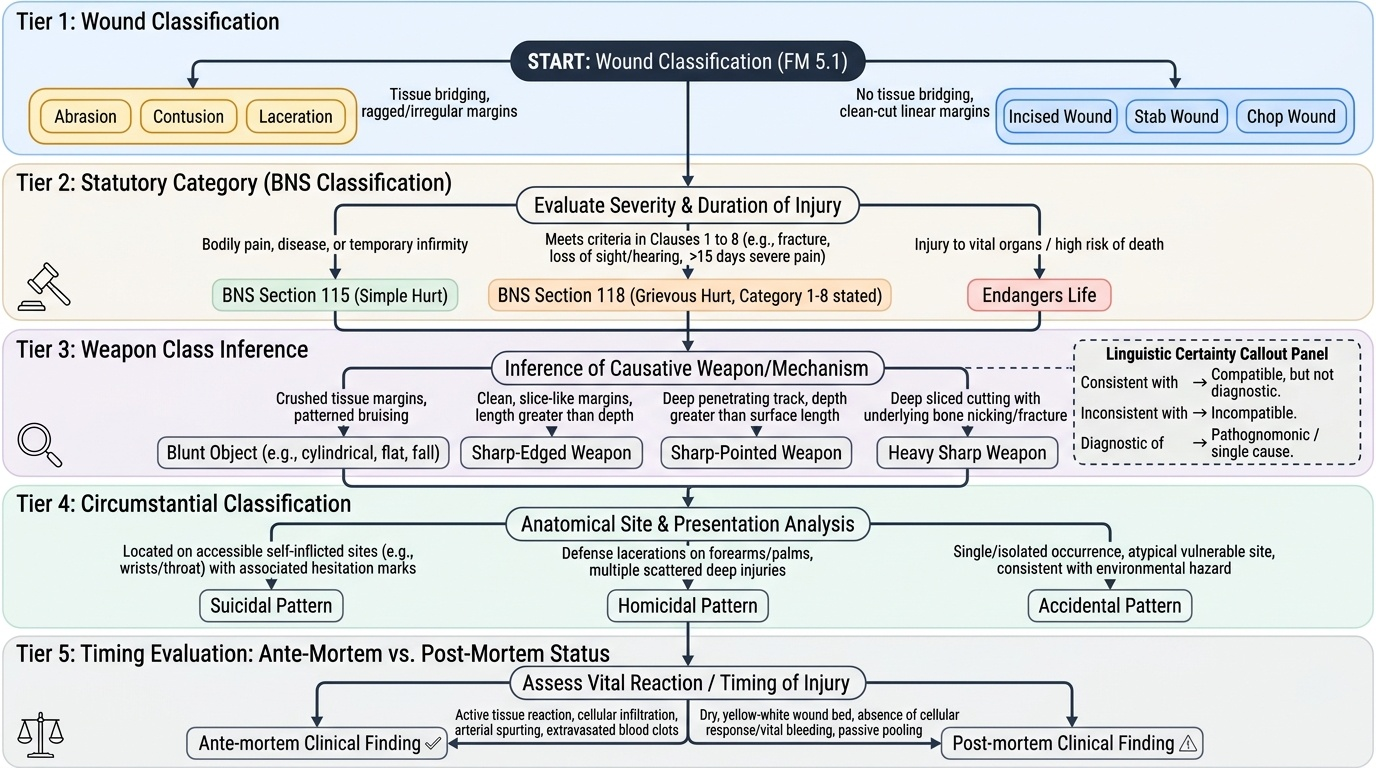
A well-structured medico-legal opinion addresses four questions in sequence. First: What type of injury is this? (applying FM5.1 wound classification — abrasion, contusion, laceration, incised wound, stab wound, chop wound). Second: What is its statutory category? (applying BNS Section 115 for hurt, BNS Section 118 for grievous hurt with the specific sub-category stated, or noting that it endangers life). Third: What weapon or mechanism is consistent with this injury? (e.g. 'consistent with a sharp-edged weapon', 'consistent with a blunt cylindrical object', 'consistent with fall on a hard surface'). Fourth: Is the injury ante-mortem or post-mortem? (if this is relevant to the case).
The language of medico-legal opinion follows established conventions. 'Consistent with' means the finding is compatible with the stated mechanism but not exclusively diagnostic of it. 'Inconsistent with' means the finding is incompatible with the stated mechanism. 'Diagnostic of' or 'pathognomonic of' is reserved for findings with no alternative explanation. These gradations of certainty are important because a doctor who overstates certainty ('this wound was definitely caused by a knife') when the finding only supports 'consistent with a sharp-edged weapon' is open to legitimate cross-examination.
For cases involving accidental, suicidal, and homicidal classification, the opinion should state the convergent features: for example, 'The pattern of injuries — multiple wounds on the back and posterior trunk, bilateral defence wounds on the forearms, and absence of hesitation marks — is consistent with a homicidal assault and inconsistent with self-infliction.' This formal statement, grounded in clinical findings, gives the police and prosecution a solid medico-legal foundation for their case.
Provided image
SELF-CHECK
A 28-year-old man has a wound described in the MLC as: 'right forearm, incised wound, 5 cm × 0.3 cm, clean margins, no tissue bridges, depth 0.4 cm, vital reaction present, along with 4 shallow parallel tentative marks at the margin.' What is the MOST appropriate medico-legal opinion?
A. Grievous hurt (BNS S118 Cat. 7 — fracture); consistent with homicidal assault
B. Simple hurt (BNS S115); wound features consistent with self-infliction (accessible site, hesitation marks, no defence wounds described)
C. Grievous hurt (BNS S118 Cat. 8 — endangers life); consistent with homicidal assault
D. Simple hurt (BNS S115); wound features consistent with accidental injury
Reveal Answer
Answer: B. Simple hurt (BNS S115); wound features consistent with self-infliction (accessible site, hesitation marks, no defence wounds described)
The wound is 5 cm × 0.3 cm with 0.4 cm depth — an incised wound that does not fracture bone, does not endanger life, and does not meet the 20-day disability criterion; it is therefore simple hurt under BNS S115. The clinical pattern — forearm location (accessible), incised wound with hesitation marks, no other wounds mentioned — is consistent with self-infliction. The medico-legal opinion should note these features and state 'consistent with self-infliction' while documenting all findings for the court's determination.