Page 13 of 20
FM14.{1,9} | Medico-legal Examination & Reporting of Injuries — SDL Guide
Learning Objectives
- Describe the procedure for conducting a medico-legal examination of an injured person, including consent, systematic injury survey, and documentation
- Identify and prepare medico-legal inferences from the seven FM14.9 specimen types: contusion, abrasion, laceration, firearm wounds, burns, head injury, and fracture of bone
- Describe the structure and required components of a medico-legal certificate (MLC) for an injured person
- Integrate examination findings, wound classification (FM5.1), and BNS statutory categories (FM5.2) into a complete medico-legal opinion
INSTRUCTIONS
The medico-legal certificate for an injured person is a document that every doctor working in a casualty or emergency setting will prepare. Unlike a standard clinical note, the MLC has formal legal standing — it is admissible in court as expert evidence, it can determine the charges filed against a perpetrator, and deficiencies in it can derail a prosecution. This module provides the procedural and reporting framework for medico-legal examination of injured persons across the range of injury types specified in FM14.9, integrating the wound classification knowledge from earlier modules into the structured clinical skill of examination and reporting.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old woman is brought to the casualty at 2 AM by the police. She is conscious, distressed, and has multiple injuries. The constable asks you to 'quickly write the MLC so we can go arrest the suspect.' On examination, you find: a 2 cm laceration over the right eyebrow, bruising on both forearms, abrasions on the left cheek, and tenderness over the right rib cage. You do not have the patient's full history and the constable is pressuring you to complete the MLC immediately. How do you handle this situation, what is the correct examination sequence, and what must your MLC contain to be legally useful and professionally defensible?
WHY THIS MATTERS
The medico-legal certificate is simultaneously a medical record and a piece of legal evidence. As a doctor working in any emergency or primary care setting in India, you will be called upon to prepare MLCs for assault victims, road traffic accident casualties, and persons in police custody. The quality of your MLC — its completeness, precision, and objectivity — directly determines its legal utility. An MLC that describes wounds vaguely ('multiple injuries present'), omits findings, or uses non-standard terminology may not support a conviction even when the clinical evidence is compelling. Conversely, a well-prepared MLC that precisely documents wound type, BNS category, and supporting clinical findings provides the prosecution with a solid medical foundation. Beyond criminal proceedings, MLCs are used in civil cases (insurance claims, accident compensation), employment disputes, and custody proceedings. The forensic examination skill is therefore not a niche subspecialty — it is a core clinical competency for every practising physician.
RECALL
From the preceding modules in this cluster, bring together the following knowledge for application: wound type classification (FM5.1) — abrasion (epidermis only), contusion (intact skin, subcutaneous haemorrhage), laceration (irregular edges, tissue bridges), incised wound (clean margins, length > depth, no tissue bridges), stab wound (depth > length); BNS injury categories (FM5.2) — simple hurt (S115), grievous hurt (S118 — 8 categories, especially Category 7 for fractures and Category 8 for 20+ days disability or endangers life); vital reaction for ante-mortem vs post-mortem determination (FM5.3 — PMN within 30 minutes, macrophages 24-48 hours). You will apply all of these in this module as an integrated clinical skill.
The MLC as Expert Evidence: Professional and Legal Stakes
Every MLC prepared by a registered medical practitioner carries the weight of expert evidence when submitted in court. The legal framework under the Bharatiya Sakshya Adhiniyam 2023 (BSA — the new evidence law replacing the Indian Evidence Act 1872) provides for expert opinion, including medical expert opinion, as admissible evidence. The doctor's MLC, properly prepared and signed, is produced before the court and the doctor may be called as a witness to explain and defend its contents under cross-examination.
The professional and ethical stakes are significant. Under-documentation — failing to record injuries, recording wounds vaguely, or omitting relevant findings — can result in evidence that fails to support a legitimate prosecution. In assault and domestic violence cases, the MLC is often the most objective evidence available, and its inadequacy can lead to acquittals that are not justified by the actual clinical findings. Over-documentation or fabricated findings — recording injuries not present, amplifying the severity, or accepting coercion from police to add findings — constitutes falsification of a medical record and making a false document, offences under the BNS with criminal consequences for the doctor.
The examining physician must therefore approach the MLC with complete independence from the investigating authority. The police may request the examination, but the content of the MLC is determined solely by the doctor's clinical findings. In the scenario above, the constable's request to 'quickly write the MLC so we can go arrest the suspect' is an inappropriate attempt to expedite or influence the process. The doctor is entitled — and obligated — to take the time required for a thorough examination. Rushing compromises the quality of evidence and the doctor's professional accountability.
