Page 5 of 18
FM10.19 | Consent in Medical Practice — SDL Guide
Learning Objectives
- Define consent and articulate its basis in autonomy and battery law
- Classify the types of consent: implied, expressed (oral and written), and informed
- List the essential ingredients of valid informed consent
- Apply the rules of consent in special situations — age, emergency, mental illness, and alcohol intoxication
- Identify the medico-legal consequences of operating without valid consent
INSTRUCTIONS
Consent is the legal and ethical cornerstone of every clinical intervention. Performing any examination or treatment without valid consent — regardless of medical necessity or good intention — constitutes battery in law. Understanding consent protects patients' autonomy and protects clinicians from criminal and civil liability. FM10.19 addresses both the doctrine and its application in the complex real-world scenarios you will encounter as a practitioner.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl presents to a gynaecology outpatient clinic with a 10-week pregnancy. She requests a termination under the Medical Termination of Pregnancy Act. She has come alone and explicitly requests confidentiality — she does not want her parents informed. The treating gynaecologist is uncertain: can a 16-year-old consent to her own termination? Does the MTP Act require parental consent? Is the doctor legally exposed if she proceeds without informing the guardian?
In a separate bay, a 45-year-old man brought in unconscious following a road traffic accident requires emergency laparotomy. No family is present and no advance directive exists. The surgical registrar needs to act immediately.
How does consent law handle these two diametrically different scenarios? What are the rules, and what are the legal consequences of getting them wrong?
WHY THIS MATTERS
Consent is not merely a signature on a form — it is a legal transaction and an expression of patient autonomy that, when absent, exposes the practitioner to civil liability for battery (intentional unconsented touching), a negligence claim (failure to disclose material risks), and potential criminal liability. Indian courts have consistently upheld that patients have a fundamental right to determine what happens to their bodies, derived from Article 21 of the Constitution (right to life and personal liberty). In practical terms, failures of consent — performing a procedure without it, or performing without disclosure of material risks — are among the commonest grounds for consumer forum complaints against clinicians.
RECALL
Recall from prior FM and ethics sessions:
- Battery — the intentional, unlawful touching of another person without consent; a tort and potentially a criminal offence under IPC.
- Autonomy — the bioethical principle that competent individuals have the right to make decisions about their own healthcare.
- Competence vs capacity — competence is a legal term; capacity is the clinical term; a person lacks capacity if they cannot understand, retain, weigh, or communicate a decision about treatment.
- Indian Majority Act 1875 — the default age of majority in India is 18 years.
- MTP Act 1971 amended 2021 — governs termination of pregnancy; the 2021 amendment extended gestational limits for specific categories.
Consent: Legal and Professional Context
Consent in medical law is the voluntary agreement by a person with the mental capacity to make an informed decision, to permit an act to be done upon their body by another. Its legal basis is threefold: (1) the common law principle that every person has the right to bodily integrity and autonomy; (2) the law of torts (battery = unconsented touching); and (3) contract — the doctor–patient relationship may be viewed as a contract requiring the patient's agreement to treatment.
The Supreme Court of India affirmed in Samira Kohli v Dr Prabha Manchanda (2008) that performing an operation — even a beneficial one — without valid consent constitutes a battery. In that case, a doctor performed a hysterectomy and bilateral salpingo-oophorectomy while the patient was under anaesthesia for a diagnostic laparoscopy; the court held that the patient's pre-operative consent for a diagnostic procedure did not extend to the radical treatment performed without regaining consent.
Consent must satisfy four essential attributes to be valid:
1. Voluntary — free from coercion, duress, undue influence, or fraud.
2. Informed — given with adequate knowledge of the nature, purpose, material risks, alternatives, and consequences of refusal.
3. Capacity — the patient has the requisite cognitive and legal capacity to consent.
4. Specificity — the consent covers the actual intervention performed; blanket or general consents that purport to cover 'anything the doctor decides' are legally questionable.
The legal framework for consent in India draws from: the Indian Majority Act 1875 (age of majority), the Mental Healthcare Act 2017 (consent for persons with mental illness), the MTP Act 1971 amended 2021 (termination of pregnancy), and the Transplantation of Human Organs and Tissues Act 1994 (amended 2014) (organ donation consent).
