Page 7 of 20
FM5.4-5 | Wound Healing, Examination & Certification — SDL Guide
Learning Objectives
- Describe the phases of wound healing with their cellular mechanisms and medico-legal dating landmarks
- Describe the stages of bone fracture healing and explain their radiological appearances relevant to injury timing
- Enumerate and explain the factors that influence the infliction and healing of wounds
- Classify wound as a cause of death into primary and secondary causes and provide clinical examples of each
- Formulate a medico-legal opinion on wound healing duration and causation of death for medico-legal certification
INSTRUCTIONS
A wound does not end when the patient leaves the emergency department. For the forensic physician, the trajectory of a wound — whether it heals normally, becomes infected, leads to complications, or results in death — is as medico-legally significant as the original injury. The time taken for healing allows courts to retrospectively estimate when an injury was inflicted. Complications that lead to death create chains of causation that must be attributed. Factors that hindered or accelerated healing can affect determinations of negligence or contributory cause. This module examines wound and fracture healing with the specific lens of medico-legal application — not just what heals and how, but what the healing process reveals about when, why, and how an injury led to its outcome.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 60-year-old farmer sustains a deep laceration on his right foot from a rusty plough 12 days before admission. He initially treated the wound with local herbs and did not seek medical attention. He is admitted with trismus, opisthotonus, and generalised convulsions. Despite ICU care, he dies on day 4 of admission. The family alleges medical negligence because the district hospital they first visited 8 days ago had 'sent him away with painkillers without proper treatment.' You are asked to prepare a medico-legal opinion: what caused this man's death, was the wound the proximate cause, and does the 8-day gap in treatment constitute contributory negligence?
WHY THIS MATTERS
Understanding wound healing is not merely an academic exercise in pathology — it is a medico-legal investigative tool. In forensic practice, the state of a wound at post-mortem examination allows the forensic pathologist to estimate when the injury was inflicted, which can corroborate or contradict a timeline presented in court. The complications of wound healing — infection, sepsis, tetanus, gangrene — create chains of causation that courts must adjudicate, and the forensic physician's opinion on 'whether this complication was caused by the original wound' is central to determining criminal liability. When a patient dies weeks after a wound, the question is not just what they died of but whether the wound was the cause of death in law — a question that the medico-legal certificate must address with precision.
RECALL
From your physiology and pathology studies, recall the cellular events in the inflammatory response: the vascular phase (vasodilatation, increased permeability), the cellular phase (neutrophil margination and emigration within hours), and the chronic phase (macrophage dominance, fibroblast activation). These are the same events that constitute the vital reaction at a wound site. Recall also from biochemistry that collagen synthesis requires vitamin C (hydroxylation of proline and lysine) and zinc (metalloprotease activity), which explains why nutritional deficiencies impair wound healing. From anatomy, recall that bone is a living organ with periosteum containing osteoprogenitor cells, which form the cellular basis of fracture repair.
When a Wound Becomes a Death: Healing Failure and Medico-legal Consequence
The medico-legal significance of wound healing extends far beyond simple recovery. In the case above, a wound that should have been manageable — a laceration that with proper wound care and tetanus prophylaxis would have healed uneventfully — has become a fatal case of tetanus, and possibly a case of medical negligence. Understanding what should have happened, and when, is the foundation of the medico-legal analysis.
In forensic medicine, wound healing timelines serve three distinct purposes. First, they are used retrospectively to estimate when an injury was inflicted based on the degree of healing observed at examination or autopsy — an early haematoma suggests a recent injury, organised granulation tissue suggests days, scarring suggests weeks. Second, they establish the chain of causation between an initial wound and a subsequent complication: if a patient dies of gas gangrene seven days after a penetrating injury, the question of whether the wound caused the death depends on the established causal link between the injury, the anaerobic environment created by devitalised tissue, and the proliferation of Clostridium perfringens. Third, they inform opinions on contributory negligence: if a factor that is known to impair healing — inadequate wound debridement, delayed treatment, failure to provide tetanus prophylaxis — is identified, the physician's failure to act can be cited as a contributory cause of the outcome.