Contemporaneous documentation is also legally required: the MLC must be completed at the time of examination, with the exact date and time recorded, and signed by the examining physician. An MLC completed retrospectively — hours or days after the examination — is vulnerable to challenge as to its accuracy and admissibility.
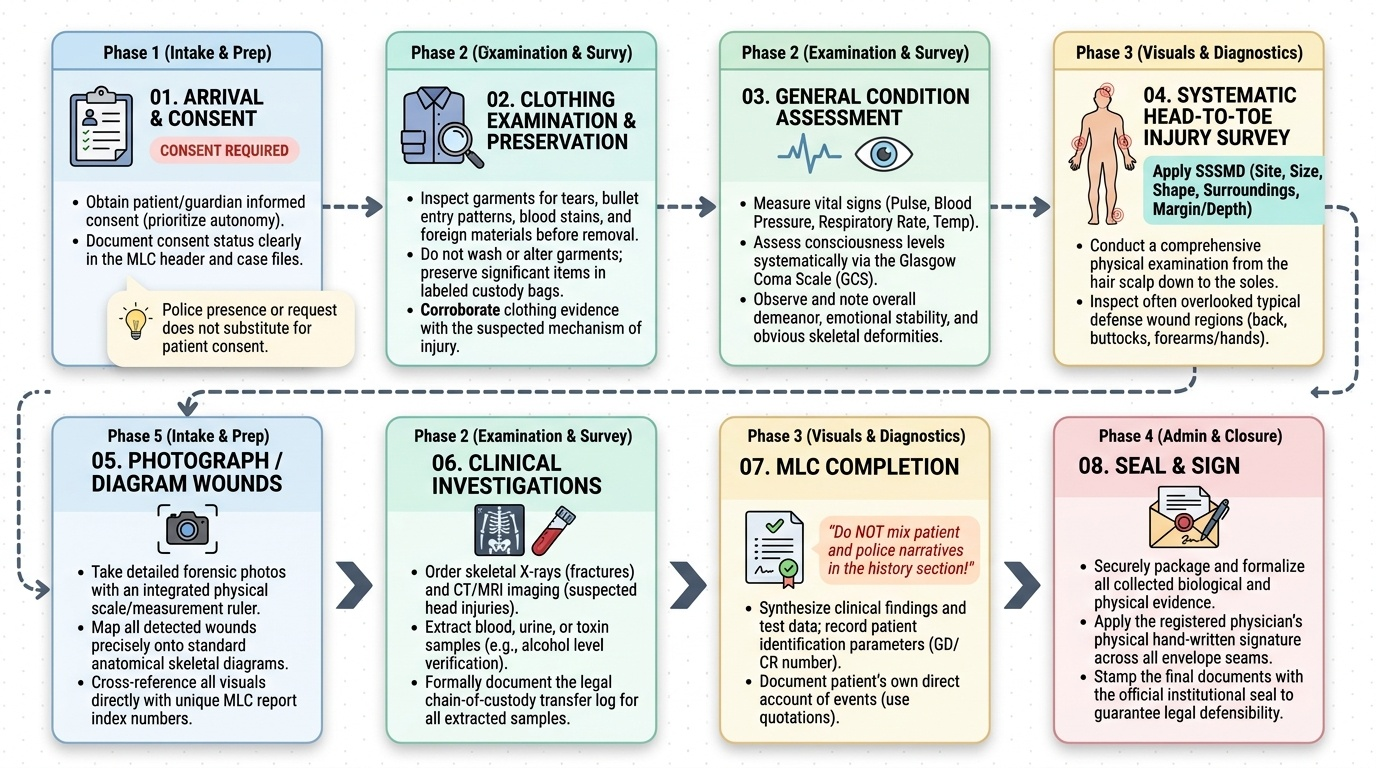
The Medico-legal Examination: Procedure and Protocol
The medico-legal examination of an injured person follows a structured procedure designed to ensure completeness, objectivity, and legal defensibility. The sequence of steps applies regardless of the etiology of injury — assault, road traffic accident, industrial accident, or firearms.
Step 1 — Consent: before any examination, obtain informed consent from the patient (if adult and conscious) or from the guardian/next of kin (if a minor, unconscious, or mentally incapacitated). Police presence and police request do not substitute for patient consent. Document the consent in the MLC and in the case notes.
Step 2 — Identification: record the patient's full name, age, sex, address, occupation, and the referring authority (police station, officer's name, GD/CR number). This information is required for the MLC header and links the document to the specific police case.