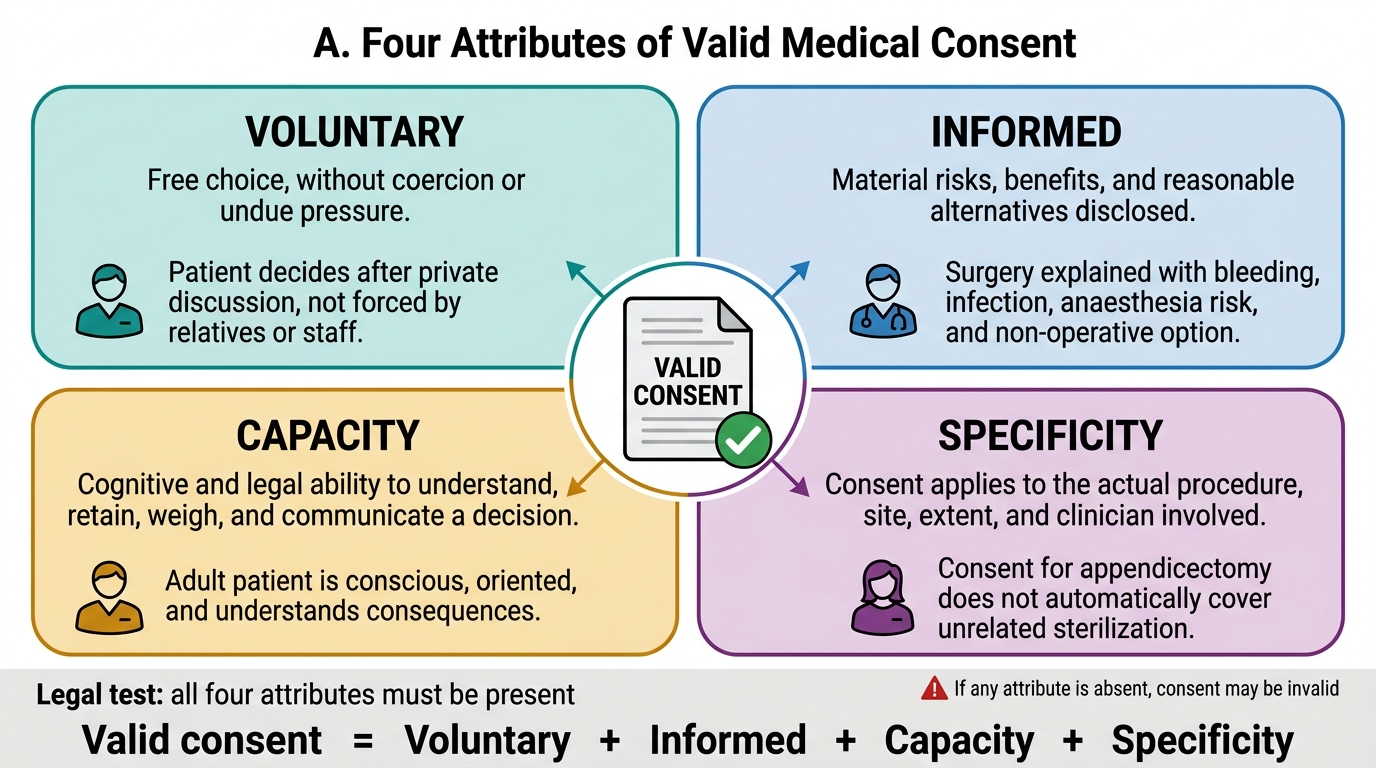
Four Attributes of Valid Consent
Types of Consent
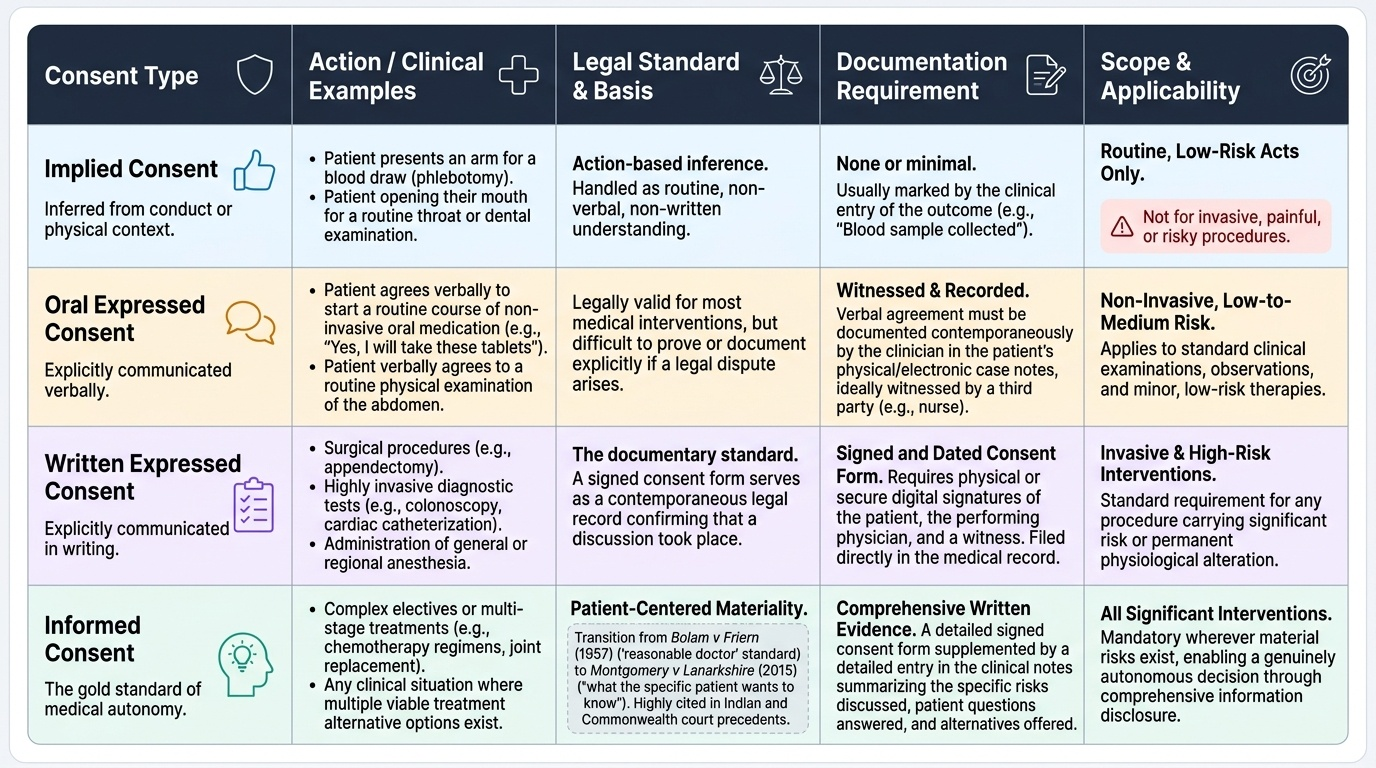
Consent in medical practice takes several forms depending on the nature of the clinical encounter, the intervention contemplated, and the patient's circumstances. Each type has distinct legal significance and different documentation requirements.
Implied consent is inferred from the patient's conduct or the context of the encounter without explicit verbal or written communication. A patient presenting an arm for phlebotomy, or opening their mouth for a throat examination, is taken to have implicitly consented to those specific, routine, low-risk acts. Implied consent does NOT extend to invasive, painful, or risky procedures, and courts have consistently refused to allow implied consent as a defence for complex interventions.
Expressed consent is explicitly communicated by the patient — either orally or in writing. Oral expressed consent is legally valid for most medical interventions but practically difficult to document; it should be witnessed and recorded in the case notes. Written expressed consent is the documentary standard for surgical procedures, invasive investigations, anaesthesia, and any intervention carrying significant risk; the signed consent form creates a contemporaneous record that the consent discussion occurred.
Informed consent is the highest standard of consent and is the legally required standard for all significant medical interventions. It goes beyond mere agreement — it requires disclosure of material information so that the patient can make a genuinely autonomous decision. Following Bolam v Friern (1957) and subsequently the landmark UK case Montgomery v Lanarkshire Health Board (2015) — which Indian courts have begun to cite — the test for adequate disclosure is what the particular patient would want to know (patient-centred materiality), supplemented by what a reasonable patient in that position would want to know, and any risk the patient has specifically asked about. This has effectively broadened the duty of disclosure beyond the older 'reasonable doctor' test.