This makes the forensic physician's knowledge of wound healing both a diagnostic skill and a legal instrument. The opinion rendered in the medico-legal certificate about wound healing trajectory and causation will be scrutinised by lawyers, judges, and medical experts in court.
Wound Healing: Phases, Mechanisms, and Medico-legal Timelines
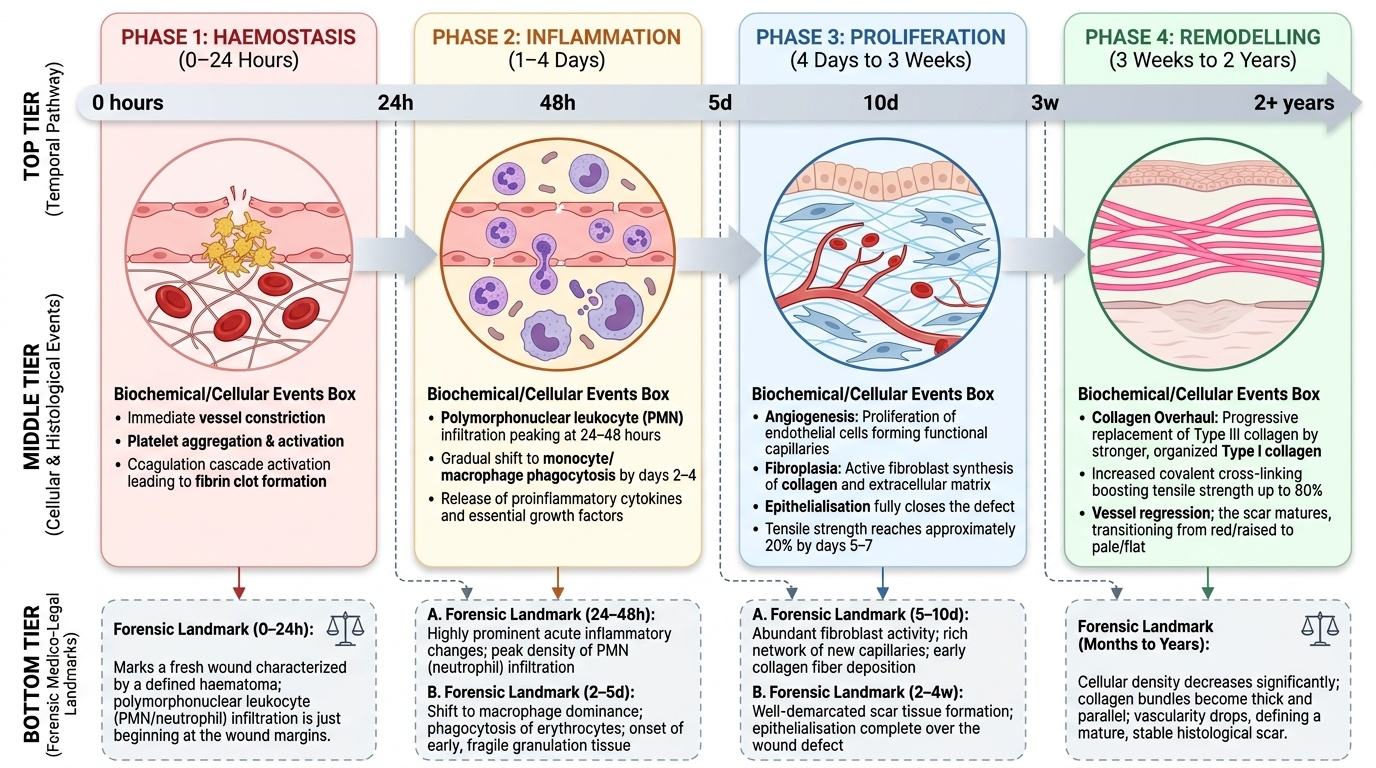
Wound healing proceeds through a sequence of overlapping phases that are well-characterised in pathology and have specific forensic dating applications. The three modes of wound closure — primary intention, secondary intention, and tertiary (delayed primary) intention — differ in whether wound edges are approximated and determine the rate and quality of healing.