Step 3 — History: record the alleged history as narrated by the police and/or the patient separately. Do NOT mix the two versions. The patient's own account of what happened, who inflicted the injuries, and when, is medico-legally relevant and may later be used to corroborate or challenge the police version. Use direct quotation where possible: Patient states — 'I was beaten by my husband with a stick at approximately 10 PM.'
Step 4 — General examination: record consciousness level (GCS if indicated), vital signs (pulse, blood pressure, respiratory rate, temperature), general appearance (clothing, demeanour, apparent emotional state), and any obvious deformity.
Step 5 — Systematic injury survey (head to toe): examine systematically from the scalp to the soles. Note the site, size, shape, surroundings, and margin/depth characteristics of every injury (SSSMD mnemonic). Do not stop after finding the first injury. Examine the back, buttocks, and the dorsum of hands and forearms (often overlooked but where defence wounds and beating evidence appear).
Step 6 — Clothing examination: clothing should be examined for tears, blood staining, and foreign material before it is removed. Clothing can provide corroborating evidence of the mechanism of injury. Note the condition and preserve significant items.
Step 7 — Ancillary investigations: order X-rays for suspected fractures, CT/MRI for head injuries, and blood/urine alcohol level where intoxication is relevant. These investigations must be referenced in the MLC when their results contribute to the opinion.
Step 8 — MLC completion, signing, and sealing: the MLC is completed in the standard format (see below), signed, dated, and timed. One copy is retained in the hospital records; one is handed to the police against a receipt.
Provided image
SELF-CHECK
A patient is brought for medico-legal examination by the police after an alleged assault. The patient is conscious but refuses to give consent for the examination, saying 'I don't want to get involved.' What is the MOST appropriate action?
A. Proceed with the examination because the police have authorised it
B. Proceed with a limited examination of visible injuries only
C. Respect the patient's refusal — document the refusal in the case record and inform the police that the examination cannot proceed without consent
D. Call the patient's family to provide consent on their behalf
Reveal Answer
Answer: C. Respect the patient's refusal — document the refusal in the case record and inform the police that the examination cannot proceed without consent
A competent adult's refusal of consent must be respected in all circumstances, including medico-legal examinations. The police authorisation for examination does not override patient autonomy. The doctor should document the refusal clearly in the case record and inform the police verbally. The patient's refusal is itself a medico-legal fact that the police must note. Family consent is relevant only for minors or incapacitated adults — it does not apply to a conscious, competent adult who refuses.
Identifying and Describing Medico-legal Specimens (FM14.9)
FM14.9 requires the ability to identify and prepare medico-legal inferences from a set of specimens or clinical findings representing the most important injury types encountered in Indian forensic practice. The following seven categories, which include nine distinct examination points, cover the full range specified in the competency.
Contusion: a blunt force injury with intact overlying skin and visible haemorrhage into subcutaneous/deeper tissue. Medico-legal inference: indicates blunt force applied to the area; patterned contusions reproduce the shape of the causative object. Key examination point: examine in good light — contusions may not be visible immediately after injury and may deepen over 24-48 hours. Photographing at intervals is useful.
Abrasion: epidermis-only injury with surface disruption, no gap, no deep haemorrhage. Medico-legal inference: direction of force can sometimes be inferred (dislodged epithelial cells point in the direction of the scraping force); surface pattern may identify the causative surface (road rash = asphalt pattern). Post-mortem abrasions are dry, parchment-like, and yellow-brown.
Laceration: blunt force wound with irregular torn edges and tissue bridges. Medico-legal inference: blunt force was applied; the presence of tissue bridges distinguishes it from incised wounds and indicates the weapon was not sharp-edged. Wound floor contamination may identify the causative surface.