Provided image
Ingredients of Valid Informed Consent
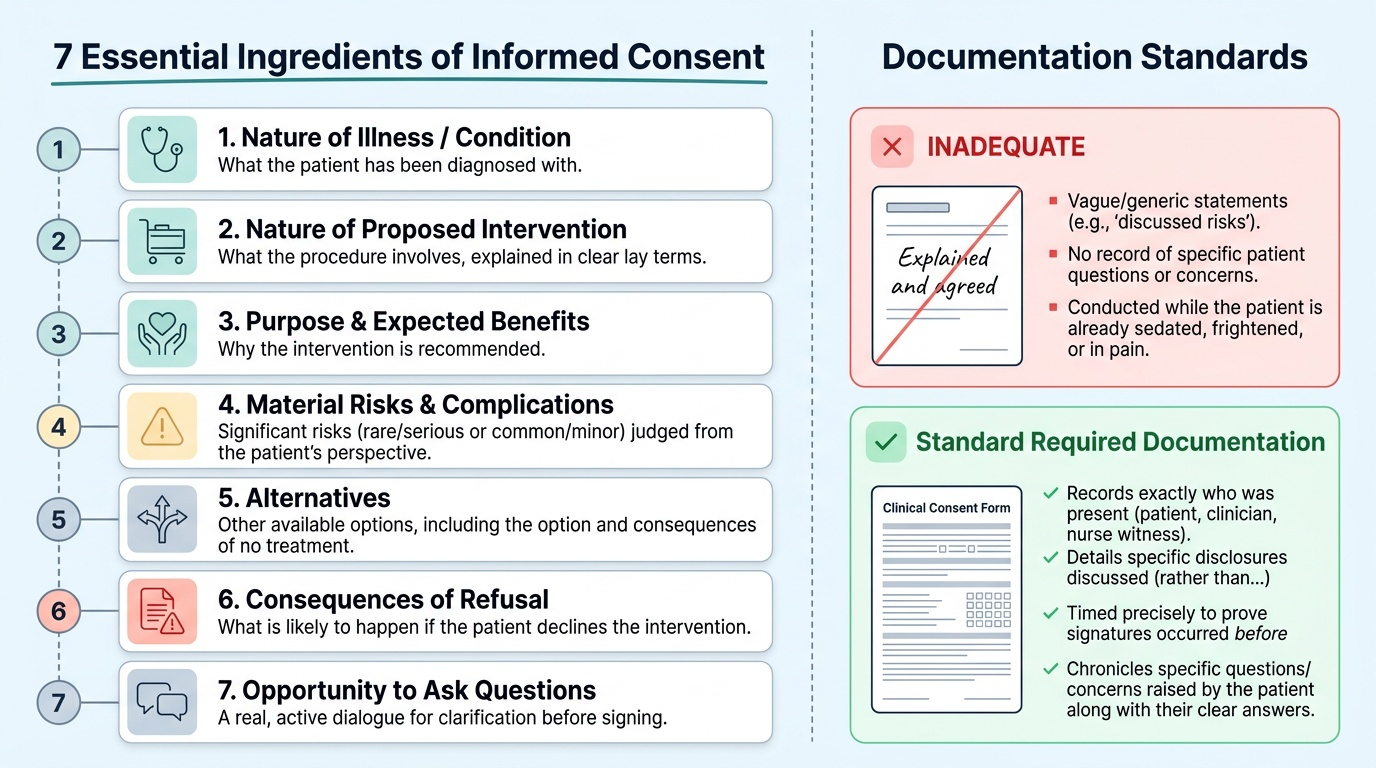
For consent to qualify as informed consent, the following elements must be communicated to the patient in language they can understand, before the intervention begins (not while the patient is already sedated, frightened, or in pain).
The seven essential ingredients of informed consent are:
1. Nature of the illness/condition — what the patient has been diagnosed with.
2. Nature of the proposed intervention — what the procedure involves, in lay terms.
3. Purpose and expected benefits — why the intervention is recommended.
4. Material risks and complications — all significant known risks, including those that are rare but serious (e.g., death under anaesthesia), and those that are common even if minor (e.g., bruising). Materiality is judged from the patient's perspective.
5. Alternatives — other treatment options available, including the option of no treatment and its consequences.
6. Consequences of refusal — what is likely to happen if the patient declines the recommended intervention.
7. Opportunity to ask questions — the patient must be given a real opportunity to seek clarification and have their questions answered before signing.
Documentation of consent must record who was present at the consent discussion, what was disclosed (a consent form that merely says 'explained and agreed' is inadequate), when the consent was given, and any specific questions or concerns raised by the patient. Witnessing the consent by a nurse or third party provides independent corroboration that the discussion occurred.
Provided image
SELF-CHECK
A 30-year-old man is scheduled for laparoscopic cholecystectomy. The surgeon explains the procedure but does not mention the 0.3–0.6% risk of common bile duct injury. A bile duct injury occurs. The patient sues for lack of informed consent. Which TEST, as applied by Indian courts, best determines whether the surgeon had a duty to disclose this risk?
A. Whether any reasonable doctor would have disclosed this risk (the old Bolam disclosure standard)
B. Whether this patient and/or a reasonable patient in their position would consider this risk material to their decision
C. Whether the risk was greater than 1%
D. Whether the patient specifically asked about complications
Reveal Answer
Answer: B. Whether this patient and/or a reasonable patient in their position would consider this risk material to their decision
The modern standard for informed consent disclosure — increasingly applied by Indian courts following Montgomery v Lanarkshire Health Board (2015) — is patient-centred materiality: whether this patient, and a reasonable patient in their position, would have considered the information material to their decision. A 0.3–0.6% risk of common bile duct injury requiring major re-surgery is almost certainly material by this standard. The older Bolam disclosure test (whether reasonable doctors disclose it) is no longer the sole criterion. Merely asking about it is not required by the patient — it is the doctor's duty to volunteer material risks.