Primary intention healing occurs when a wound is clean, with opposed edges (sutured surgical wound or a narrow incised wound), minimal contamination, and adequate blood supply. Healing is rapid, with minimal scar formation. The phases are: haemostasis (minutes to hours — platelet plug, fibrin clot), inflammation (1–4 days — PMN infiltration peaks at 24–48 hours, giving way to macrophages by day 2–4), proliferation (day 4 to approximately 3 weeks — fibroblasts synthesise collagen, epithelialisation is complete within 24–48 hours for a closed wound, tensile strength increases to approximately 20% of normal by day 5–7 and 80% of final strength by 6 weeks), and remodelling (3 weeks to up to 2 years — type III collagen is progressively replaced by type I collagen, cross-linking increases, scar matures from red and raised to pale and flat).
Secondary intention healing applies to wounds where edges cannot be approximated — open lacerations, contaminated wounds, wounds with tissue loss. Healing occurs by granulation tissue formation from the base and edges of the wound, which contracts (wound contraction by myofibroblasts) and is eventually covered by epithelium migrating from the edges. This process is slower and produces a larger scar. The same cellular sequence applies, but the proliferative phase is more prominent and prolonged.
Tertiary (delayed primary) intention involves deliberately leaving a wound open for 4–5 days (to allow decontamination and to ensure no infection) before surgical closure. This is used for heavily contaminated wounds.
For medico-legal purposes, the critical dating landmarks from Reddy's are:
- 0–24 hours: fresh wound, haematoma present, PMN infiltration just beginning
- 24–48 hours: acute inflammatory changes prominent, PMN peak
- 2–5 days: macrophage infiltration, early granulation tissue
- 5–10 days: fibroblast activity, new capillaries, early collagen
- 2–4 weeks: scar formation, epithelialisation complete in secondary intention
- Months to 2 years: scar maturation and remodelling
Provided image
SELF-CHECK
At autopsy, a wound on the right leg shows moderate macrophage infiltration, early fibroblast activity, and beginning collagen deposition with no significant scar formation. Approximately when was this wound most likely inflicted?
A. Within 1–6 hours of death
B. 2–5 days before death
C. 2–4 weeks before death
D. More than 6 months before death
Reveal Answer
Answer: B. 2–5 days before death
The combination of macrophage infiltration (replacing the early PMN phase), early fibroblast activity, and beginning collagen deposition without significant scar corresponds to the transition between the acute inflammatory and early proliferative phases — approximately 2–5 days. PMN-dominated wounds suggest 24–48 hours; mature scar formation suggests weeks; scar remodelling suggests months to years.
Bone Fracture Healing: Medico-legal Significance and Radiological Timelines
Bone fracture healing follows a sequence that is distinctly different from soft tissue healing, and its radiological appearances over time are of direct medico-legal value in estimating the age of a fracture when the victim is unable to provide a history or when the history is disputed. Per Reddy's, the stages and their approximate timelines are well-established reference points for forensic reporting.
Stage 1 — Haematoma formation (within 24–48 hours of fracture): Blood from torn vessels in the periosteum and marrow fills the fracture gap. No radiological change is visible at this stage beyond the fracture line itself.
Stage 2 — Soft callus/fibrocartilaginous callus (approximately 2–6 weeks): Granulation tissue replaces the haematoma; periosteal osteoprogenitor cells and mesenchymal cells from marrow form fibrocartilage bridging the fracture gap. At 2–3 weeks, early periosteal new bone formation becomes visible on X-ray as a fuzzy density alongside the fracture site. This is the first radiological sign that a fracture is undergoing active repair, indicating an age of approximately 2–3 weeks or more.
Stage 3 — Hard callus/woven bone formation (approximately 6–12 weeks): The fibrocartilage callus is replaced by woven bone. On X-ray, the callus bridge is clearly visible as a bony density bridging the fracture gap; the fracture line may still be partly visible. The bone is structurally united but not yet mature.
Stage 4 — Remodelling to lamellar bone (1–2 years, age and bone size dependent): The woven bone is progressively replaced by mature lamellar bone under the influence of mechanical stress (Wolff's law). The callus becomes less prominent, and in children the bone may eventually appear near-normal on imaging.