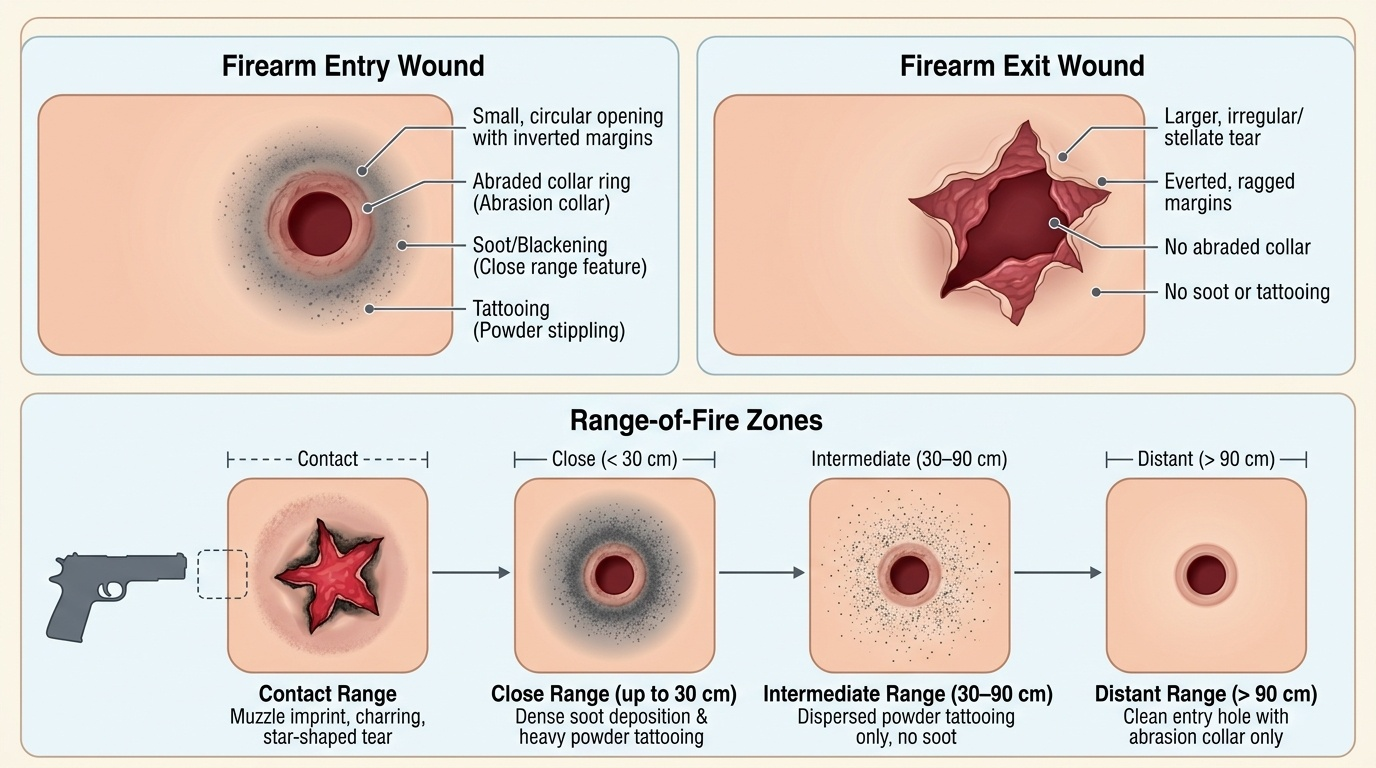
Firearm wounds: require differentiation of entry from exit wounds. Entry wound features: relatively small, inverted/inturned margins, abraded collar (Fisch collar — abrasion caused by the bullet spinning and driving skin inward), and in contact/close range shots — blackening (soot deposition), singeing (burning of skin/hair), and tattooing (unburnt powder grains embedded in skin). Exit wound features: typically larger, everted/irregular margins, no abraded collar, no blackening or tattooing. The range of firing can be estimated from the presence and extent of blackening and tattooing:
- Contact: blackening, singeing, cruciate laceration from gas blast, soot in wound track
- Close range (up to ~30 cm): blackening and some tattooing
- Intermediate range (30–90 cm): tattooing, no blackening
- Distant: no secondary features, abraded collar only
Provided image
Burns: document using the Rule of Nines for body surface area (BSA) estimation (head = 9%, each arm = 9%, chest/abdomen anterior = 18%, back = 18%, each thigh+leg = 18%, perineum = 1%). Depth: superficial epidermal (erythema only, no blistering), superficial partial-thickness (painful blistering), deep partial-thickness (reduced sensation, haemorrhagic blistering), full-thickness (insensate, waxy/leathery, no blistering). Medico-legal inference: pattern of burns (immersion burns — sharp demarcation at the waterline; contact burns — shape of object; chemical burns — trail-drip pattern) assists in determining mechanism and whether self-inflicted, accidental, or homicidal.
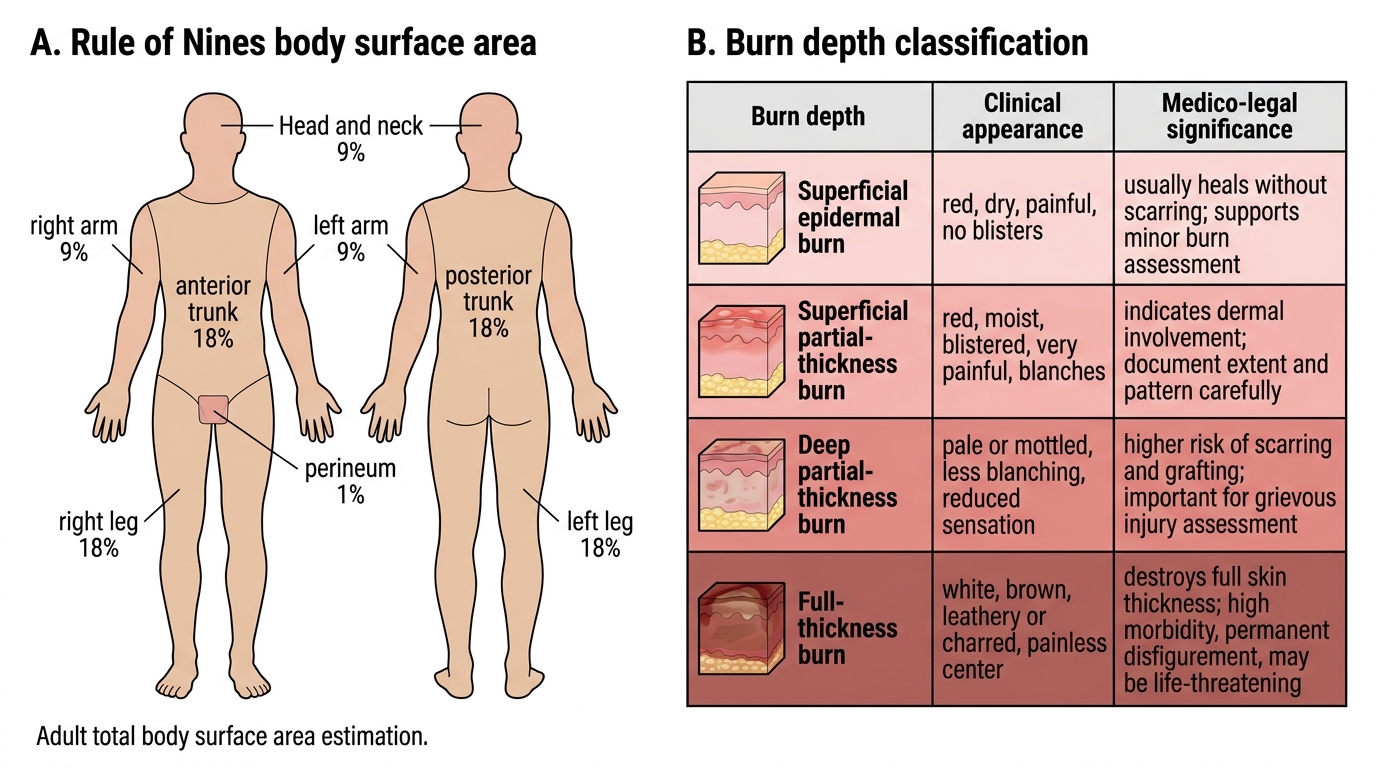
Rule of Nines and Burn Depth Classification
Head injury: encompasses scalp wounds, skull fractures, and intracranial injury. Key medico-legal pattern: a lucid interval — an initial period of consciousness followed by deterioration — is characteristic of extradural haemorrhage from rupture of the middle meningeal artery (typically associated with a temporal bone fracture). Immediate and persistent unconsciousness suggests diffuse axonal injury or severe cerebral contusion. Contre-coup injury (contusion on the side opposite the impact) is produced by deceleration of the brain against the opposite inner skull surface.
Fracture of bone: note site, fracture type (transverse, oblique, spiral, comminuted), alignment, and healing stage (using the radiological timeline from FM5.4 — periosteal new bone at ~2-3 weeks, hard callus at ~6-12 weeks). Spiral fractures of long bones in children are a classic pattern in non-accidental injury (child abuse) from rotational force. Multiple fractures at different healing stages on skeletal survey also suggest non-accidental injury.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
FM14.9 Specimen Identification and Forensic Inference
CLINICAL PEARL
The lucid interval is one of the highest-yield clinical-forensic correlations in head injury. A patient who is conscious at the scene, transported to hospital, but then deteriorates to unconsciousness — especially with ipsilateral pupil dilation — has an extradural haemorrhage from middle meningeal artery rupture until proven otherwise. For the forensic physician, the lucid interval means that even if the victim dies, they were not immediately incapacitated by the blow. This has implications for whether the victim could have moved, called for help, or provided information before losing consciousness — all of which may be relevant to the criminal investigation timeline.