The medico-legal application of these timelines is most commonly required when: (a) a suspected non-accidental injury (child abuse) involves old fractures in various stages of healing; (b) a victim claims a recent injury but X-ray shows advanced callus formation suggesting an older fracture; or (c) a body is found and fractures must be dated to establish perimortem vs ante-mortem timing. In child abuse cases, the presence of multiple fractures at different stages of healing on a single skeletal survey is a cardinal radiological sign that the injuries are non-accidental and occurred on different occasions.
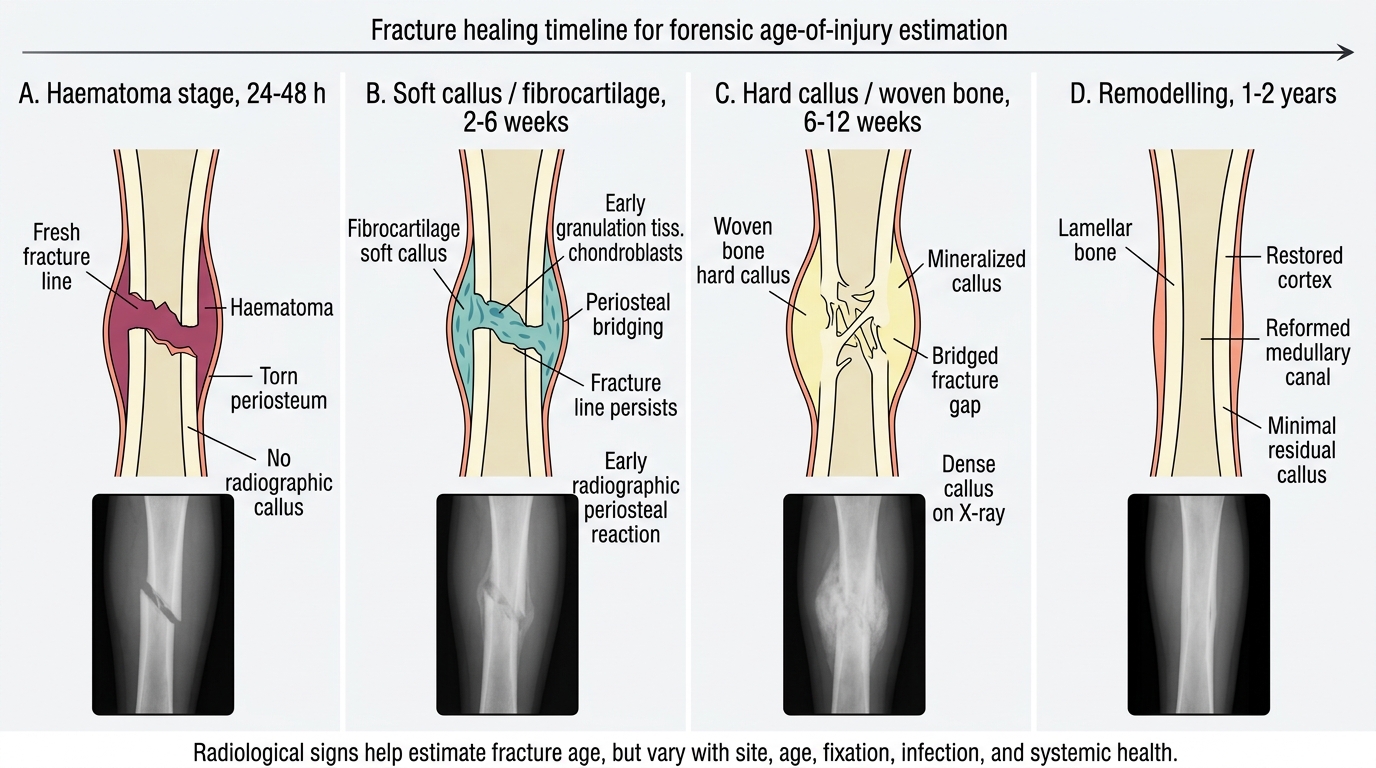
Radiological Timeline of Fracture Healing